
Abstract
The question of how urbanisation and poverty are linked in sub-Saharan Africa is an increasingly pressing one. The urban character of the HIV epidemic in sub-Saharan Africa exacerbates concern about the urbanisation–poverty relationship. Recent empirical work has linked urban poverty, and particularly slum residence, to risky sexual behaviour in Kenya’s capital city, Nairobi. This paper explores the generalisability of these assertions about the relationship between urban poverty and sexual behaviour using Demographic and Health Survey data from five African cities: Accra (Ghana), Dar-es-Salaam (Tanzania), Harare (Zimbabwe), Kampala (Uganda) and Nairobi (Kenya). The study affirms that, although risky behaviour varies across the five cities, slum residents demonstrate riskier sexual behaviour compared with non-slum residents. There is earlier sexual debut, lower condom usage and more multiple sexual partners among women residing in slum households regardless of setting, suggesting a relatively uniform effect of urban poverty on sexual risk behaviour.
Introduction
Simultaneously the fastest-urbanising continent and the one most devastated by the HIV pandemic (United Nations, 2005; UNAIDS, 2006), the question of how urbanisation, poverty and sexual risk behaviour are linked in sub-Saharan Africa is an increasingly pressing one. Urbanisation in Africa is unprecedented in its effects on poverty and health outcomes as, unlike other regions, urbanisation is not accompanied by falling poverty rates or improved health care. Instead, urbanisation has occurred in the absence of economic growth, thereby intensifying poverty levels among the expanding urban population (Brockerhoff and Brennan, 1998; Fay and Opal, 2000; Dodoo et al., 2007). The rapid urbanisation and growth of urban slum settlements in sub-Saharan Africa present cause for significant concern, particularly given their association with sexual risk and HIV. However, it remains unclear whether the link between urban poverty and sexual risk is generalisable to all urban settings in the region, or whether previous findings are primarily pertinent to specific nations and cities. This paper examines the relationship between slum residence and risky sexual behaviour across five African cities that reflect varying degrees of urban poverty and other relevant characteristics.
Recent empirical work has causally linked urban poverty in the US to sexual risk behaviour such as lower age at first sex, less contraceptive use and more sexual partners (Billy et al., 1994; Brewster, 1994; Brewster et al., 1993; Browning et al., 2005). This pattern also extends to sub-Saharan Africa, including Kenya’s capital city, Nairobi (Zulu et al., 2002, 2003; Dodoo et al., 2003, 2007). However, that body of work begs the question of whether these findings are unique to Nairobi, given its particularly high proportion of residents (roughly two-thirds) who live in slums (Zulu et al., 2003; UN-HABITAT, 2006). Of primary concern is whether other cities across the continent exhibit a similar relationship between urban poverty and sexual risk behaviour, or whether the earlier findings are uniquely a Nairobi phenomenon. The answer to this question has implications for the type of interventions that can be used to address the rapid spread of HIV in these regions.
Africa and Urbanisation
By the end of 2008, for the first time more than half of the human population resided in urban areas, with the urban population in Asia and Africa expected to double between 2000 and 2030 (UNFPA, 2007). No world region is currently urbanising faster than Africa and, while urbanisation that occurred in most other regions frequently coincided with rapid economic growth, this has not been the case for the continent (Fay and Opal, 2000; United Nations, 2005). This expansion of the urban population during a period of economic stagnation has resulted in the growth of impoverished slum settlements. Thus, the general urban advantage in health outcomes seen across the world is not evident in Africa (Montgomery and Hewett, 2004), which is simultaneously burdened with the highest levels of HIV/AIDS. The HIV pandemic has soared in sub-Saharan Africa, which contains two-thirds of those infected with HIV world-wide (UNAIDS, 2006). 1
While urban slum residence and HIV have become increasingly intertwined, scholarly work on urban poverty has been undermined by the unavailability of data in a field where hitherto the principal focus has been on rural areas. The dialogue about urban poverty, slum residence and demographic and health outcomes advanced appreciably with Zulu et al.’s (2002) coining of a proxy measure for slum residence that allowed existing Demographic Health Survey (DHS) data to be applied to the study of urban poverty. That paper documented the effect of slum residence on sexual behaviour in Nairobi and found that slum residents were vulnerable to reproductive health risks. Dodoo et al. (2007) continued the dialogue by addressing the ensuing question of whether the disadvantage found by Zulu et al. (2002) was truly an urban poverty effect or simply one generally of poverty. Their comparison of rural and urban contexts reinforced the argument for a unique impact of urban poverty vis-à-vis adverse sexual outcomes. A logical next question regards whether the cumulative findings of these two papers represent a uniquely Kenyan phenomenon, or whether the urban poverty effect is generalisable to other cities on the continent most exacerbated by the HIV virus. We test the consistency and strength of the empirical relationship between urban poverty and risky sexual behaviour with comparable data from five African cities: Accra (Ghana), Dar-es-Salaam (Tanzania), Harare (Zimbabwe), Kampala (Uganda) and Nairobi (Kenya).
