
Abstract
Introduction
With growing attention to the role of social factors in shaping health, efforts have emerged to integrate social risk information into population health surveillance and healthcare delivery. However, current approaches to address social risk tend to focus on responding to each risk factor in isolation, overlooking the interconnected nature of multiple social risks that often cluster together.
Methods
This study used latent class analysis to identify profiles of co-occurring social risk using a national sample of 110,028 adults across 17 U.S. states.
Results
Three profiles emerged: Low Social Risk, Moderate Financial Strain with Food Insecurity, and High Financial Strain with Food and Housing Insecurity. These profiles were characterized by their health conditions and examined in relation to self-reported health (SRH). The High Financial Strain with Food and Housing Insecurity profile was characterized by elevated rates of depression, obesity, hypertension, and the highest odds of reporting poor/fair SRH (OR = 3.1, 95% CI: 2.78–3.67). The Moderate Financial Strain with Food Insecurity profile also showed increased odds of poor SRH (OR = 2.03, 95% CI: 1.85–2.23).
Conclusion
The findings underscore the importance of understanding clustering of social risks to provide more targeted, effective population health strategies.
Introduction
Social determinants of health (SDoH) are the conditions in which people are born, grow, work, live, and age, that comprise non-medical factors that account for 80% of variance in health outcomes. 1 These conditions include education, job opportunities, income, access to nutritious foods, safe and affordable housing, and neighborhood environments. 2 Greater attention towards social needs in recent years has prompted the development of screening instruments such as PRAPARE, 3 and the Accountable Health Communities social needs tool. 4 These assessments have been utilized in healthcare systems’ efforts to collect information on social risk factors such as housing or food insecurity, access to transportation etc. to leverage this data with clinical information to develop better strategies to address social risk. Consequently, an expanding body of research has emerged, identifying social risk factors and investigating their associations with specific health conditions and quality of life. Despite growing knowledge and identification of social risk factors, less is known about how multiple risks cluster and interact to influence health outcomes. The fundamental cause theory provides a framework for understanding socioeconomic status as a fundamental cause of health inequalities. Socioeconomic status affects disease and health outcomes through multiple social risks that tend to cluster or co-occur.5-7 Unequal access to resources influences both the exposure to risk and the capacity to mitigate its effects. Individuals with lower socioeconomic status are more likely to experience multiple social risks and less likely to access resources to minimize the consequences of diseases, which can ultimately contribute to poorer health outcomes.
Efforts to identify and assess multidomain social risk have grown as evidenced by a recent systematic review indicating broad adoption of screening tools by healthcare systems, particularly in assessing food insecurity, housing instability, and transportation access in relationship to health care utilization outcomes, such as emergency department visits and inpatient admissions 8 Regarding associations between unmet social needs and health conditions, such as diabetes, cardiovascular disease, and COVID-19,9-11 studies have often focused on a single condition despite evidence indicating that these conditions frequently co-occur with behavioral and other physical health conditions.12,13 Although social risk is increasingly assessed across multiple domains, this information is not often analyzed through a multidimensional lens to examine how co-occurring social risk is associated with health outcomes. Current approaches tend to treat these factors as independent and additive rather than interconnected and clustered. 14 Univariate or additive examinations of social risk factors may not fully capture the compounding effect of multiple, intersecting social risks. Multiple intersecting social risks can operate synergistically where challenges in one domain such as financial strain could increase risk in other domains such as food or housing insecurity. These compounded exposures may limit access to care, complicate disease management thereby contributing to poorer health. As such, analytic approaches that leverage data on social risk factors to identify compounding patterns of social risk can enhance our understanding of how multiple risks co-occur and when they may signal categorically higher risk circumstances that can affect health outcomes.
