
Abstract
Youth are disproportionately affected by substance use and associated sexual risk behaviors, increasing STI and HIV susceptibility. This study analyzed the interplay between alcohol/drug use before sex (ABS/DBS), perceived sex approval (e.g., perceived familial or peer approval in engaging in sex), and HIV/STI risk perception among youth aged 13–21 (n = 150). We assessed how these factors influenced condomless vaginal/anal sex (VAS) and oral sex practices. Results showed significant interactions between perceived sex approval and lifetime ABS for lifetime condomless VAS, and between HIV/STI risk perception and lifetime ABS for current condomless oral sex. These findings underline the influence of perceived sex approval and HIV/STI risk perception on youth’s sexual behaviors. Implications for targeted interventions are discussed.
Keywords
Introduction
Youth, particularly adolescents and young adults in the United States, face a disproportionate burden of sexually transmitted infections (STIs), including the human immunodeficiency virus (HIV). In 2020, individuals aged 13–24 years accounted for 20% (6,135) of all new HIV diagnoses (Centers for Disease Control and Prevention [CDC], n.d., a), ranking only second to individuals ages 25–34 (CDC, n.d., b). Youth disproportionately engage in ABS or DBS, which enhances the risk for condomless sex (CDC, 2019) and HIV infection. Prior research has suggested that understanding HIV and ways to prevent transmission among youth can increase condom use (Anderson et al., 1990; Qing et al., 2022; Shamu et al., 2020; Yu et al., 2022). Theories such as the Theory of Planned Behavior have explored how perceived approval of sexual activity may influence high-risk behaviors (Darabi et al., 2017). However, research in this domain has predominantly focused on vaginal sex, neglecting the potential risks associated with oral sex. While studies have shown that perceptions of sexual approval and risk can impact condomless sex (Lammers et al., 2013; Qing et al., 2022; Villarruel et al., 2004), the extent to which these factors influence the relationship between ABS or DBS and condomless sex, particularly oral versus vaginal or anal sex (VAS), remains understudied.
Perceived Sex Approval
Perceived sex approval, encompassing the youth’s perception of approval from key social network members such as parents, siblings, and peers, is recognized as influential in condomless sexual behaviors (Miller, 2002; Villarruel et al., 2004). Although youth familial and peer norms may differ, youths’ values often converge with both family (Boehnke et al., 2007) and peer norms (Solomon & Knafo, 2007), extending to the realm of sexual activity. For example, research suggests that youth’s perceived sex approval from parents, peers, and sexual partner are positively related to intentions to have sexual intercourse (Villarruel et al., 2004). However, scant research has examined the association between perceived sex approval and distinct types of condomless sex (oral vs. vaginal), as well as its moderation effects among youth. Perceived sex approval may play a role in mitigating risks associated with condomless oral sex or VAS, including STIs and human papillomavirus (HPV)-related head and neck cancers, which are increasing in prevalence (Strome et al., 2022).
HIV/STI Risk Perception
Beyond perceived sex approval, HIV/STI risk perception is another crucial factor in condomless sexual behaviors among youth. Historically, HIV/STI risk perception, defined as an individual’s perception of susceptibility and knowledge of prevention strategies regarding HIV/STI, has been associated with reduced sexual risk behaviors among youth (Barrientos et al., 2007; DiClemente et al., 1992; Ploem & Byers, 1997). Low levels of HIV/STI risk perception have been linked to risky sexual behaviors, including condomless sex (Lammers et al., 2013; Raiford et al., 2009). Additionally, perceptions of vulnerability to acquiring HIV/STI may predict condom use during sex (Abel & Brunton, 2005; Leval et al., 2011; MacPhail & Campbell, 2001). Hence, youth with heightened HIV/STI risk perception are less likely to engage in condomless sexual behaviors (Grossman et al., 2008; Shamu et al., 2020). Nevertheless, it is argued that HIV/STI risk perception alone may be insufficient in understanding HIV/STI-related behaviors, necessitating a broader psychosocial perspective that incorporates attitudes, norms, and behavioral skills (Wulfert & Wan, 1993). Yet, research on risk perception’s role in moderating the association between substance use before sex and different types of condomless sex (oral vs. vaginal) among youth is limited.
HIV/STI-Related Health Risk Behaviors
National data indicate that 18.8% of youth report current ABS or DBS, with an additional 46.2% reporting current condomless sex (CDC, n.d., c). Extensive research demonstrates that youth engaging in ABS or DBS are at heightened risk for current condomless sexual behaviors (Dallo & Martins, 2018; Kingree et al., 2000; Sanchez et al., 2013; Tucker et al., 2012). Hence, understanding the factors influencing condomless sexual behaviors among youth engaging in ABS or DBS is crucial for developing HIV/STI strategies for this vulnerable population.
Few studies have investigated potential differences in condomless oral sex versus condomless VAS. This is critical given that less than 10% of male and female youth report using condoms during their last oral sex encounter (Habel et al., 2018; Holway & Hernandez, 2018), whereas 65% of youth report using condoms during their last VAS encounter (Hadley et al., 2009). Consequently, youth may perceive oral sex as less risky. Although the risk of HIV attributable to condomless oral sex is low (Page-Shafer et al., 2002), many other STIs are spread through condomless oral sex, including chlamydia, gonorrhea, syphilis, and human papillomavirus (HPV) which can lead to oropharyngeal squamous cell carcinoma (OPSCC; Edwards & Carne, 1998; Taberna et al., 2017). Studies indicate that adolescents and young adults generally perceive oral sex as less risky and more socially acceptable compared to VAS (Halpern-Felsher et al., 2005). Moreover, the epidemiological evidence supports a higher STI risk associated with VAS compared to oral sex (Habel et al., 2018). Additionally, loss of virginity is primarily linked with vaginal and anal sex (Bersamin et al., 2007), potentially explaining youth’s inclination toward oral sex from a cultural norm perspective. Despite these distinctions, few studies have examined condomless VAS and oral sex separately. Furthermore, most studies and prevention efforts on targeting sexual risk behaviors among youth primarily focused on vaginal sex (Halpern-Felsher et al., 2005). Additionally, limited research has investigated the association between perceived sex approval, HIV/STI risk perception, and condomless sex among youth, including their moderating effects.
