
Abstract
Violence and traumatic stress negatively affect physical health in youth. Incarcerated adolescents have high rates of violence exposure and health problems, however, few studies have examined medical records and violence exposure in this high-risk population. Self-reported violence exposure and symptoms of stress were collected in 115 incarcerated male adolescents. Medical charts were reviewed for the presence of somatic complaints and chronic health conditions. Regression modeling and odds ratios demonstrated that exposure to intimate partner violence (IPV), child abuse, and sexual abuse predicted specific health conditions. The hierarchical regression model established that traumatic stress and a history of sexual abuse predict cumulative health problems. The study demonstrates that early exposure to violence combined with the presence of traumatic stress symptoms increases the risk for later health problems and can be used by healthcare providers to identify youth at increased risk of long-term health outcomes in high-risk populations.
Keywords
Youth violence exposure (VE) is a major public health concern in the United States. It has far-reaching consequences for individuals, families, and communities (David-Ferdon et al., 2021). VE is known to be associated with negative health outcomes (Bonomi et al., 2007; David-Ferdon et al., 2021; Fredland et al., 2008; Graham-Bermann & Seng, 2005; Griggs et al., 2019; Wright et al., 2016) in both adulthood and during childhood. This confluence between VE and health may be due in part to factors that are associated with both the likelihood of VE and poor health conditions such as pollution and noise (Evans, 2006; Evans & Kantrowitz, 2002). However, a large study of census-level data found that VE uniquely contributes to poor health beyond other neighborhood variables (Beck et al., 2016), which suggests that there may be individual mechanisms that make some children more susceptible to the health effects of VE. Biological theories would argue that the individual-level response to trauma is one potential mechanism.
Early work on the role of adverse childhood experiences (ACE) found that exposure to ACE in childhood is associated with negative health outcomes in adulthood (Felitti et al., 1998). Subsequent research has posed the biological stress response as a mechanism for poor health outcomes following VE. VE triggers a stress response that facilitates a healthy response to the stressor such as running away, often referred to as fight, flight, or freeze (Thompson et al., 2014), however, the body needs to return to a state of calm after the stressor, known as allostasis. Overexposure to stress experiences taxes the ability to return to allostasis and compromises underlying biological mechanisms that allow the shift from heightened arousal when needed back to a state of calm when the stressor disappears (Gunnar & Cheatham, 2003; Meaney, 2001). Repeated overexpression of the stress response is known to have long-term consequences for physical health and to be a precursor to the development of trauma symptoms and PTSD.
Much of the work on VE and health outcomes is retrospective studies of adults with high VE. Incarcerated youth are known to have high rates of VE (Ford et al., 2013; Kimonis et al., 2011; Malvaso et al., 2018) however, the causal relation between trauma symptoms, VE, and health outcomes in adolescent high-risk populations, such as incarcerated youth, is not well understood. Despite evidence that incarcerated youth have very high levels of mental health and educational deficits, which have been reviewed in recent meta-analyses (Chow et al., 2022; Livanou et al., 2019; Steele et al., 2016; Young et al., 2015) there is shockingly little recent work on the physical health problems in incarcerated youth (Butler et al., 2008; Forrest et al., 2000; Golzari et al., 2006; Lader et al., 2003), which leaves open the question of whether the relation between VE and the rate of physical health conditions during adolescence is associated with post-trauma clinical functioning.
Health Studies of Incarcerated Youth
Despite the dearth of research on medical problems in this population, it is clear that incarcerated youth have more physical health problems than the general population (Butler et al., 2008; Feinstein et al., 1998; Forrest et al., 2000; Golzari et al., 2006; Hein et al., 1980; Williams, 2006). One study that used a medical record review and self-reported health survey responses from a random selection of detained youth in Maryland found that 45% of the sample had some medical condition, including allergies, asthma, and high blood pressure (Shelton, 2000). However, the mechanisms of the health problems of incarcerated youth remain unclear.
Violence Exposure and Negative Health Outcomes
The relation between children’s VE and negative physical health outcomes is well-established (Fredland et al., 2008; Friedrich & Schafer, 1995; Golzari et al., 2006; Goodwin & Stein, 2004; Griggs et al., 2019; Wegman & Stetler, 2009; Wright et al., 2016). Epigenetic factors have been shown to alter the rate of biological aging which is known to contribute to long-term health outcomes (Jovanovic et al., 2017), specifically in cardiac health. In a recent population-based study the researchers found that the number of VE is additively a risk for physical health problems (Rueness et al., 2019a). In a recent study, population-level VE was related to childhood rates of asthma treatment and hospitalization after controlling for commonly co-occurring neighborhood problems like poverty and substandard housing (Beck et al., 2016). The presence of health conditions is also linked to community VE, such as increased asthma, cardiometabolic risk, decreased sleep, impaired immune functioning, and dissatisfaction with health (Beck et al., 2016; Griggs et al., 2019; Heissel et al., 2018; Kapur et al., 2022; Landeo-Gutierrez et al., 2019; Miller et al., 2018; Wright et al., 2016).