Risky Behaviour and the Slum Environment
There are various reasons why impoverished settlements may heighten risk behaviour, including local opportunity structure and resources. High unemployment rates and low wages in these urban areas make women vulnerable to risky behaviour, coercing them to exchange sex for money and to have multiple partners in order to supplement income, all of which increases the likelihood of exposure to HIV infection (Krishnan et al., 2008; Zulu et al., 2003). Messages about the local opportunity structure impact risky behaviour, as residents who perceive or experience greater opportunities will be more likely to avoid behaviour that will reduce their chances of success due to disease or unwanted pregnancy (Billy and Moore, 1992; Brewster et al., 1993; Driscoll et al., 2005; Krishnan et al., 2008; Wilson, 1987, 1991). Further, impoverished communities frequently lack vital resources, such as schools and medical facilities, that encourage health-promoting behaviour (Leventhal and Brooks-Gunn, 2000).
Residence in urban slum communities also heightens exposure to social and cultural factors that encourage risky behaviour. Weakened social networks in such communities undermine collective efficacy, reducing neighbours’ supervision and monitoring of risky behaviour (Sampson, 1997; Skogan, 1990; Woldoff, 2002; Wilson, 1987). The social isolation prevalent in disadvantaged neighbourhood environments further shields residents from the taboo of destructive behaviour. A contagion model also suggests that residents in disadvantaged neighbourhoods adopt risky behaviour from surrounding peers (Leventhal and Brooks-Gunn, 2000; Wilson, 1987).
General findings about sexual risk and urban poverty will not benefit the formation of successful policies and interventions if significant variations in patterns do exist across contexts. There are noteworthy differences in the urban environments across the five cities we selected, as well as in the countries that house them. Zimbabwe’s capital Harare has the lowest prevalence of slum residence among its urban residents, followed by Ghana’s capital Accra and Kenya’s capital Nairobi, with Tanzania’s Dar-es-Salaam and Uganda’s Kampala exhibiting the highest incidence of slum residence (UN-HABITAT, 2003). Ghana has the highest percentage of residents living in urban areas (49 per cent), compared with Zimbabwe (37 per cent), Tanzania (25 per cent), Kenya (21 per cent) and Uganda (13 per cent). Regarding national poverty, Kenya and Ghana show the lowest rates of overall poverty among the five countries (23 per cent and 45 per cent respectively), relative to Zimbabwe (56 per cent), Tanzania (58 per cent) and Uganda (85 per cent) (UNFPA, 2007).
Given these differences between the five cities and countries along these traits, as well as various cultural and social characteristics, a discovery of a relatively uniform influence of urban poverty on risky behaviour would strengthen the notion that the effect of urban poverty is resilient across residential contexts and not highly responsive to variations in other contextual factors.
Data and Methods
The availability of standardised, nationally representative Demographic and Health Survey (DHS) data for most African countries permits this analysis. Although DHS data employ country census frames, they, unfortunately, do not oversample urban areas. Similarly, they do not include slum identifiers. We restrict our analysis to the capital cities of the selected countries because, without actual slum identifiers, we lean on the proxy measure first proposed by Zulu et al. (2002) to identify slum households. As we shall describe, the proxy measure only has face validity in large metropolises. Slum households are identified by the simultaneous absence of three basic household amenities: electricity, flush toilets and running water piped into the home; 2 households with all three are deemed to not be in slums. 3 We must note that residence in slums is not necessarily synonymous with household poverty, as slums exhibit heterogeneity in the socioeconomic status of their residents (UN-HABITAT, 2003).
The proxy measure, which only has face validity in the largest cities in Africa, enables the investigation of intraurban differences in the comparison of slum and non-slum households. Although it is reasonable to classify any household in a major metropolis, such as the capital city of any African country, that lacks all three of these basic amenities as likely to be located in a slum, it would be difficult to make the same extrapolation to rural settings. In capital cities, political and economic influences definitively dictate that supply of amenities exists, whereas in rural areas and even smaller towns, the absence of, for instance, electricity may simply be due to political or administrative constraints (Zulu et al., 2002). Thus, the nature of the proxy dictates that we limit analysis to such metropolises, as the measure may not be as valid in smaller towns and villages.
We focus on women for a number of reasons. Women comprise a rapidly growing segment of the HIV-infected population world-wide and are particularly likely to have higher infection rates than men in sub-Saharan Africa (UNAIDS, 2006). This is due in part to their greater vulnerability to factors that heighten risky sexual behaviour and consequently HIV, including barriers to educational attainment and economic dependence on men that diminishes their ability to refuse sex or negotiate safer sex (Kim et al., 2008). Gender-based norms further limit women’s sexual decision-making in relationships (Kim et al., 2008; Krishnan et al., 2008).