To address these gaps in the literature, this study aims to explore (a) the associations of perceived sex approval and HIV/STI risk perception with lifetime and current condomless oral, vaginal, and anal sex among a diverse sample of youth and (b) the influence of perceived sex approval and HIV/STI risk perception on the association between ABS or DBS and lifetime and current condomless oral, vaginal, and anal sex. We hypothesized that (a) higher perceived sex will correlate with increased likelihood of lifetime and current condomless oral, vaginal, and anal sex; (b) greater HIV/STI risk perception will be associated with reduced likelihood of lifetime and current oral, vaginal, and anal sex; and (c) higher perceived sex approval and/or HIV/STI risk perception will strengthen the association between ABS or DBS and lifetime and current condomless oral, vaginal, and anal sex.
Methods
Participants and Procedures
This study utilizes baseline assessments from two pilot randomized clinical trials (RCTs) conducted at a youth-centered clinic in resource-limited Southeast Michigan. The trials were conducted from October 2016 to July 2017 and from May 2018 to March 2020 (Cordova et al., 2020, 2024; García-Torres et al., 2021). The trials aimed to evaluate a digital health intervention’s efficacy in preventing HIV/STI among youth. All study procedures received approval from the University of Michigan Institutional Review Board (HUM00097290), with a certificate of confidentiality obtained from the National Institutes of Health.
The interventions were tailored to address the unique challenges of youth in Southeast Michigan, focusing on engaging those at elevated risk for HIV/STI. Recruitment utilized various methods, including distributing flyers, word-of-mouth recommendations, clinic waiting areas, and direct patient contact.
Eligibility criteria required participants to be aged 13–21, reside in Southeast Michigan, and have no history of psychiatric hospitalization. Additionally, participants in the second trial had to be sexually active in the past 6 months and have access to a smartphone or tablet. A total of 150 youth were enrolled across both trials.
Data collection employed a web-based application for online surveys. The trials were conducted independently, and participants could not participate in both. Parental consent was not required for participants aged 13–17, in accordance with Michigan regulations. Socioeconomic data were not collected due to unreliability (Hammond et al., 2021), but the clinic served in Ypsilanti, a community with a median household income below the US median (U.S. Census Bureau, 2023a, 2023b).
Following informed consent, participants completed baseline assessments. Further methodological details and study context, including specific objectives and outcomes, are available in previous publications (Cordova et al., 2020, 2024).
Measures
Given the resource limitations and small sample sizes of our pilot study, single-item measures were utilized for self-efficacy in both research and clinical practice, following recommendations (Cunny & Perri, 1991; Hoeppner et al., 2011). Alcohol and drug use behaviors and sexual risk behaviors were dichotomized for analysis, with 0 indicating no risk present and 1 indicating risk present.
Sociodemographic Variables
Age, gender (1 = male, 2 = female, 3 = other), ethnicity (1 = White, 2 = Black, 3 = other), and sexual or gender minority status (0 = heterosexual, 1 = sexual or gender minority) were assessed.
Trial
Data were categorized based on the trial they originated from: the first trial with 50 participants (1 = study with 50 participants) or the second trial with 100 participants (0 = study with 100 participants).
Lifetime ABS and DBS
Adapted items from the Monitoring the Future study (Johnston et al., 2018) were used to assess lifetime ABS and DBS: “Have you ever been under the influence of alcohol before having sex?” and “Have you ever been under the influence of drugs while having sex?”.
Current ABS and DBS
Similarly, adapted from the Monitoring the Future study (Johnston et al., 2018) assessed current ABS and DBS, covering the past 30 days in one trial and the past 90 days in the second trial: “During the past 30/90 days, have you been under the influence of alcohol before having sex?” and “During the past 30/90 days, have you been under the influence of drugs while having sex?”.
Lifetime Condomless Sex
Participants’ lifetime condomless sex was assessed using items extracted from the Sexual Behavior Instrument (Jemmott et al., 1998): “Have you ever had vaginal or anal sex without using a condom?” and “Have you ever had oral sex without using a condom?”.
Current Condomless Sex
Similarly, items from the Sexual Behavior Instrument (Jemmott et al., 1998) assessed current condomless sex, covering the past 30 days in one trial and the past 90 days in the second trial: “In the past 30/90 days, about how often have you had vaginal or anal sex without using a condom?” and “In the past 30/90 days, about how often have you had oral sex without using a condom?” Responses were recoded as 0 = never and 1 = at least once.
Perceived Sex Approval
Perceived sex approval was measured on a 5-point Liker scale, asking: “Would most people who are important to you approve or disapprove of you having sex in the next 30/90 days?”. Higher scores represented higher perceived sex approval.
HIV/STI Risk Perception
HIV/STI risk perception was assessed with a statement rated on a 5-point Likert scale: “If I have sex without a condom I am likely to get HIV/STIs.” Higher scores indicated stronger risk perception.