Literature has linked specific VE (such as physical abuse) with general somatic complaints, cardiac disease, and chronic diseases, including arthritis, asthma, ulcers, obesity, and migraines (Chen et al., 2023; Hilker et al., 2005; Huffhines & Jackson, 2019; Midei & Matthews, 2011; Norman et al., 2012; Rivara et al., 2019; Rueness et al., 2019a; Spitzer, Ewert, et al., 2021; Spitzer, Lübke, et al., 2021; Tietjen & Peterlin, 2011). In Chen et al.’s (2023) meta-analysis of coronary heart disease risk following child abuse, both general exposure to abuse in childhood and specific physical, emotional, or sexual abuse, increased the relative risk of heart disease to 1.5 times the risk of the general population. Childhood abuse is also correlated with negative cardiometabolic health outcomes as adults, with specific outcomes being higher body mass index and higher heart rate, (Soares et al., 2021), obesity (Berens et al., 2017; Mundi et al., 2021), type 2 diabetes (Berens et al., 2017), myocardial infarction (Jacquet-Smailovic et al., 2021), atherosclerosis (Spitzer, Lübke, et al., 2021), and coronary heart disease and stroke (C. Lee et al., 2023).
A major contributor to these health conditions may be the biological cascade of high allostatic load (Rogosch et al., 2011), including cortisol production, brain development, and connectivity in various regions (Aiyer et al., 2014; Cará et al., 2019; Demir-Lira et al., 2016; Goetschius et al., 2020; Peckins et al., 2012). There is some work suggesting that allostatic load leads to chronic inflammation of the neuroimmune network which could lead to both physical and mental health outcomes (Nusslock & Miller, 2016). While informative, these studies are limited in that some assess only one or two types of VE while others do not account for a variety of health problems that children may experience.
Violence Exposure and Traumatic Stress Symptoms
VE has been consistently linked to posttraumatic stress symptoms in children and adolescents (Cook-Cottone, 2004; Haj-Yahia et al., 2019, 2021; Lynch, 2003; Mazza & Reynolds, 1999; Rivara et al., 2019; Rosenthal, 2000). Childhood VE has been shown to modulate the stress response system and the perception of stress (Heinze et al., 2017; Jovanovic et al., 2017; Theall et al., 2016). In one study that demonstrates this connection, adolescents exposed to community violence had higher rates of posttraumatic stress symptomatology, as well as depression and aggression, with proximity to the event related to the degree of PTSD symptomatology (Scarpa, 2003). In a clinic assessing severe behavior problems, the relation between exposure to interparental violence (IPV), aggression, and posttraumatic stress symptoms in adolescents (Moretti et al., 2006) was examined. Moretti found that one-third of the sample met the criteria for posttraumatic stress disorder (PTSD) and the relationship between IPV and aggression was strongest for those adolescents who met the criteria for PTSD.
In a similar study, abused women and their children were assessed for exposure to abuse, symptoms of posttraumatic stress, and adjustment (Graham-Bermann & Levendosky, 1998). Simply being exposed to the abuse of their mother was correlated with symptoms of traumatic stress in the child, and 13% qualified for a PTSD diagnosis. When mothers of at-risk preschoolers in another study were asked to report on both traumatic events that their child had experienced and symptoms of traumatic stress, stress scores were highest for traumatic events that involved family violence and family members, as compared to accidents, death, or more distant traumatic events (Graham-Bermann et al., 2008).
Traumatic Stress and Health Outcomes
Varying stressors, ranging from daily stressors to natural disasters to poverty, have long been identified as a consistent predictor of poor health outcomes in old and young populations (Cobb & Steptoe, 1996; Cohen et al., 1998; Cohen & Williamson, 1991; Coleman et al., 1998; Polick et al., 2022; Surtees & Wainwright, 2007; Taylor et al., 2006). Clinical reactions to stressful events also have been linked to negative physical health outcomes (Irwin et al., 1996; Woods, 2005; Zayfert et al., 2002). Posttraumatic stress symptoms are related to other physical changes such as increased heart rate, cortisol levels and sleep difficulties (Buka et al., 2001) as well as to chronic fatigue syndrome and fibromyalgia (Borsini et al., 2014), seizures (I. Lee et al., 2015), and obstructive respiratory diseases (Spitzer, Ewert, et al., 2021).
The causal relation between trauma symptoms, VE, and health outcomes in adolescent high-risk populations, such as incarcerated youth, is not well understood. One study of at-risk preschoolers assessed these relationships and found that rates for conditions such as asthma, allergies, flu/cold, and gastrointestinal problems were higher than expected for children who had symptoms of traumatic stress but not higher when there was VE without traumatic stress, suggesting that traumatic stress symptoms are a causal mechanism for physical health (Graham-Bermann & Seng, 2005).
A few studies have explored the interconnectedness of these relationships, finding that traumatic stress symptoms mediate VE and health outcomes. For example, multiple studies show that symptoms of traumatic stress predict negative health outcomes after intimate partner violence, leading to neuromuscular, stress, sleep, and gynecologic-related issues, among others (J. C. Campbell & Lewandowski, 1997; Dutton et al., 2006; Woods et al., 2008). Additionally, studies assessing different forms of VE, such as combat and community VE, have also found that traumatic stress symptoms act as a pathway to asthma, gastrointestinal issues, and somatic complaints (R. Campbell et al., 2008; Fairbrook, 2013; Graham-Bermann & Seng, 2005; Schnurr & Spiro, 1999). In a recent study of maltreated youth researchers found that posttraumatic stress reactions in this population mediated the relation between VE and physical health symptoms with a high degree of variance explained by trauma symptoms throughout development (Rueness et al., 2019b).