The DHS gathers data for women aged 15–49, and we focus on surveys from each of five countries: Ghana (2008), Kenya (2003), Tanzania (2004), Uganda (2006) and Zimbabwe (2005). The slum selection criteria translate into samples from Accra, Nairobi, Dar-es-Salaam, Kampala and Harare of 616, 1120, 385, 781 and 1350 respondents respectively. Three measures that have bearing on the spread of HIV comprise the dependent variables of interest. These variables, which reflect risky sexual behaviour, are age at first sexual intercourse, multiple sexual partnerships and condom use during last sexual intercourse. All respondents were asked their age at first sexual intercourse. This is a duration variable that allows assessment of the risk or hazard of sexual initiation, which calls for survival analysis. Further, women were asked the following question: “In the last 12 months how many different persons (other than your husband/man you are living with) have you had sexual intercourse with?” This question allows us to derive the number of sexual partners women had in the preceding year. Finally, we examine the non-use of condoms during the last sexual encounter using the binary measure of condom use: non-use scored ‘0’ and use scored ‘1’.
We first explore the pattern of attrition based on age at first sexual intercourse, taking only those who are life-long slum residents or who report being virgins when they arrived in the slum they were interviewed in. We run Cox proportional hazard models based on residence type (slum and non-slum), city (Accra, Dar-es-Salaam, Harare, Kampala and Nairobi) and the city–residence type interaction. Statistically insignificant interactions between city and residence type would suggest uniform behaviour across cities. A total of five city–residence dummies are derived from the interaction of cities (Nairobi, Accra, Dar-es-Salaam, Kampala and Harare) and residence (slum and non-slum). The final model incorporates control variables, including religion (Christians, others), age and years of education. This model will allow us to study the residence–city effect after controlling for other factors, enabling us to explore hypotheses about the uniformity of urban poverty effects.
We use ordinary least squares regression to analyse multiple sexual partnerships and logit models to study the binary condom use outcome during last sexual intercourse, employing the same five analyses plan described earlier. Beyond religion, age and years of education, we also control for length of stay in current residence, marital status (currently married, divorced, widowed, never married), sex of the household head and employment status (employed, unemployed) in the final model.
We recognise the limitations in examining self-reported sexual behaviour, as individuals may not provide honest answers given the sensitive nature of the topic. Further, memory recall may pose concerns, as some women may not recall their precise age at first intercourse or number of sexual partners over a particular time-period. However, DHS addresses these concerns by using local calendars to prompt individuals about events. Further, while in each country we expect more accurate reporting in non-slum settings, there is little to suggest that the reporting quality difference between slums and non-slums will vary across countries. Thus, we do not anticipate any systematic biases across countries that would compromise our findings regarding the generalisability of the urban poverty effect.
Results
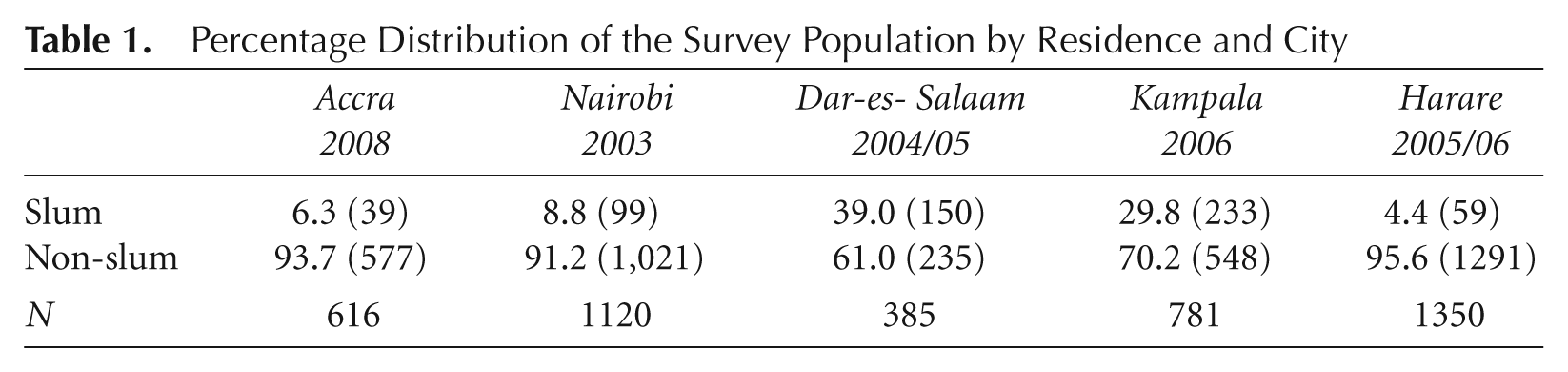
The pooled data covered a total of 1354 female respondents between ages 15–49 across the five cities. Among them, 13.6 per cent belonged to slum households and 86.4 per cent to non-slum households. Disaggregating across cities evidences vastly different proportions of respondents in slums across cities. Table 1 indicates that approximately a third of Kampala and Dar-es-Salaam respondents live in slums, while only 4.4 per cent, 6.3 per cent and 8.8 per cent of those in Harare, Accra and Nairobi do respectively.