Statistical Analyses
Descriptive, chi-square, and moderation analyses were conducted using SPSS V.28.0.1.0. Regression analyses were completed through StataSE 17, specifically using Firth’s logistic regression via a user-written command. Statistical analysis proceeded in four steps. First, descriptive statistics, such as frequencies and proportions for categorical variables (including sociodemographic and ABS or DBS) were generated. Means and standard deviations for continuous variables (age, perceived sex approval, and risk perception) were also reported. Second, chi-square analyses and independent sample t-tests were conducted: lifetime condomless VAS and lifetime condomless oral sex were compared across all independent variables. Current condomless VAS and current condomless oral sex were also compared. In an additional analysis 2.5, comparisons were made across the two trials’ samples, where the outcomes, predictors, and moderators included in the study were compared using independent sample t-tests. Third, a hierarchical logistic regression (HLR) was used via Stata to estimate the adjusted odds ratio (aOR) to quantify the association of each explanatory variable with the dependent variable (Block 1: sociodemographic variables and trial, Block 2: lifetime and current ABS or DBS, and Block 3: perceived sex approval and risk perception). The statistical significance level was <0.05 and adjusted odds ratios (aOR) and 95% confidence intervals (CI) were reported. Finally, moderation tests were conducted using PROCESS v4.1 for SPSS (Hayes, 2022) with 10,000 bootstrap replications to examine if perceived sex approval and risk perception moderated the association between condomless sex and ABS or DBS. Moderation tests examined the interaction between perceived sex approval or risk perception and ABS in relation to condomless oral sex and VAS. All moderation analyses were conducted controlling for age. Unstandardized regression coefficients and CIs were reported.
Results
The sample consisted of 106 females (71.1%), 21 males (14.1%), and 22 (14.8%) identified as other, which included 12 trans males (8.1%), 3 trans females (2%), and 7 nonbinary (4.7%). The mean age was 19.12 years (range = 13–21, SD = 1.82). Most participants identified as non-Hispanic White (n = 67, 45%), followed by Black or African American (n = 59, 39.6%), and other (n = 23, 15.4%). The other ethnicity category consisted of multiple race/ethnicity (n = 15, 10.1%), Hispanic or Latino (n = 5, 3.4%), American Indian/Native American (n = 1, 0.7%), Asian (n = 1, 0.7%), and other (n = 1, 0.7%). More than half of the participants identified as heterosexual (n = 86, 57.3%), while 64 (42.7%) participants identified as sexual or gender minority.
In terms of substance use and sexual risk behavior prevalence, descriptive statistics indicated that 53.3% (n = 80) of youth reported lifetime ABS, 43% (n = 64) reported lifetime DBS, 88.3% (n = 128) reported lifetime condomless oral sex, and 74.7% (n = 109) reported lifetime condomless vaginal or anal sex. Further, 25.5% (n = 37) of youth reported current ABS, 30.3% (n = 44) reported current DBS, 68.1% (n = 96) reported current condomless oral sex, and 59.7% (n = 86) reported current condomless vaginal or anal sex.
Chi-square analysis for lifetime sex indicates a significant relationship between lifetime ABS and lifetime condomless oral sex (χ21 = 14.17, p < .001) as well as lifetime condomless VAS (χ21 = 6.16, p = .01). There was also a significant relationship between lifetime DBS and lifetime condomless oral sex (χ21 = 10.51, p = .001) as well as lifetime condomless VAS (χ21 = 8.28, p = .004).
Additionally, chi-square analysis for current sex indicates a significant relationship between lifetime ABS and current condomless VAS (χ21 = 9.81, p = .002). There was also a significant relationship between lifetime DBS and current condomless oral sex (χ21 = 4.30, p = .04) as well as current condomless VAS (χ21 = 10.90, p < .001).
Lastly, independent sample t-test analysis showed that participants who reported lifetime condomless oral sex had significantly higher perceived sex approval (mean 3.40, SD 0.88) relative to those who did not report lifetime condomless oral sex (mean 2.41, SD 0.94; t141 = −4.34, p < .001). Furthermore, participants who reported current condomless VAS had significantly lower HIV/STI risk perception (mean 3.56, SD 1.29) relative to those who did not report current condomless VAS (mean 3.91, SD 1.09; t132.75 = 1.77, p = 0.04).
Correlates of Lifetime Sexual Risk Behaviors
Lifetime Condomless Oral Sex
Results of the HLR for lifetime condomless oral sex are indicated in Table 1. The first block included the sociodemographic variables and trial indication. The second block included the sexual risk behaviors variable (i.e., lifetime and current ABS; lifetime and current DBS). The third block included perceived sex approval and HIV/STI risk perception. Of the 11 explanatory variables, none were statistically significant in the final HLR model for lifetime condomless oral sex.
Hierarchical Logistic Regression Model Explaining Lifetime Condomless Oral Sex.