While these results demonstrate the significance of the relationship between VE, traumatic stress symptoms, and health outcomes in identifying health issues, more research is needed to determine the extent of the relationship.
Present Study
A goal of the present study is to use incarcerated youth medical records review to examine intake health conditions and their association with exposure to different types of pre-incarceration VE and current trauma symptoms. We hypothesize that childhood VE will be related to the presence of a high rate of health disorders. We further hypothesize that the presence of traumatic stress symptoms will interact with VE such that VE and trauma symptoms will increase the association between VE and the presence of physical health conditions in this high-risk population of adolescents.
Method
Sample
Participants were drawn from an all-male adolescent training facility in Southeastern Michigan. The sample consisted of willing youths, who provided consent, within the general facility population. There were 200 beds at the facility at the time of the study with a rotating population that was mostly full. One hundred and twenty-three (123) youth consented or assented to participation in the study. For various reasons, such as transfer to a new facility, eight youths never provided any data after consenting, leaving a final sample of 115 boys.
Procedure
The University of Michigan Institutional Review Board (IRB) approved this study. In addition to IRB approval, it was necessary to obtain permission from the State Department of Human Services to conduct the study in a state-run facility. Researchers also obtained a federal Certificate of Confidentiality due to the delicate nature of the data collected. Each youth was given a brief description of the study and asked if they were interested in learning more about the study. After expressing interest in the study, adolescents consented to participate if they were over 18 years old. Consent forms were written at the third-grade level.
For youth under 18 years old, the legal guardians of each youth were contacted via letter to obtain parental consent. If the youth was a state ward the court was asked for consent. Once signed guardian or court approval was returned via mail, youths under 18 years old read and signed an assent form. Assent forms were written at a third-grade level and youth were given access to teachers and researchers to explain the nature of the study and the benefits and risks of participation.
Adolescents were not compensated for participation. The training school received a small amount of money to benefit the boys at the facility, but this donation was not contingent on individual participation. Adolescents who did not consent to take part in the study were given another task to complete so that facility staff would not know who participated in the study.
Researchers gave directions to the participants that were written at the third-grade reading level. If the adolescent did not understand the instructions, the directions were read aloud to him by a researcher. Trained graduate and undergraduate research assistants collected health data from participants’ medical files that were coded at the facility. For additional confidentiality, only the participants’ assigned numbers appeared on their files during file review. The present study is part of a larger project on the relationships between cognitive disabilities, VE, and behavioral problems that are publicly available (Perkins et al., 2023).
Measures
Health Problems
Trained graduate and undergraduate research assistants coded health data from each participant’s medical chart. Information collected on current and past health status included: allergies, asthma, headaches, high blood pressure, attention deficit hyperactivity disorder (ADHD), gastrointestinal problems, and seizures (see Supplemental Appendix A). ADHD was included as a health condition rather than a mental health condition because it was used in the 2001 National Health Interview Survey (NHIS) on child health (Bloom et al., 2009). Information regarding any current and past prescribed medications was collected and coded for diagnostic purposes. Diagnoses derived from medications are shown in Supplemental Appendix B. A total health score was obtained by summing the number of health conditions from 1 to 7.
Interpersonal Violence
Violence history was examined with the Conflict Tactics Scale (CTS) (Straus, 1979). The CTS is extensively used to determine children’s exposure to domestic violence and healthy resolution of conflict (Straus & Gelles, 1995). The measure assesses conflict in relationships and how they are handled in dyads (parent-parent, child-parent, sibling, Straus, 1990).
For each relationship, there were 18 items on a 1 to 5 Likert-type scale where one equals “never” and five equals “every day.” The present study modified the CTS to examine variations in experience given the age of the participant. In our sample, youth ranged in age. In addition, physical and verbal altercations are known to be more common in early childhood (Tremblay et al., 2004). In this modified version, each participant rated how often the item happened to him from ages 6 to 12 and again from ages 13 to 18. There are four subscales for each of the types of relationships assessed; reasoning, verbal aggression, mild conflict tactics, and severe conflict tactics. To obtain a total score, reasoning items are reverse coded.
In this study, three relationships are examined: 1) conflict instigated by the participant’s sibling (sibling violence), 2) by the participant’s parents toward the child (child abuse), and 3) conflict between the participants’ parents (IPV). Reliability for the current study ranged from (alpha) .92 to .95.
Sexual Abuse
A modified version of the Childhood Trauma Questionnaire (CTQ, Bernstein, 1994) was used to assess sexual abuse (SA) history. The original scale has 5 items and was modified to add items to assess SA that might not be identified by the participant as abusive – “I had sex with an adult or with someone who was a lot older than me (someone at least 5 years older than me).” It is common in youth populations that sexual experiences with older teens and young adults are classified as “dating” rather than SA (Lassri et al., 2022). The rating scale consisted of 5 points, from 0 (never true) to 1 (rarely true), 2 (sometimes true) to 3 (often true) to 4 (very often true). Internal consistency for the childhood sexual abuse scale in the present study was (alpha) .85.
Community Violence
This measure used 15 community violence items adapted from The Things I Have Seen and Heard scale (Martinez & Richters, 1993; Richters & Martinez, 1993) to assess whether study participants were exposed to community violence during childhood. Scores represent the total of community violence items endorsed and range from zero to 15. Internal consistency in the present study was .89 (alpha).