Percentage Distribution of the Survey Population by Residence and City
Age at First Sexual Intercourse
Table 2 presents the survival analysis for women who were virgins when they moved into the slum. Among these respondents, slum residence in strongly linked to risky sexual behaviour. Overall, 47 per cent of women in slums are still virgins at age 16, meaning that a majority (53 per cent) have already had sexual intercourse by that age. Conversely, in non-slum households, not even a third of the female population has done so by age 16. Even by age 18, less than half of non-slum women have had intercourse, while in slums, only 19 per cent of 18-year-olds remain virgins.
Life table survival proportions for age at first sex, by residence and age
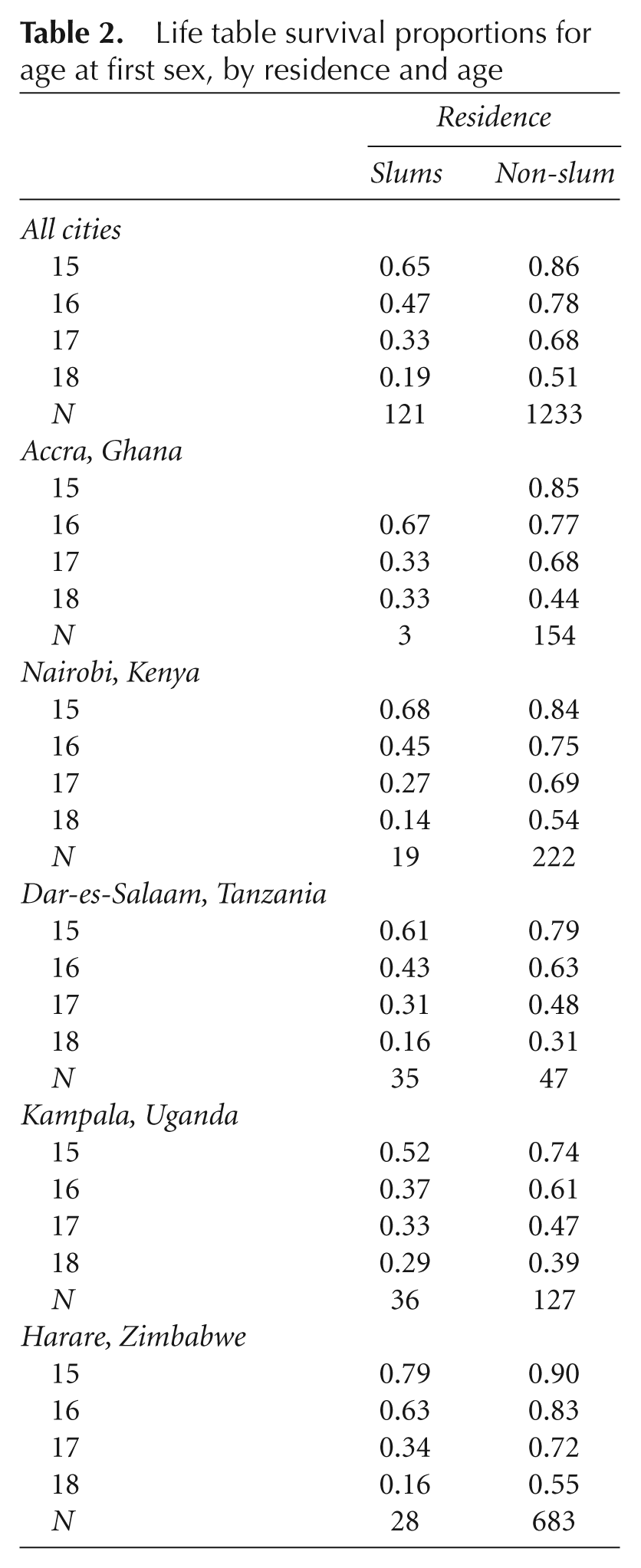
Interestingly, there are differences in sexual behaviour by type of residence and country. Among slum residents, women in Harare and Accra are more likely to show delayed entry into sexual activity, with the 50 per cent threshold surpassed by age 17 in both countries, which is a full year later than the slum residents of Nairobi, Dar-es-Salaam and Kampala. However, regarding non-slum women, it is only in Harare and Nairobi that a majority has avoided sexual intercourse by age 18. Among non-slum women, those in Kampala show the most rapid entrance into sexual activity. Based on these results alone it appears that, across contexts, slum residence does not uniformly affect entry into sexual activity.