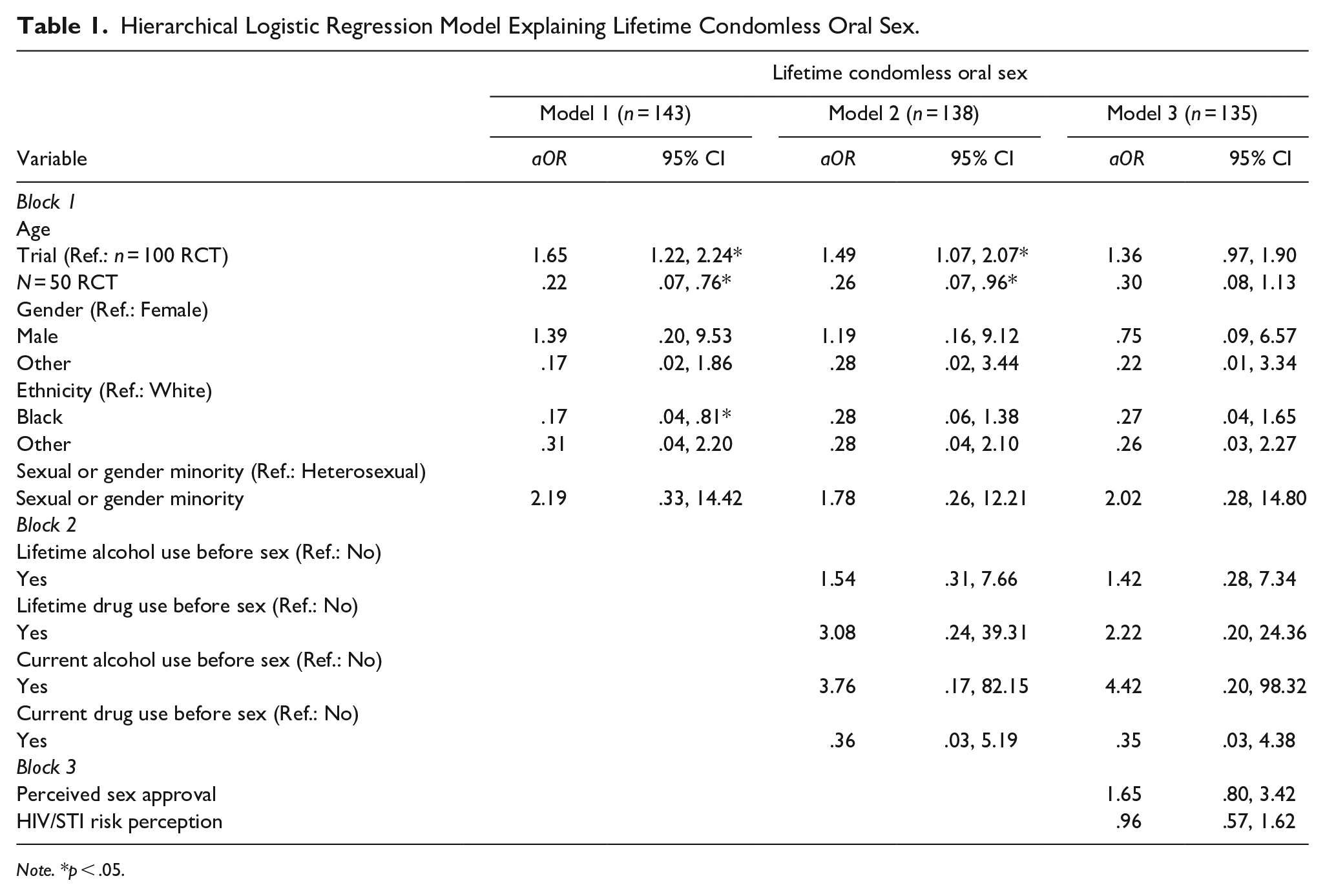
Note. *p < .05.
Lifetime Condomless Vaginal or Anal Sex (VAS)
Results of the HLR for lifetime condomless VAS are indicated in Table 2. The first block included the sociodemographic variables and trial indication. The second block included the sexual risk behaviors variable. The third block included perceived sex approval and HIV/STI risk perception. Of the 11 explanatory variables, two were statistically significant in the final HLR model for lifetime condomless VAS: age and other gender. A 1-year increase in age was associated having 1.63 times the odds of engaging in lifetime condomless VAS (aOR = 1.63, 95% CI: 1.21–2.20). Additionally, the odds of lifetime condomless VAS were lower for youth who identified as other (trans male, trans female, or nonbinary) compared to females (aOR = .04, 95% CI: .01–.21).
Hierarchical Logistic Regression Model Explaining Lifetime Condomless Vaginal or Anal Sex.