Posttraumatic Stress Symptoms
Posttraumatic stress symptoms were assessed with the Trauma Symptom Checklist for Children (TSCC), a 44-item self-report measure (Briere, 1996; Briere & Elliott, 1994). The TSCC is appropriate for youth who have experienced a range of traumatic events such as various forms of child abuse, neglect, accidents, and natural disasters (Briere, 1996), and assesses the level of clinical response to trauma. The checklist includes five clinical scales including anxiety, depression, anger, posttraumatic stress, and dissociation. Items are rated on a 4-point scale ranging from zero to three, where zero equals “never” and three equals “almost all of the time.”
Analyses
To examine the relationship between VE, traumatic stress response, and physical health outcomes in incarcerated adolescents, a series of logistic regression analyses were performed with specific health problems as outcomes. The most common health outcomes, including allergies, asthma, ADHD, and seizures, served as the dependent variables in these analyses. Age at exposure was also examined as a predictor to understand the role of developmental timing.
To test the hypothesis that childhood VE is related to the presence of health disorders and that trauma symptoms may moderate the effect of VE on health we regressed previously correlated VE types on the outcome of the presence of specific health problems using trauma symptoms as a moderator.
Results
Demographics
The youth ranged in age from 13 to 20 years with a mean age of 17.28 years (SD = 1.30). Fifty-two percent of the adolescents identified as white, 41% African American, 3% Multiracial, 2% Hispanic or Latino, 1% Asian or Pacific Islander, and 1% as other. Thirty-seven percent were raised in two-parent homes, 30% in single-parent families, 15% where the mother or father was living with a partner, 15% with a relative other than the parents, and 3% in foster homes. The grade last completed in school ranged from 7 to 13 (including GED completion) with a mean of 10.44 (SD = 1.58). Sample characteristics are further detailed in previously published work (Perkins et al., 2011, 2012, 2014).
Physical Health
Participants ranged from having no health problems to experiencing all seven conditions drawn from their health records. Having two conditions was most common (33% of the sample) and having five conditions was least common (2.7% of participants). Allergies represented the most prevalent condition with 48.6% of the sample affected. ADHD was the second most common health problem with 53.3% of the adolescents, followed by asthma with 40.5% of participants affected. Twenty-three percent of participants had a history of seizures, with 14.4% having gastrointestinal problems. The least common problems were high blood pressure (4.6%) and headache (11.7%). In comparison to the National Health Interview Study (Bloom et al., 2009), sample youth had 3 to 7 times the rate of health problems (see Supplemental Appendix A).
Violence Exposure
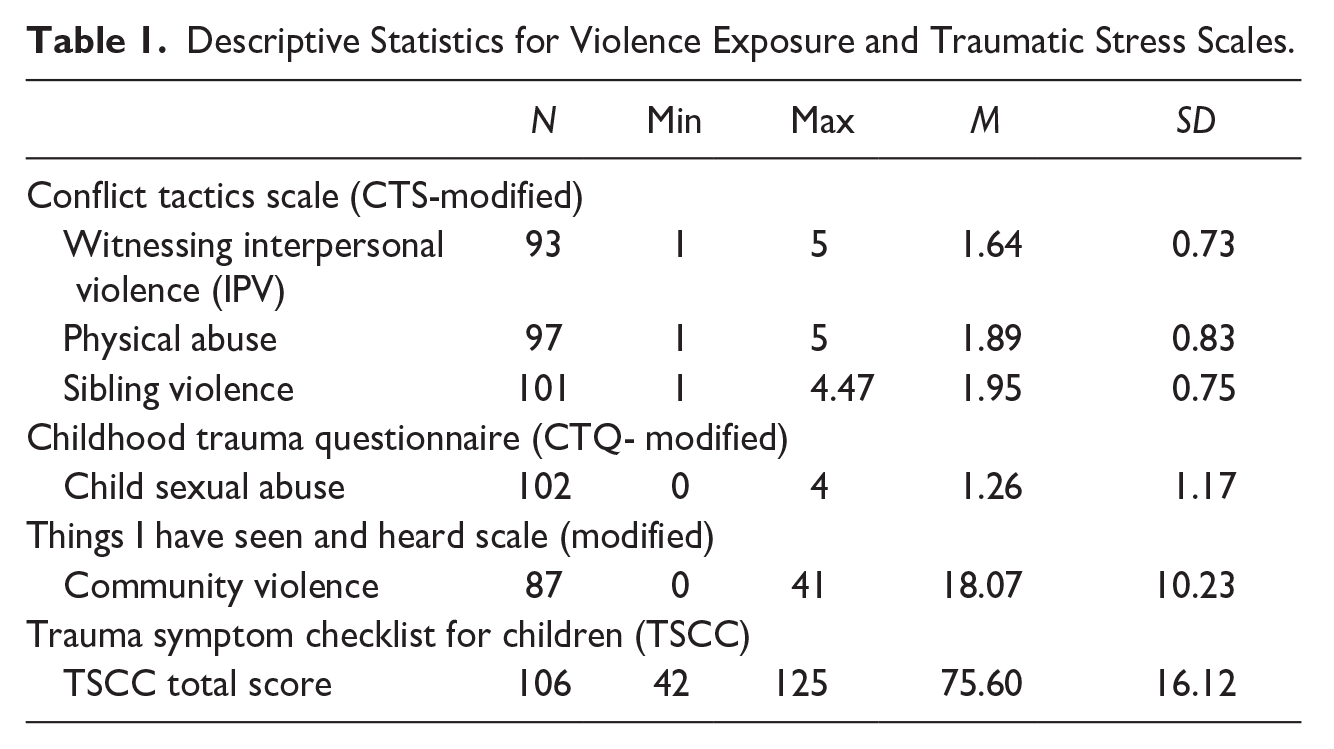
Total scores on the modified CTS in the present study ranged from 30 to 485 with a mean of 237.97 and a standard deviation of 80.56. The sibling violence score ranged from 1 to 5 with a mean of 1.95 and a standard deviation of 0.70 (see Table 1). A score of 1.95 is interpreted as approximately a mean score of 2, or “a couple of times a year.” The IPV and child maltreatment scores also averaged near a score of 2. The modified sexual abuse subscale from the CTQ used in the present paper ranged from 0 to 4 with a mean score of 1.26 or “rarely true” (see Table 1).