This study utilizes data on social risk factors from a representative sample of the general population in the United States to identify subgroups with distinct social risk profiles using latent class analysis (LCA). We sought to understand the relationship between the identified social risk profiles and self-reported health (SRH). SRH is a widely recognized indicator for general health and has demonstrated predictive power in explaining relationships with adult healthcare outcomes, including morbidity, and mortality.15,16 SRH is also an important indicator for population health and has been integrated into measurement frameworks such as the County Health Rankings Model, as well as national health objectives reflected in Healthy People 2030 to track and monitor overall health and well-being.1,17 Several studies have found associations between food and housing insecurity and poor SRH.18-21 However, to date, we know more about the relationship between isolated social risk factors such as food or housing insecurity and SRH18,20-24 and less about the confluence of social risk, multiple health conditions, and SRH. The present study expands the literature by exploring how social risks commonly cluster and how these clusters are related to health risk.
Methods
Data & Sample
Data from the 2017 Behavioral Risk Factor Surveillance System (BRFSS) were used in this study. The BRFSS is an annual cross-sectional survey that collects data on health outcomes, social risk, health-related risk behaviors, use of preventive services, and chronic conditions from non-institutionalized adults who reside in each of the states and selected US territories. In 2017, the BRFSS conducted a module on SDoH that 17 states opted into including: Colorado, Florida, Georgia, Iowa, Kentucky, Maryland, Massachusetts, Minnesota, Mississippi, New Hampshire, Ohio, Oklahoma, Pennsylvania, Utah, West Virginia, Wisconsin, and Wyoming. 25 Data from these states were extracted to create the dataset for this study. We included data from all these states. Respondents with missing social risk information (N=26,404) were excluded from the LCA analysis. The final analytic sample size for the latent class analysis included 110,028 adults from these states.
Measures
Social Risk Factors
Our LCA included four measures of social risk factors in the BRFSS SDoH module. 25 Housing insecurity was assessed by asking if respondents were unable to pay mortgage, rent, or utility bills in the past 12 months (dichotomized as 0 for no, 1 for yes). Food insecurity was based on asking respondents how often the food they purchased did not last and lacking money to buy more (categorized as 1 for never, 2 for sometimes true, 3 for often true). Stress was assessed by how often respondents reported feeling tense, restless, nervous or anxious in the past 30 days (categorized as 1 for none of the time, 2 for a little of the time, 3 for some of the time, 4 for most of the time). Financial insecurity was based on responses to how respondents’ finances usually work out at the end of the month (categorized as 1 for ending up with money left over, 2 for having just enough money, 3 for not having enough money to make ends meet).
Health Status
The primary outcome of interest, self-rated health (SRH), was assessed using the question: “Would you say that in general your health is - excellent, very good, good, fair, or poor?” Responses were categorized into a binary variable, where excellent, very good, and good were coded as 0, and fair and poor were coded as 1, consistent with previous research. 26
Covariates
In examining the relationship between social risk profiles and SRH, we included health conditions and sociodemographic factors as covariates. A binary indicator for each of the following health conditions was constructed assigning a value of “1” if respondents reported being told by a clinician that they had the condition and “0” otherwise: diabetes, asthma, cancer, stroke, chronic obstructive pulmonary disease, chronic kidney disease, depressive disorders, hypertension, arthritis, obesity, and high cholesterol. A composite variable, number of chronic conditions, was created to measure the prevalence of multiple health conditions. Sociodemographic variables consisted of age, sex, race/ethnicity, income, education, and language preference.