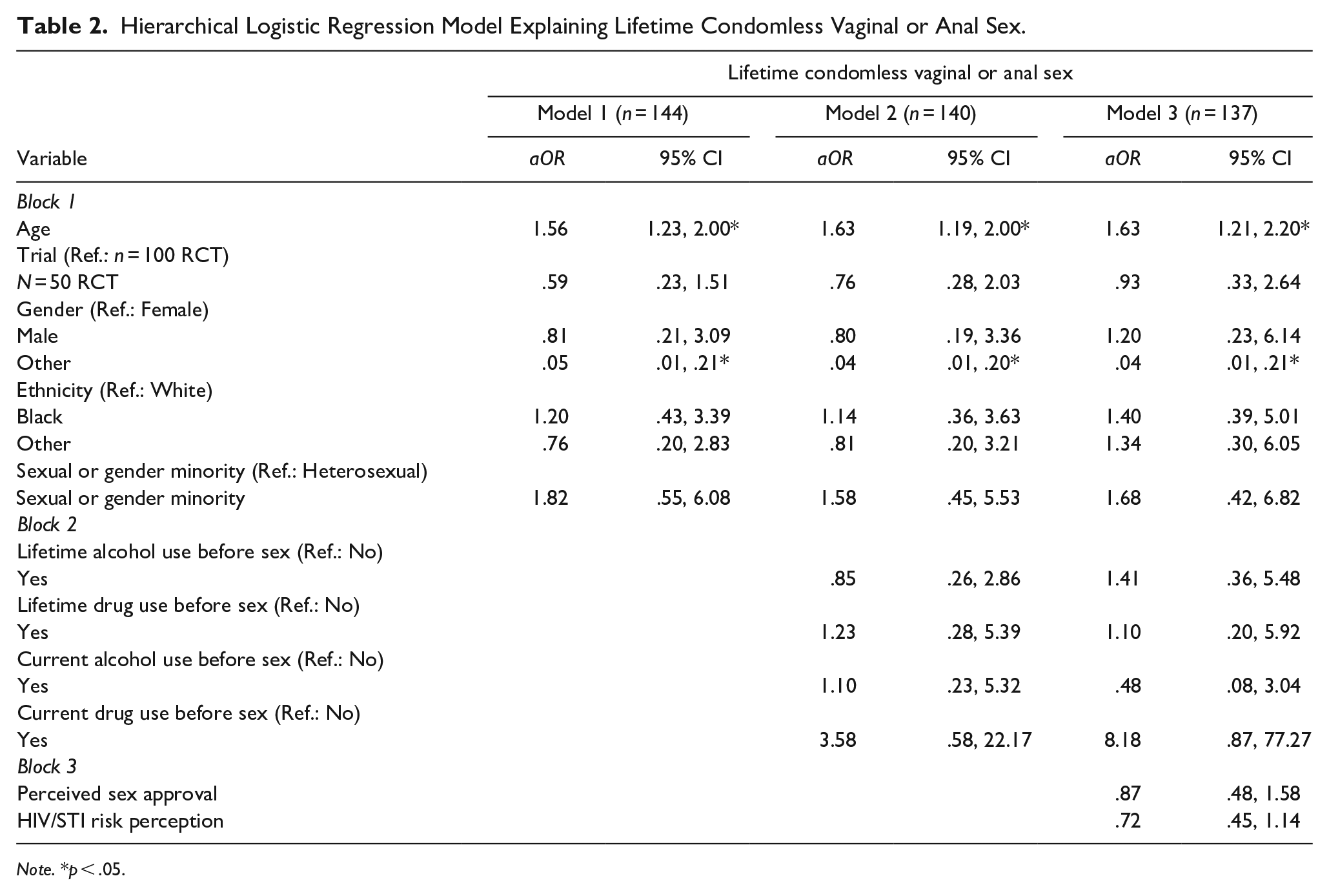
Note. *p < .05.
Correlates of Current Sexual Risk Behaviors
Current Condomless Oral Sex
Results of the HLR for current condomless oral sex are indicated in Table 3. The first block included the sociodemographic variables and trial indication. The second block included the sexual risk behaviors. The third block included perceived sex approval and HIV/STI risk perception. Of the 11 explanatory variables, one was statistically significant in the final HLR model for current condomless oral sex: trial. This suggests that there is a statistically significant difference between the two trials after accounting for the variables included in the model (aOR = .39, 95% CI: .17–.88).
Hierarchical Logistic Regression Model Explaining Current Condomless Oral Dex.
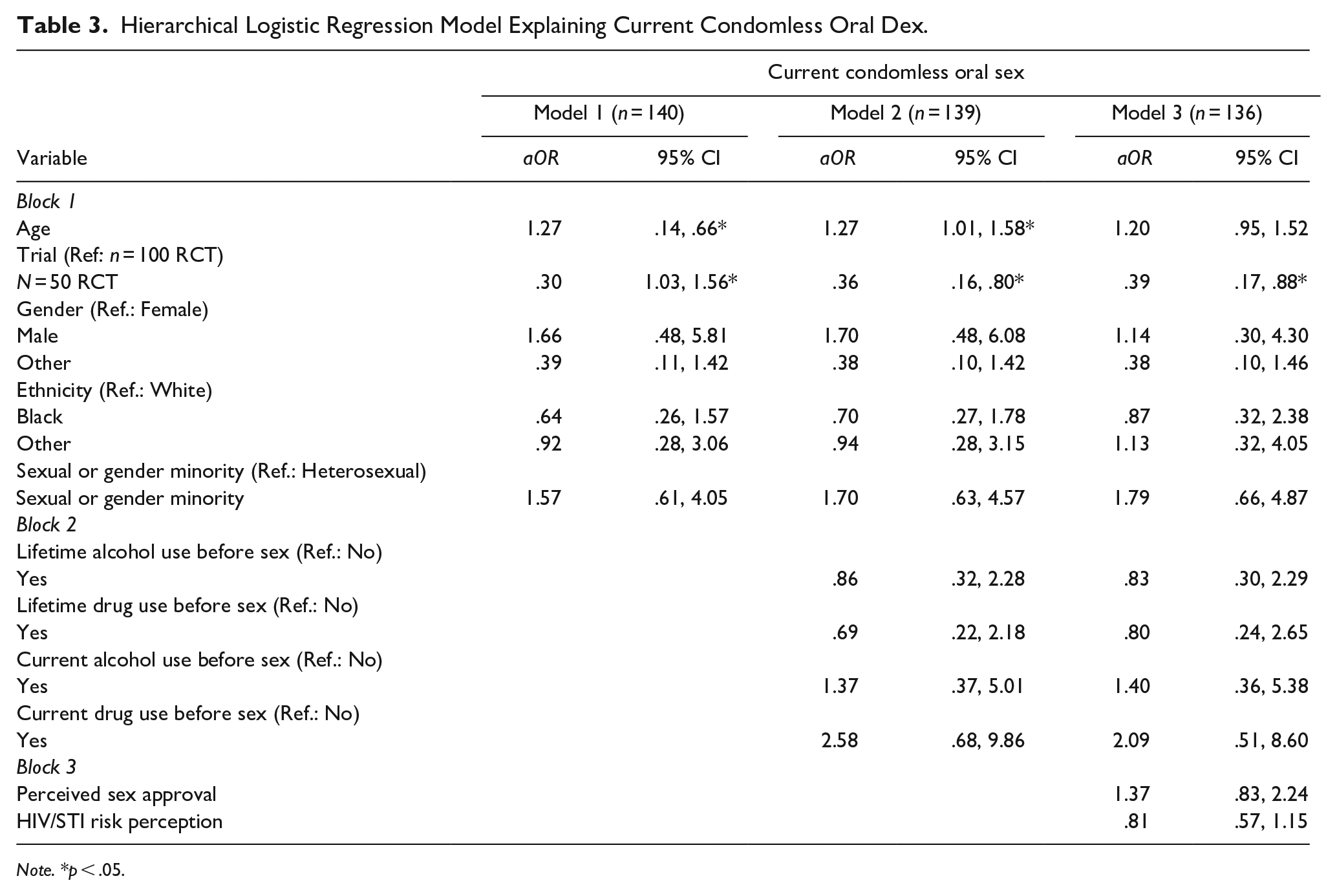
Note. *p < .05.