Descriptive Statistics for Violence Exposure and Traumatic Stress Scales.
Posttraumatic Stress Symptoms
The total score for the TSCC in the present study ranged from 42 to 125 with a mean score of 75.60 (see Table 1).
Correlations Between Variables
Pearson intercorrelations between total health problems, types of VE, and traumatic stress mean scale scores show that sexual abuse was correlated with the total health score at p < .05 (see Table 2). Witnessing IPV traumatic stress symptoms showed significant positive correlations with other forms of family violence.
Pearson Intercorrelations Among Total Health Problems, Types of Violence Exposure, and Traumatic Stress Mean Scale Scores.
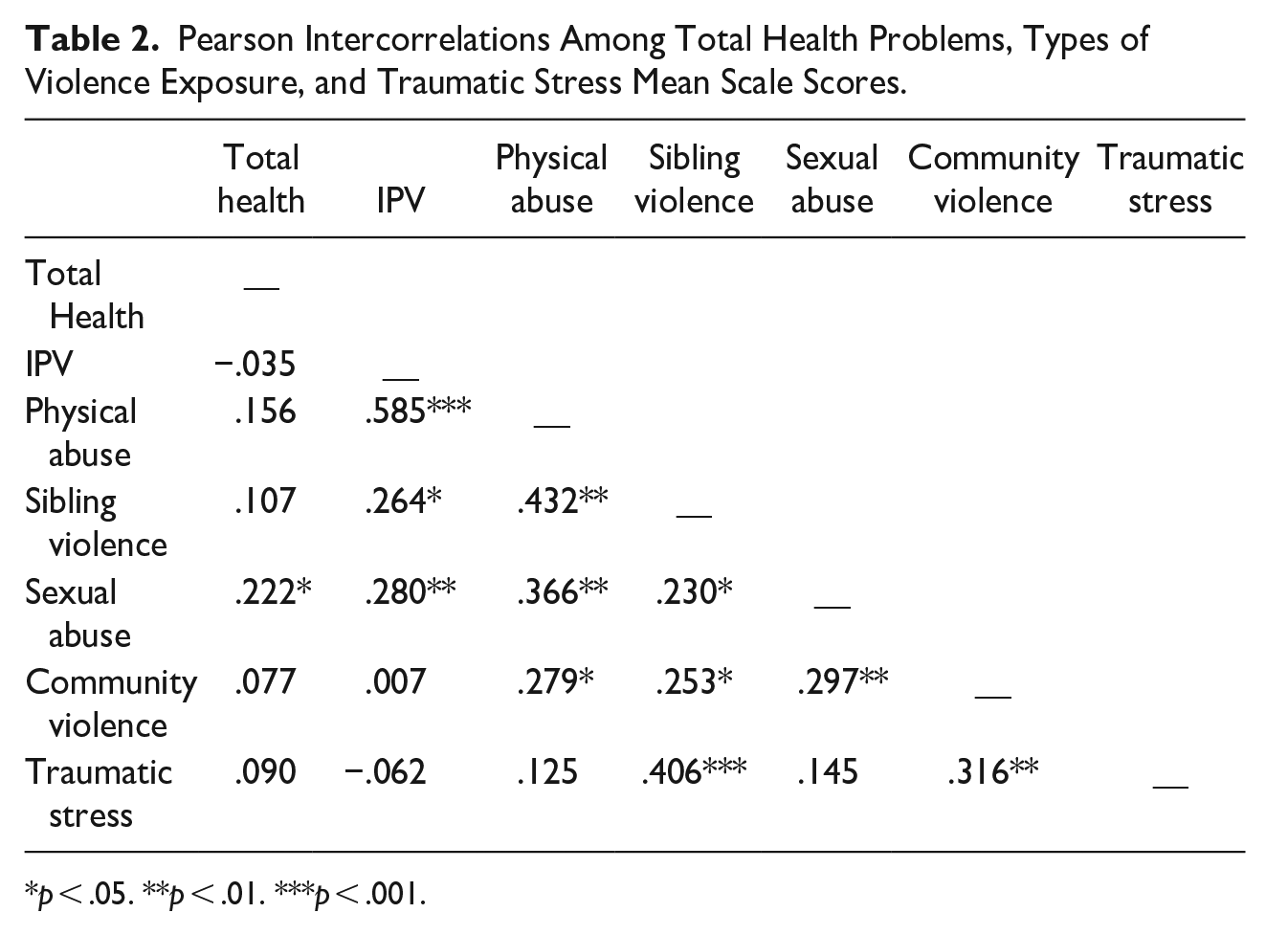
p < .05. **p < .01. ***p < .001.