Analysis
LCA was used to identify distinct groups of individuals characterized by similar social risk profiles. LCA is a statistical technique used to identify subgroups or latent classes within a population that share certain characteristics, based on participant responses to categorical indicators. 27 In this study, LCA was employed to identify latent classes based on response patterns to the categorical social risk variables. The analysis was conducted using Mplus Version 8. 28 Model fit statistics, such as the Akaike Information Criteria (AIC) and Bayesian Information Criteria (BIC), were employed to assess model fit and determine the optimal number of classes, ensuring the robustness and validity of our LCA results. Finally, logistic regression was used to examine the association between the identified social risk profiles and SRH adjusting for age, sex, race/ethnicity, income, language preference and number of health conditions. All analyses employed survey weights to account for complex sampling and the combination of surveys from multiple states. 25
Results
The LCA sample consisted of 110,028 observations. Latent classes for social risk profiles were identified by fitting a series of models and the goodness-of-fit indices indicated that a three-class model had the best overall fit (Appendix A). The three-class model demonstrated better fit than the two-class model. Although models with additional classes had lower AIC and BIC values they retained less than 5% of the sample in the smallest class and had lower entropy. Therefore, the three-class model was selected to balance model fit, class size, and interpretability. The three identified latent classes differed in their response patterns, reflecting varying levels of social risk. These profiles were labeled as the Low Social Risk group, the Moderate Financial Strain with Food Insecurity group, and the High Financial Strain with Food and Housing Insecurity group. The predicted probabilities of social risk for each identified profile are displayed in Appendix B. The Low Social Risk profile comprised 75.08% of the sample and was characterized by low probabilities of experiencing social risk across all domains. Adults in this profile had a low probability(P) of being housing insecure (P = 0.003), food insecure (P = 0.006 sometimes; P=0.003 often), experiencing financial strain (P=0.257 just enough money; P=0.005 not enough money), and experiencing stress (P =0.284 a little stress; P=0.127 stressed sometimes; P=0.034 stressed most of the time; P= 0.013 stressed all the time). The Moderate Financial Strain with Food Insecurity group comprised 18.41% of the sample and was characterized by adults with elevated probabilities of having just enough money (P = 0.757) and sometimes experiencing food insecurity (P = 0.30 sometimes; P=0.039 often). These two social risk factors distinguished this profile from the Low Social Risk profile. The probability of experiencing housing insecurity (P=0.158) and stress (P =0.282 a little stress; P= 0.307 stressed