Table 3 presents the coefficients and hazard rate from Cox proportional hazard models. Model 1 confirms that sexual activity starts later in non-slum compared with slum settings, with a coefficient of −0.80. Model 2 shows that, relative to Nairobi residents, those living in Dar-es-Salaam and Kampala start sexual activity earlier, whereas those in Accra and Harare are not significantly different. Model 3 simultaneously confirms both the slum disadvantage and the variations in sexual activity across the cities evidenced in model 2.
Coefficient and hazard rate from Cox proportional hazard models: effect of residence on age at first sex for women
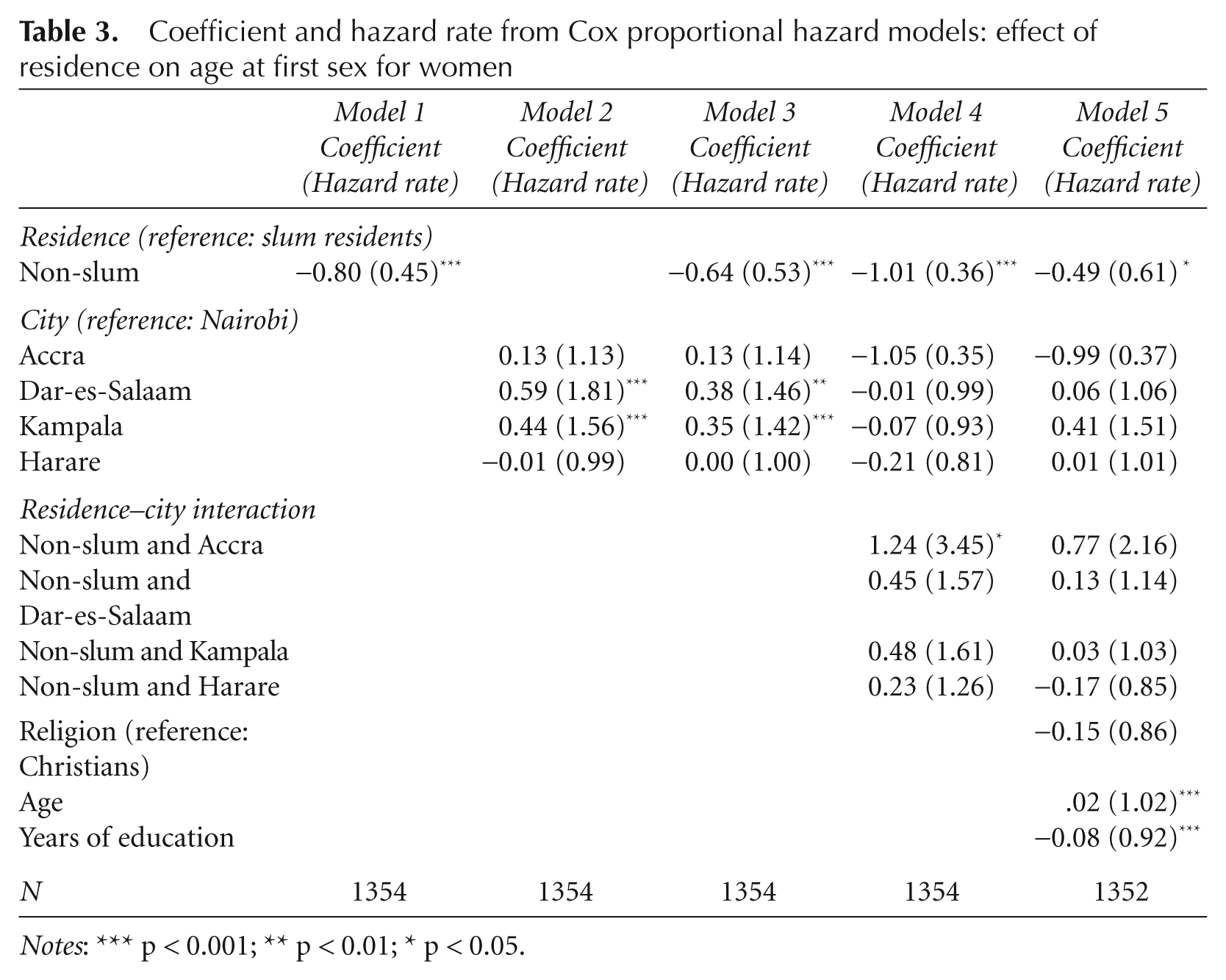
Notes: *** p < 0.001; ** p < 0.01; * p < 0.05.