Current Condomless Vaginal or Anal Sex (VAS)
Results of the HLR for current condomless VAS is indicated in Table 4. The first block included the sociodemographic variables and trial indication. The second block included the sexual risk behaviors variable. The third block included perceived sex approval and HIV/STI risk perception. Of the 11 explanatory variables, two were statistically significant in the final HLR model for current condomless VAS: age and other gender. A one-year increase in age was associated with having 1.60 times the odds of reporting current condomless VAS (aOR = 1.60, 95% CI: 1.21–2.11). Additionally, the odds of current condomless VAS were lower for youth who identified as other (trans male, trans female, or nonbinary) compared to females (aOR = .09, 95% CI: .02–.37).
Hierarchical Logistic Regression Model Explaining Current Condomless Vaginal or Anal Sex.
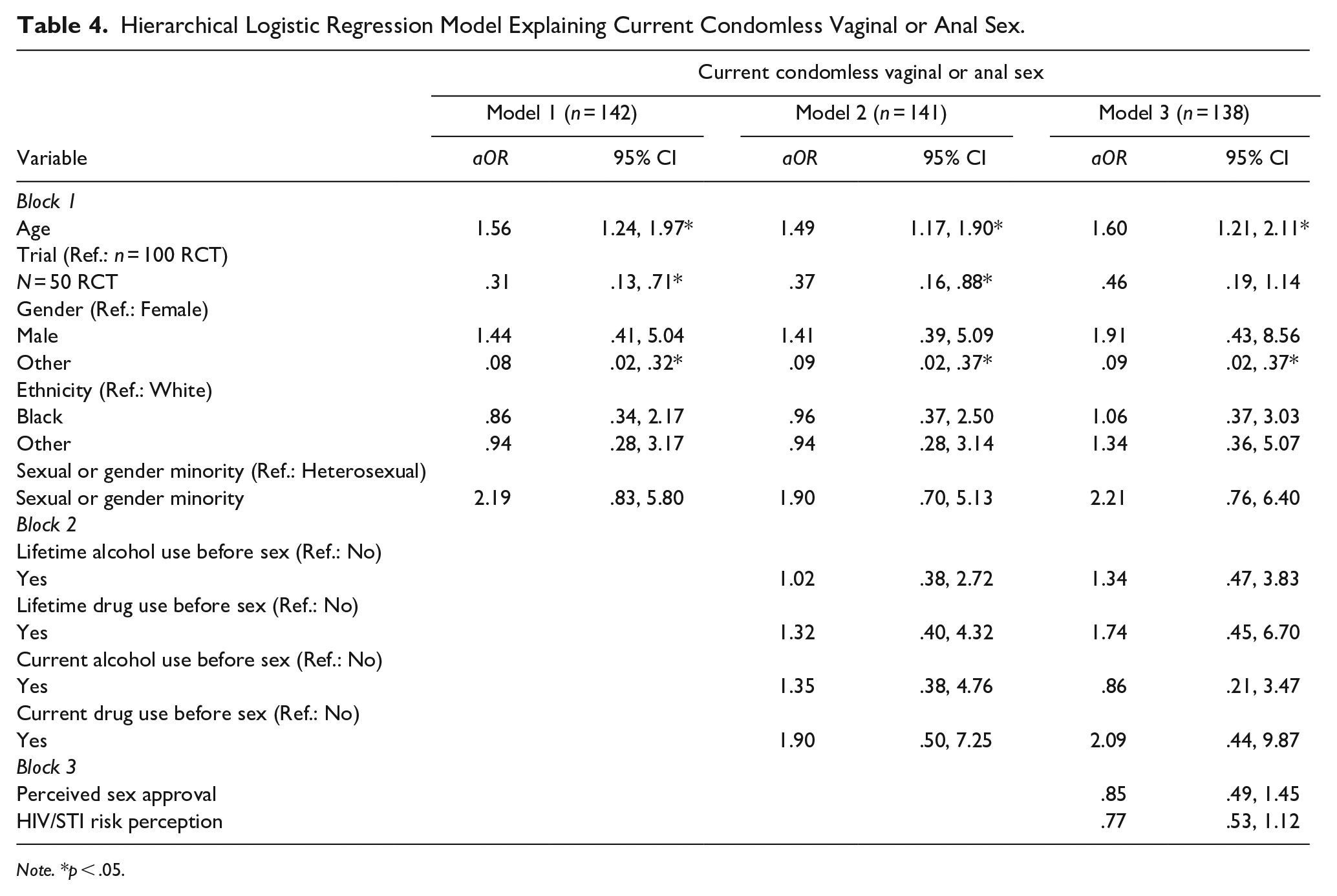
Note. *p < .05.