Binary Logistic Regressions
Binary logistic regression showed no associations between age and health conditions (see Table 3). VE measures predicted two health outcomes (allergies and ADHD). Binary logistic regressions revealed that both physical and sexual abuse were significant positive predictors of ADHD rates. Asthma was predicted by community violence. The total score on the TSCC predicted fewer cases of asthma.
Results of Binary Logistic Regression Predicting the Presence of Asthma, Allergy, ADHD, and Seizures using Violence Exposure, Sexual Abuse, and Traumatic Stress.

p < .05. **p < .01.
Moderation Analysis
To examine if the correlation between childhood sexual abuse and total health score was moderated by individual traumatic stress symptoms, a linear regression was performed with the interaction between the CTQ SA score and TCSS total score as a moderator. Model 1 of the mediation analysis was significant for the effect of SA on total health problems, F(98) = 5.085, p = .026, see Table 4. In Model 2, SA remained a significant predictor of total health problems while the interaction between TSCC total score and CTQ SA moderated the effect at a trend level, F(97) = 4.203, p = .018, showing that TSCC partially moderated the relationship between SA exposure and total health. The change in R2 showed a trend toward significance, F(97) = 3.206, p = .076. Taken together, the mediation model accounted for approximately 8% of the variance in adolescents’ health problems, an increase from 4.9%.
Moderator Analyses: Sexual Abuse Predicting Total Health Problems With Trauma Symptoms as Moderator.
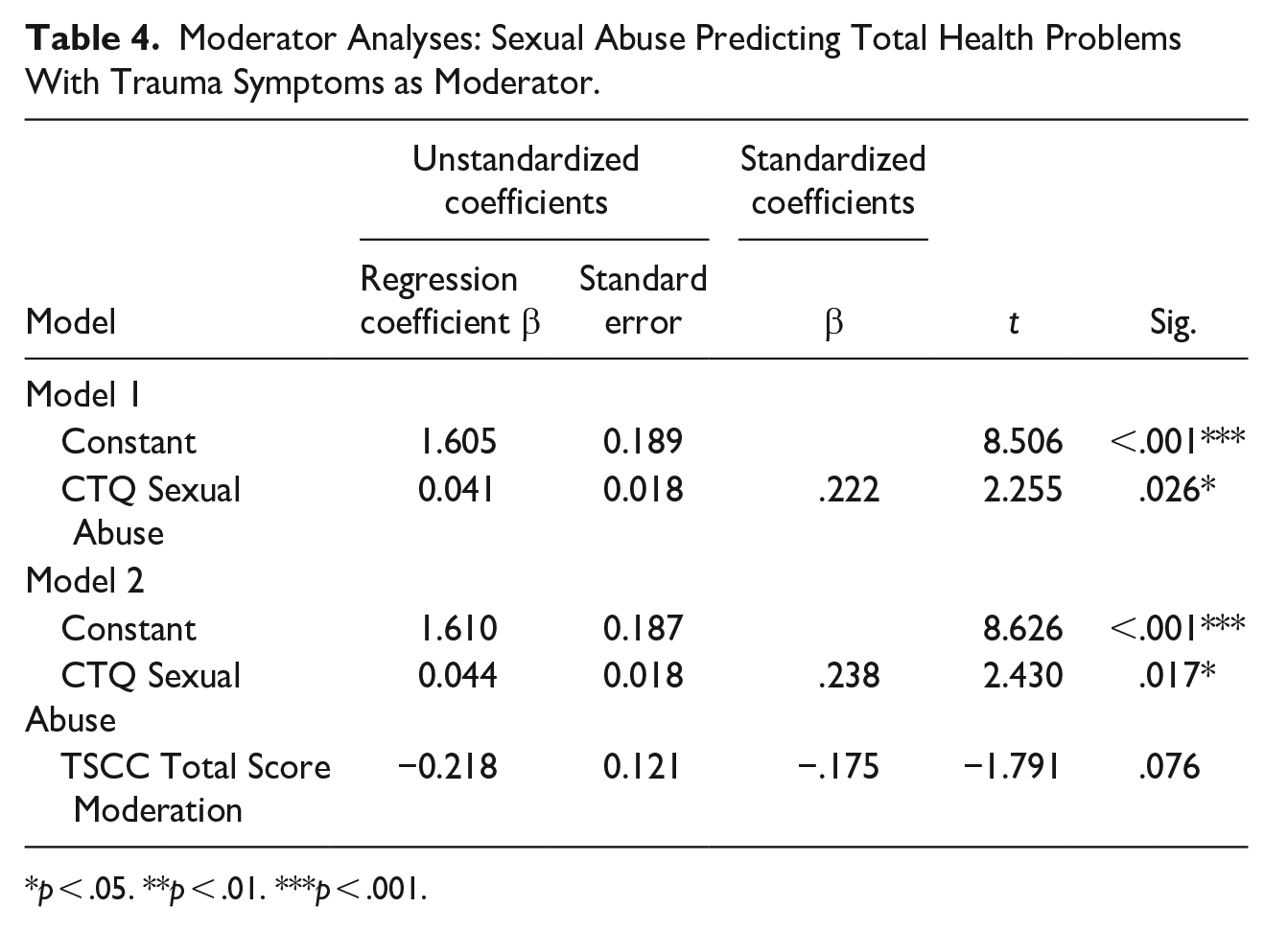
p < .05. **p < .01. ***p < .001.