Model 4 introduces interaction terms for city and residence type in order to test the generalisability of urban poverty effects. Three of the four interaction terms are not significantly different from the omitted category that is the Nairobi/slum interaction and the one significant interaction term pertains to Accra and specifically non-slum residents of Accra. Once controls are introduced in model 5, the effect of slum residence in these countries does not vary significantly relative to Nairobi residents, even in the face of the selected control variables.
Condom Use during Last Sexual Intercourse
Table 4 presents the effect of slum/non-slum residence on condom use at last sexual intercourse. Because the dependent variable is binary in nature, we present the odds ratios from the logit model. Contrary to the age at sexual debut findings presented in Table 3, model 1 of Table 4 initially suggests that slum residence may not be a significant predictor of risky behaviour. However, model 2 shows that residents of Accra, Dar-es-Salaam and Kampala are significantly more likely to use condoms in their sexual encounters relative to those in Nairobi, with coefficients of 1.38, 1.62 and 1.96 respectively, even though Table 3 had demonstrated that women in Dar-es-Salaam and Kampala lose their virginity faster. The next model also shows that, relative to Nairobi women, those in Harare are less likely to use condoms. Interestingly, when both the city and residence type variables are included in model 3, slum residence emerges as a significant predictor of condom usage with a coefficient of 1.83, implying that slum women are more likely to engage in unprotected intercourse. At the same time, net of the effect of slum residence, all four presented cities show significantly higher condom use compared with Nairobi. Overall, it appears that the Nairobi patterns are not precisely in line with those in the other cities.
Effects of residence and other factors on condom use at last sexual intercourse (odds ratios) for women
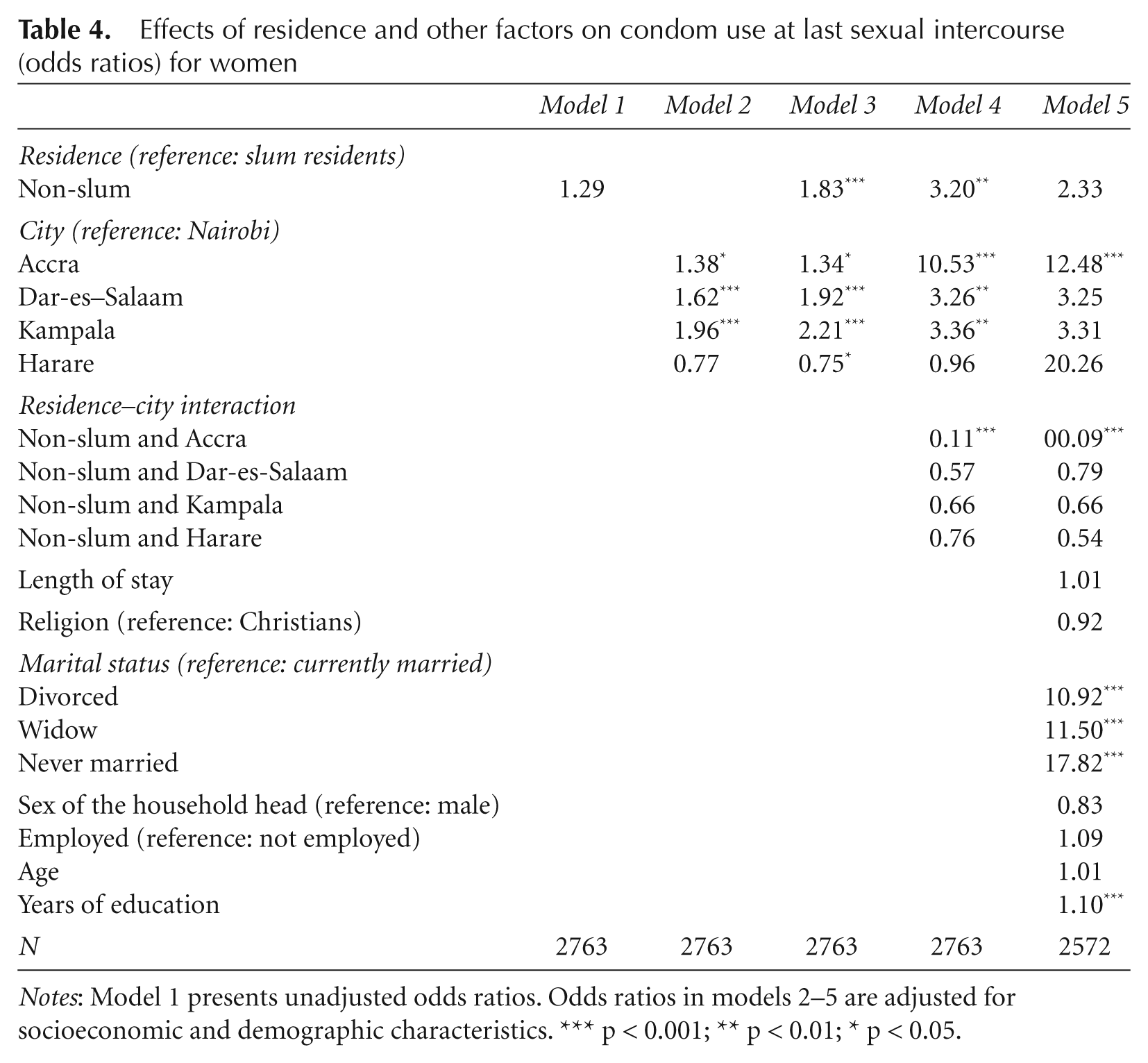
Notes: Model 1 presents unadjusted odds ratios. Odds ratios in models 2–5 are adjusted for socioeconomic and demographic characteristics. *** p < 0.001; ** p < 0.01; * p < 0.05.