Moderation analyses
The interaction between perceived sex approval and lifetime ABS was significant (b = −1.04, 95% CI: –2.03–[–.06], p = .04), indicating that perceived sex approval moderated the association between lifetime ABS and lifetime condomless VAS. Results indicated that at low perceived sex approval (1 SD below the mean = 2.32), the relationship between lifetime ABS and lifetime condomless VAS was positive and significant (b = 1.90, 95% CI: 0.40–3.40, p = .01), but not significant at the mean (mean = 3.25; b = 0.92, 95% CI: −.04–1.88, p = .06) or at high perceived sex approval (1 SD above the mean = 4.18; b = −.05, 95% CI: −1.19–1.08, p = .93). Perceived sex approval only strengthened the association between lifetime ABS and lifetime condomless VAS when participants reported low perceived sex approval.
Additionally, the interaction between HIV/STI risk perception and ABS was significant (b = 0.71, 95% CI: 0.02–1.39, p = .04) for current condomless oral sex, indicating that HIV/STI risk perception moderated the association between lifetime ABS and current condomless oral sex. Results indicated that at high HIV/STI risk perception (1 SD above the mean = 4.93), the relationship between lifetime ABS and current condomless oral sex was positive and significant (b = 1.23, 95% CI: 0.15–2.32, p = .04), but not significant at low HIV/STI risk perception (1 SD below the mean = 2.50; b = −.48, 95% CI: −1.70–.73, p = .44) or at mean HIV/STI risk perception (mean = 3.71; b = 0.37, 95% CI: −.42–1.17, p = .36). HIV/STI risk perception only strengthened the association between lifetime ABS and current condomless oral sex when participants reported high HIV/STI risk perception.
Discussion
This study extends the literature on sexual risk behaviors by investigating the association between condomless oral sex and condomless VAS in relation to substance use before sex, perceived sex approval, and HIV/STI risk perception. Our first hypothesis of the positive association between perceived sex approval and both lifetime and current condomless oral sex and condomless VAS was not supported in this study sample. Although we did not have significant findings, previous research has suggested that engagement in oral sex is associated with perceived peer approval (Bersamin et al., 2006; Cherie & Berhane, 2012; Potard et al., 2008) and perceived parental values (Dittus & Jaccard, 2000; Hutchinson et al., 2003; Jaccard et al., 1996; Somers & Anagurthi, 2014). Youth who believe that their parents or peers approve of them engaging in sex may be more inclined to engage in oral sex, as they might believe it is relatively safe in comparison to VAS. In terms of vaginal sex, a study among Spanish-dominant youth found that normative beliefs regarding their parent’s and peers’ approval of sexual intercourse were positively related to intentions to have vaginal sex (Villarruel et al., 2004). These findings indicate that youth may engage in condomless sex more frequently, especially when it aligns with their perceived sex approval. Our findings may differ due to our smaller sample size and wider age range. It’s plausible that perceived sex approval affects participants differently based on age and developmental stages.
Similarly, our hypothesis regarding the association between higher levels of HIV/STI risk perception and a lower likelihood of condomless oral sex and condomless VAS was not supported. This contrasts with previous findings suggesting that youth with high levels of HIV/STI risk perception may be less likely to engage in condomless sexual behaviors (Lammers et al., 2013; Shamu et al., 2020). Our differing results could be attributed to variations in sample characteristics and cultural contexts, as these data collection took place in more homogeneous communities (i.e., Black young adults in South Africa) and among older populations (Lammers et al., 2013; Shamu et al., 2020). It may be that HIV/STI risk perception works differently in diverse youth, and from a developmental perspective, is not as effective among younger adults. Another explanation may be that youth do not believe they are at risk for acquiring HIV/STIs in the first place, regardless of whether they use a condom or not. Previous studies have shown that condom use is associated with youths’ perceptions of whether they feel vulnerable to acquiring HIV or STIs (Abel & Brunton, 2005; Leval et al., 2011; MacPhail & Campbell, 2001). Youth also may value the use of condoms for reasons outside of STI prevention, primarily using condoms to prevent both pregnancy and STIs in combination (Abel & Brunton, 2005). Our study sample of youth may have varied risk perceptions whether this is a result of their knowledge of condoms in preventing HIV/STIs or their perceived susceptibility to acquisition.
Regarding our third hypothesis, we found partial support as perceived sex approval moderated the association between lifetime ABS and lifetime condomless VAS, while HIV/STI risk perception moderated the association between lifetime ABS and current condomless oral sex. Specifically, the association between lifetime ABS and lifetime condomless VAS was stronger for participants who reported lower levels of perceived sex approval. Although the directionality of the association is counterintuitive, it is possible that youth with low levels of perceived sex approval may be less likely to engage in risky behaviors, as this implies that their family and peers may be less supportive of them engaging in condomless VAS or using ABS. For example, youth with perceptions of maternal disapproval of sex are less likely to initiate sexual activity (Dittus & Jaccard, 2000), however, research has seldom explored the relationship between perceived familial approval of sex and condomless sex. In addition, youth with low perceived sex approval may be less likely to engage in ABS, decreasing the chances of condomless sex as alcohol can impair judgment and decision-making (Cho & Yang, 2023). In fact, in a post hoc analysis, we found that higher perceived sex approval was associated with higher odds of lifetime ABS (p < .001, aOR = 2.18, 95% CI: 1.44–3.29), which is also to say the reverse: lower perceived sex approval is associated with lower odds of lifetime ABS. Perceived sex approval may influence youth’s decision to take part in other risky sexual activities, such as ABS. This finding aligns with previous studies that have found that peer influence may play a significant role in youth sexual risk behaviors through descriptive norms (peers’ sexual behaviors), injunctive norms (peer approval), and social capital (Cordova et al., 2022; van de Bongardt et al., 2015). Peer norms have been found to be significantly associated with willingness to drink (Jackson et al., 2014), however, the moderation effects of perceived sex approval and ABS with respect to condomless VAS are lacking in research. As we did not examine the direction of this moderation analysis, this finding should be interpreted with caution.