Discussion
Since the early work on ACE, there has been a known connection between VE and adult health outcomes. It is less clear that VE in childhood is associated with the presence of poor health during childhood and the direction of effect is unclear. Understanding potential causal mechanisms in high-risk populations can lead to the development of interventions and screenings to reduce the risk of both VE and poor health outcomes. This is one of the few recent studies of incarcerated adolescents to examine medical records or attempt to quantify the extent of medical problems in incarcerated youth and to study the role of VE, traumatic stress symptoms, and health conditions within an at-risk incarcerated population.
In the present study, youth who are incarcerated showed high rates of health problems compared to NIHS rates during a similar period, as much as 7 times the rate. Our study demonstrates that prior SA and the presence of traumatic stress symptoms are important predictors of the rate of health problems among incarcerated male adolescents. While trauma symptoms were assessed at the time of the survey, health conditions were assessed at intake and SA was a retrospective self-report. This allows for a cautious interpretation of the direction of effect.
Violence Exposure, Traumatic Stress, and Specific Health Conditions
As previous research has demonstrated (Feinstein et al., 1998; Forrest et al., 2000; Hein et al., 1980; Shelton, 2000), incarcerated youth face numerous health issues, that exceed those found in the general population, with rates near 50% for some disorders. In this sample of incarcerated youth, allergies, asthma, ADHD, and seizures were the most prevalent conditions, in line with findings from previous work that found that respiratory and central nervous system disorders are common in this population (Hein et al., 1980; Shelton, 2000). High rates of ADHD and other cognitive disabilities have been found in our work and other prior studies (Perkins et al., 2014; Young et al., 2015).
Significant, positive correlations were found between several types of violence, which indicates that if the youth was exposed to one type of violence, he was often exposed to another kind. This supports many other studies that have documented the overlap in VE (McGuire & Jackson, 2018a, 2018b; Nikolaidis et al., 2022; Sheridan et al., 2017; Smith & Pollak, 2020, 2021). As reported in other studies, traumatic stress symptoms were significantly correlated with community and family violence (B. N. Bailey et al., 2005; J. C. Campbell & Lewandowski, 1997; R. Campbell et al., 2008; Dutton et al., 2006; Fairbrook, 2013; Haj-Yahia et al., 2019, 2021; Heinze et al., 2017; Moretti et al., 2006; Scarpa, 2003; Schnurr & Spiro, 1999; Seng et al., 2005; Theall et al., 2016; Woods et al., 2008).
This study also found that certain types of violence were uniquely related to specific health problems. The presence of asthma was associated with CV exposure, which is in line with previous research that shows that lung and breathing issues are common in high-risk populations and that this is not fully explained by poverty and poor living conditions (Beck et al., 2016; Butler et al., 2008; Landeo-Gutierrez et al., 2019; Spitzer, Ewert, et al., 2021; Wright et al., 2016). There are several reasons why this might occur. Airway constriction is often considered a stress reaction that could be connected to past violent events. In our study higher symptoms of traumatic stress separately predicted asthma, supporting this view. Past VE predicting the presence of asthma may be associated with other variables not measured in this study, such as individuals exposed to violence may be more likely to have poor living conditions. These environments might induce asthma symptoms if there is pollution or other toxins in the air.
Child physical abuse and exposure to IPV are associated with ADHD. It is important to note that other studies have found the presence of ADHD predicting childhood abuse (Gokten et al., 2016; Stern et al., 2018; Turner et al., 2010). It is well-known that children with disabilities, including both mental and physical health disorders, are at greater risk for VE (Perkins, 2012; Perkins & Graham-Bermann, 2012; Sullivan et al., 2010; Sullivan & Knutson, 2000), however, because our measures are both retrospective it is impossible to know the direction of effect. Further research will need to be done to determine the directionality of this relation. Understanding the direction of effect could assist in developing individual treatments for child abuse as a preventive intervention for ADHD or developing educational programming for parents at risk of abusing children with ADHD. Finally, it is not surprising that VE was not a stronger predictor of allergies. This condition is considered a reaction to aspects of the physical environment, such as genetics and exposure to toxins in utero (Holloway et al., 2010; Khan et al., 2015), which may or may not be more common in environments where violence is common.
Our findings support past literature, which suggests that being exposed to violence increases the risk of experiencing physical health problems (Aiyer et al., 2014; Bair-Merritt et al., 2012; Beck et al., 2016; Chen et al., 2023; Heissel et al., 2018; Hilker et al., 2005; Hussey et al., 2006; Jovanovic et al., 2017; Kapur et al., 2022; Landeo-Gutierrez et al., 2019; Midei & Matthews, 2011; Miller et al., 2018; Mueller & Tronick, 2019; Norman et al., 2012; Peckins et al., 2012; Rivara et al., 2019; Suglia et al., 2015; Wilson et al., 2005a; Wright et al., 2016).
Violence Exposure, Traumatic Stress, and Total Health Outcomes
In the moderation model, sexual abuse was a major contributor to total health problems, supporting the idea that sexual abuse is uniquely difficult for long-term health. The overall effect of an association between two measures of pre-incarceration status may suggest that the presence of health conditions makes children more vulnerable to becoming victims of SA.