The interaction terms in models 4 and 5 indicate that non-slum residents of Accra seemed to be significantly more likely to use condoms at their last sexual encounter. In the case of age at first sex, these results suggest that slum residence poses risk factors for sexual behaviour and that variations in risk exist across the cities, but overall the urban poverty effect is relatively uniform across locations, at least when compared with Nairobi.
Multiple Sexual Partnerships
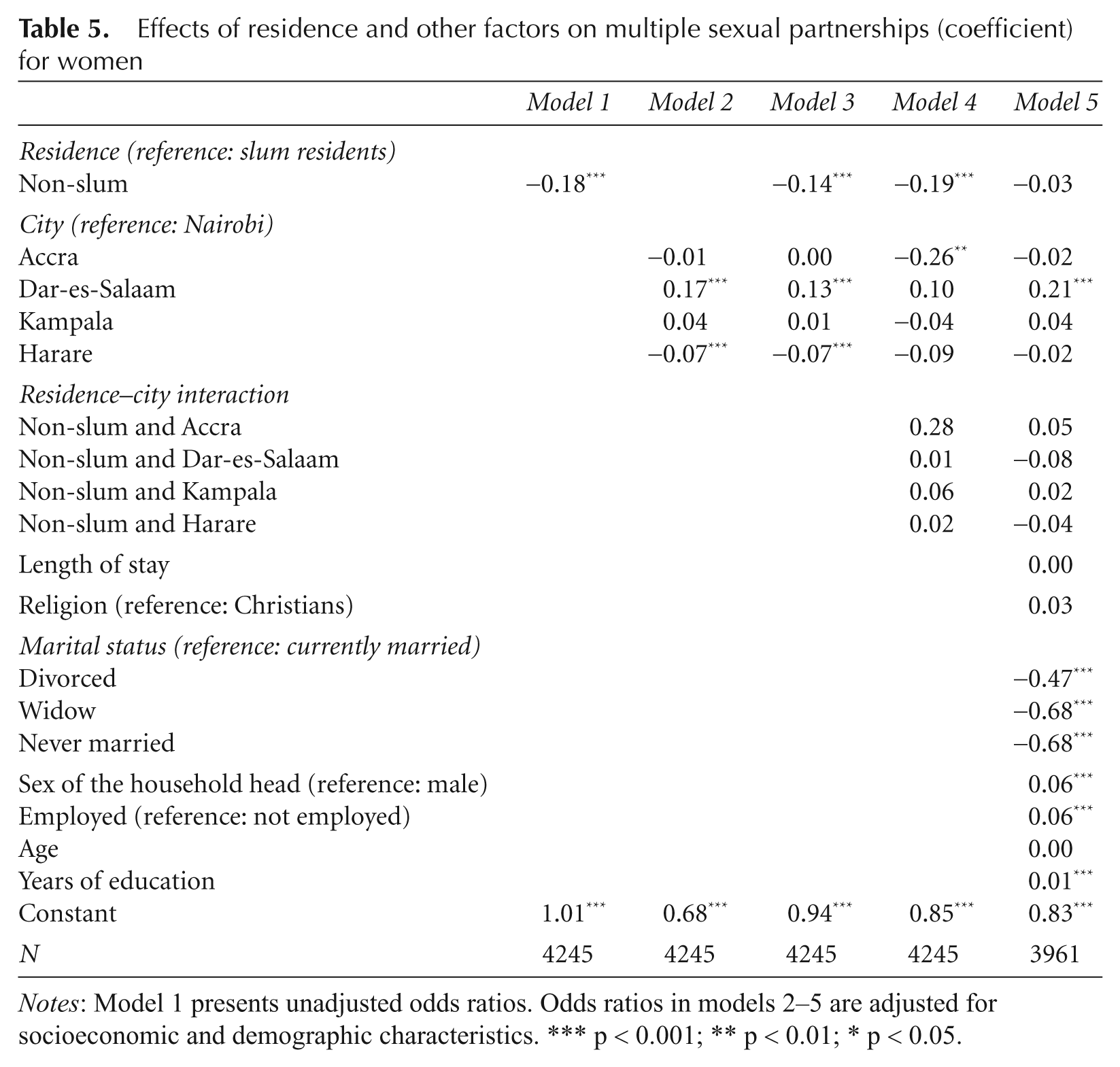
Table 5 employs ordinary least squares regression to examine the relationship between multiple sexual partnerships and residence. Model 1 suggests that non-slum residence is associated with lower multiple partnership, with a coefficient of −0.18. Model 2 shows that, compared with their counterparts in Nairobi, women in Dar-es-Salaam have more sexual partners (coefficient = 0.17), while those in Harare have fewer (coefficient = −0.07). These patterns remain relatively consistent in model 3, underscoring the peculiarity of cities. However, the lack of any significant interaction terms in models 4 and 5 once again implies that slum residence is associated with risk behaviour in a uniform way across the cities.