Lastly, HIV/STI risk perception only moderated the association between lifetime ABS and current condomless oral sex. Specifically, the association between lifetime ABS and current condomless oral sex was stronger for participants who had high HIV/STI risk perception. This finding suggests that HIV/STI risk perception as well as ABS may play a role in condomless oral sex. It appears that youth who are aware that condoms are an effective preventive biomedical tool for HIV infection and who have not used ABS may be less likely to engage in condomless oral sex. However, this finding should be interpreted with caution as we did not examine the direction of this association. Future research should explore the direction of this interaction.
Advancing scientific knowledge regarding how VAS and oral sex outcomes differ based on meaningful moderators is important. In this study, we found that HIV/STI risk perception strengthened the association between lifetime ABS and current condomless oral sex (but not condomless VAS), whereas perceived sex approval strengthened the association between lifetime ABS and lifetime condomless VAS (but not condomless oral sex). Importantly, these relationships that were moderated by HIV/STI risk perception and perceived sex approval may provide important avenues for intervening and preventing differing condomless sex (oral vs. VAS). It may be that high HIV/STI risk perception only serves as a potential moderator in the case of oral sex because these youth are more aware of the risks that are associated with condomless oral sex, which include increased risk for STIs and head and neck cancers (Strome et al., 2022). Educating youth about preventative measures, regardless of the type of condomless sex, is important. Perceived sex approval only served as a moderator for condomless VAS. Perhaps youth with low perceived sex approval believe that condomless VAS is more risky than condomless oral sex, and therefore their perceptions only take effect as moderators with condomless VAS. Familiarizing youth with the risks of both condomless oral sex and condomless VAS is crucial to prevent future STIs and other health complications. Additionally, only ABS, but not DBS, was implicated in these interactions. While a substantial amount of literature has shown the link between ABS and condomless sex, the findings regarding DBS have been mixed, especially with cannabis (Dir et al., 2018). In this study, we did not differentiate between specific illicit drugs. Therefore, we speculate that cannabis is the driving substance behind drug use that is being measured in this study.
The present study has intervention implications. Previous research has shown that school-based interventions focused on HIV/STI risk perception have promoted higher levels of condom use (Kinsler et al., 2004) and reductions in sexual exposure (Adeomi et al., 2014). However, interventions looking at direct behavioral changes in this context are limited. Previous research has explored theoretical predictors like the Theory of Planned Behavior and the socio-ecological framework concerning perceived sex approval. Studies show that subjective norms, such as peer and family approval, significantly predict condom use among college students (Asare, 2015). Educational interventions based on the Theory of Planned Behavior effectively reduce high-risk sexual behaviors (Darabi et al., 2017), suggesting potential benefits for interventions in schools, like modifying perceived sex approval among peers, to prevent such behaviors. Moreover, the socio-ecological framework reveals various factors influencing youth’s engagement in sexual risk behaviors, including family, peers, and social norms (Khuzwayo & Taylor, 2018). Programs enhancing parent-child communication and peer relationships regarding sexual behaviors could mitigate condomless sex. These insights and theoretical frameworks offer explanations for current findings and lay the groundwork for future research.
Study findings should be interpreted in light of several limitations. First, this study used a cross-sectional design. As a result, the temporal nature of the relationships cannot be inferred. Future studies should include longitudinal designs to understand the moderating effects of perceived sex approval and HIV/STI risk perception on condomless sexual behaviors. Moreover, the age range in this sample was broad, from 13 to 21, and may not have accounted for developmental differences. Nevertheless, when these data were collected, adolescence comprised the 13–21 age span. Furthermore, we identified discrepancies in the HLR between the two study trials. Although we accounted for the differences between study trials in our analyses, future research involving larger sample sizes would not only provide a more robust validation of our findings but also offer the opportunity to explore additional predictors that were not examined in the present study. The study also used self-reported measures, which increases the potential for participants to misreport sexual behaviors. However, adolescents have been found to report high levels of honesty in responding to sexual behavior questionnaires (Jones & DePalma, 1999; Siegel et al., 1998). Lastly, this study involved a sample that is not nationally based. Although the sample is community-based and included diverse youth, study findings may not be generalized to all youth in the United States as participant responses were taken from only one community-based clinic. This study should be replicated with other large and diverse samples to determine whether these findings hold true across other regions of the world.
In conclusion, this study advances understanding of condomless sex, perceived sex approval, HIV/STI risk perception, and substance use among youth. Interventions targeting familial and peer approval and enhancing HIV/STI risk perception may mitigate the risk of condomless sex, thus reducing HIV and STI transmission. Prospective studies are needed to elucidate the temporal relationships between psychosocial factors and condomless sex.
Footnotes
Data Availability Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was supported by a grant from the National Institute on Drug Abuse (R03DA04189101A1) and pilot funding from the University of Michigan Rogel Cancer Center to David Cordova. Preparation of this manuscript was supported in part by the Stamps Scholars Program to Sarah Khreizat.