However, trauma symptoms were assessed at the time of the survey, which is post-medical intake, and after our retrospective survey of VE. We found that current trauma symptoms moderated the association between SA and health at the trend level. These findings are in line with past research that reveals a mediating relationship between the three variables (R. Campbell et al., 2008; Graham-Bermann & Seng, 2005; Rueness et al., 2019b), with SA as a particularly high risk for negative health. However, this moderation was in the direction of lowering total health problems. Although both health and SA are retrospective reports, trauma symptoms were assessed as current. If we assume that trauma symptoms are the result of SA in the youth who experience SA, we can gain some insight into the direction of the effect. For those youth who developed trauma symptoms post-SA it may be that good health status before the SA is a risk factor for developing trauma following SA in this older sample or that youth with poor health and SA have less insight into their mental health functioning.
Limitations
One of the greatest strengths of this study is the medical records review of incarcerated youth, which enables some understanding of the causal direction of current functioning. However, our findings are limited by the quality of the records. Medical records were dependent on the thoroughness with which health history was collected and the extent of healthcare experiences. It is clear from prior work that incarcerated youth are less likely to have routine medical care but more likely to have medical care rising from injury or serious medical conditions (Barnert et al., 2016; Feinstein et al., 1998; Hein et al., 1980; Williams, 2006). Our data likely undercounted medical conditions due to incomplete records. We attempted to correct for poor record keeping by using both diagnoses in the record and intake medication to categorize an individual with a condition.
There are limitations to our data collection. Although the research assistants were trained to collect data from existing medical charts, considering the large amount of information contained in each chart and the inconsistency of the format some diagnoses may have been inadvertently overlooked during file review. It was impossible to know if there was a systematic gap in rates of diagnosis due to the wide variety of formats. Some youth had fairly extensive records, while others appeared to have almost no health history. Our data can not show if some health categories are systematically under or overreported.
Another limitation is the use of self-report data for VE and trauma symptoms. Although there was no indication of over or underreporting issues, youth may have been motivated to report more or less VE and trauma symptoms to please researchers or in a misguided belief that this could influence their sentence or treatment.
A final limitation of this study is the sample size. Although this is one of a limited number of studies to examine youth who are incarcerated and well within the average sample size with this population (Chow et al., 2022; Livanou et al., 2019; Pyle et al., 2016; Steele et al., 2016; Young et al., 2015), a larger sample size would have added power to detect variance (Funder et al., 2013; Sassenberg & Ditrich, 2019). While some of the correlations and beta values approached significance, a larger sample may have produced more significant findings.
Conclusion
The study contributes valuable information by showing higher rates of health conditions in incarcerated adolescents than in the general population and that VE is predictive of asthma, ADHD, and total health problems. Given these data, violence history, as well as traumatic stress symptoms, should be assessed during initial intake evaluations of detained youth along with a detailed assessment of identified health conditions. These data are important to researchers and policymakers. Exposure to ACE is well-known to be associated with long-term increased rates of morbidity and mortality. While youth are incarcerated, stabilizing health and providing trauma-informed care can decrease the long-term health risks in youth. Recent work has shown trauma-informed care to be positive for justice-involved youth (Baetz, 2021; Olaghere, 2021) however, more research into long-term health outcomes needs to be done. Youth-serving institutions should monitor trends in health, VE, and trauma so that longer-term trends can be identified.
Understanding how traumatic stress interacts with physical health symptoms will assist in the development of assessments for the early detection of traumatic stress that may shape later health and could serve as a warning sign that long-term health problems may be developing. There have been calls for the need for better trauma and health assessments (Committee on Adolescence et al., 2011) however, a joint assessment of trauma and physical health might help detect traumatic stress exposure that has been unrecognized and untreated. Early detection of the joint role of trauma and physical health will also help develop targeted interventions for this population, with the potential for preventive treatment targeted to youth incarcerated. Practitioners who treat incarcerated youth should be made aware of these predictors and the health disparities between them. Overall, the findings of the present study contribute to the body of research that takes a holistic approach to the study of health problems by considering multiple forms of deleterious experiences and their sequelae as they affect youth.
Given the risk that children with disabilities in the general population have to VE, future research should examine the role of cognitive disabilities, VE, and physical and mental health in this population.
Supplemental Material
sj-docx-1-yas-10.1177_0044118X241229733 – Supplemental material for Contributions of Violence Exposure and Traumatic Stress Symptoms to Physical Health Outcomes in Incarcerated Adolescents
Supplemental material, sj-docx-1-yas-10.1177_0044118X241229733 for Contributions of Violence Exposure and Traumatic Stress Symptoms to Physical Health Outcomes in Incarcerated Adolescents by Suzanne Perkins, Rebecca M. Ametrano, Marisa Leach, John P. Kobrossi, Joanne Smith-Darden and Sandra A. Graham-Bermann in Youth & Society
Footnotes
Data Availability Statement included at the end of the article
Data Availability Statement
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Eunice Kennedy Shriver National Institutes of Child Health and Development [3P50HD096719-05S1, 2022] for the writing of the report; the NIMH Training Grant for the Interdisciplinary Research Program on Violence and Mental Health [T32 MH020041] for study design and collection of data, the Office of Vice President for Research and Rackham School of Graduate Studies at the University of Michigan for study design, collection, analysis and interpretation of data.
Supplemental Material
Supplemental material for this article is available online.
Author Biographies
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.