Effects of residence and other factors on multiple sexual partnerships (coefficient) for women
Notes: Model 1 presents unadjusted odds ratios. Odds ratios in models 2–5 are adjusted for socioeconomic and demographic characteristics. *** p < 0.001; ** p < 0.01; * p < 0.05.
Discussion
Two intentions of the Millennium Development Goals (MDG) are to improve the lives of at least 100 million slum-dwellers by 2020 and to attenuate the spread of HIV/AIDS. This paper addresses the intersection of these two MDGs, insofar as HIV/AIDS is disproportionately an urban phenomenon in sub-Saharan Africa and slum-dwellers constitute a major segment of the urban poor in Africa. Previous studies have generally identified urban poverty effects on risky behaviour. More specifically, a handful of studies concentrating on Nairobi have elucidated the link between slum residence and sexual risk behaviour (Zulu et al., 2002, 2003; Dodoo et al., 2003, 2007). The generalisability of this finding has been in question, particularly given the peculiar size of slums in Nairobi; one of Nairobi’s slums, Kibera, is purportedly the largest slum on the continent with over half a million residents.
For the first time, this paper speaks to the generalisability of the relationship between slum residence and risky sexual behaviour and underscores the urban penalty of risky health outcomes in developing countries. Overall, slum residents demonstrate riskier sexual behaviour compared with non-slum residents. There is earlier sexual debut, lower condom use and a higher incidence of sex with multiple partners among women residing in slum households compared with those living in non-slum settings. However, our findings also demonstrate that risky sexual behaviour, specifically, earlier loss of virginity (i.e. younger sexual debut), lack of condom usage and multiple sexual partnerships are generally invariant across the five city slums. Among all city/residence interactions terms across the three models, only one emerged as statistically significant. Overall, this would suggest a uniform effect of urban poverty on sexual behaviour across the five selected cities.
The robustness of the relationship between urban disadvantage and risky sexual behaviour across cities and countries that differ in their rates of poverty and urbanisation, as well as other economic, political, social and cultural characteristics, is a meaningful result. Entrenchment in urban slums presents a powerful barrier to health-promoting behaviours, regardless of the particular country in which these slums are housed. This suggests that successful policy and programme interventions to address risky sexual behaviour and the spread of HIV in slum settlements may not require context-specific strategies.
More research, both quantitative and qualitative, is necessary to uncover the most compelling factors that are driving the relationship between slum residence and risky behaviour world-wide. Aside from DHS data, there are few comparative studies of urban poverty and sexual risk across continents or between developing and non-developing countries (Harpham, 2009). While impoverished urban areas exist in both developing and industrialised countries, the effect of residence in these areas may depend on whether they are housed in the former or latter. Residents of ghettos or slums in industrialised countries may still benefit from greater national expenditures for education, health, housing and overall social welfare that could diminish the impact of slum residence on risky sexual behaviour (Harpham, 2009). Further, entrenched gender inequalities that limit women’s economic independence in developing countries may render slum women in these areas more vulnerable to transactional sex for survival.
Given the rapid growth of HIV in urbanising African countries, as well as globally in countries such as China that were relatively untouched by the disease until recent years (Zhongdan et al., 2008), cross-national research will continue to be vital in identifying strategies to diminish risky sexual behaviour. The current study has uncovered consistency in the urban poverty penalty across sub-Saharan African countries, although more scrutiny must be directed towards unravelling the mechanisms behind this effect while also acknowledging the potential for regional variations in factors that heighten risk behaviour.
Footnotes
1.
2.
The UN-HABITAT defines a slum household as one that lacks any one of the following five elements: access to improved water, access to improved sanitation, security of tenure, durability of housing and sufficient living area.
3.
Intermediate households with one or two of the amenities do not attract much interpretive attention here.