sometimes; P=0.133 stressed most of the time; P=0.062 stressed all of the time) also increased in this group relative to the Low Social Risk profile. The High Financial Strain with Food and Housing Insecurity group comprised 6.51% of the sample and reported the highest probabilities of experiencing housing insecurity (P = 0.66), food insecurity (P = 0.366 often; P = 0.453 sometimes), financial strain (P= 0.244 just enough money; P= 0.746 not enough money) and persistent stress (P= 0.111 a little stress; P=0.246 stressed sometimes; P = 0.292 stressed most of the time; P= 0.274 stressed all the time). Figure 1 shows a visual representation of the predicted probabilities of reporting various social risks by the three latent classes. To enhance the interpretability of the radar plot, the category specific probabilities in Appendix B were combined to represent the overall likelihood of experiencing each social risk. For example, food insecurity, combined the probabilities of “often” and “sometimes” experiencing food insecurity. Similarly, financial insecurity combined the predicted probabilities of “have just enough money left over” and “not enough money left over”. Stress combined the predicted probabilities for “a little stress”, “stressed sometimes”, “stressed most of the time” & “stress all of the time”. Graph of latent class profiles
Weighted Descriptive Characteristics of Identified Social Risk Latent Class Profiles

Logistic Regression Results for Association Between Self-Reported Health and Identified Social Risk Profiles
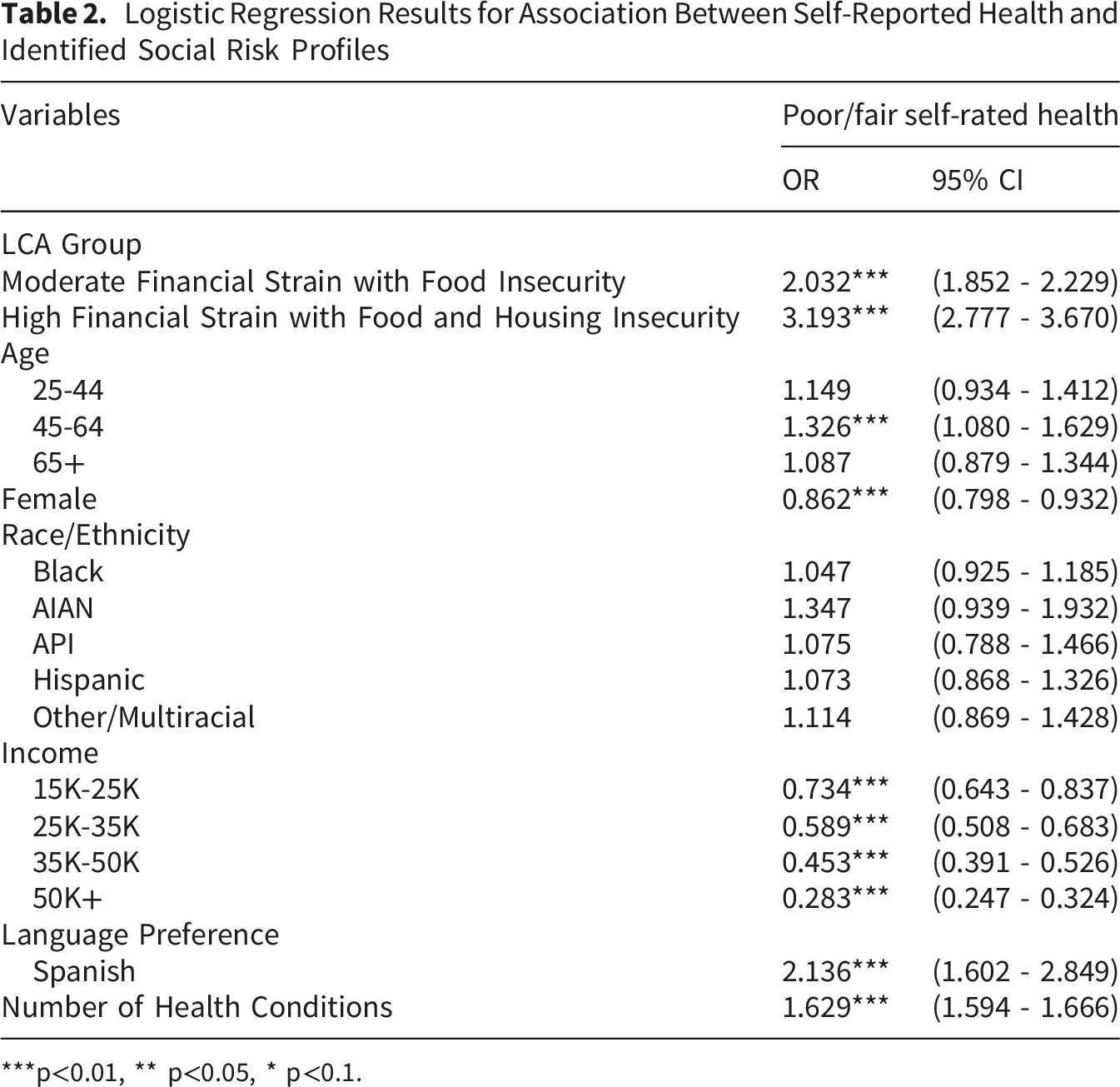
***p<0.01, ** p<0.05, * p<0.1.
Discussion
The profiles identified in this study distinguish individuals who have enough resources to consistently meet their needs from those who have just enough to get by but may sometimes compromise on essentials such as food, and those facing more severe economic precarity that compromises affording stable housing. The findings indicate that social risks do not occur in isolation, instead they cluster in ways that often reflect underlying constraints in economic and social resources. In this context, access to resources play an important role in shaping both vulnerability to risk and the capacity to respond, consistent with theoretical frameworks such as the fundamental cause theory.5-7 The association between compounding social risk and poorer self-rated health observed in this study points to the cumulative burden of socioeconomic disadvantage. Individuals facing multiple overlapping risks such as those adults in the High Financial Strain with Food and Housing Insecurity profile are more likely to experience competing demands that force trade-offs between essential needs such as housing, food, and health. It is worth noting that the association between socioeconomic status and health is not unidirectional, as chronic illness or poor health can limit employment opportunities and income, and this can reinforce exacerbating social and economic hardship. 29 Adults in the Moderate Financial Strain with Food Insecurity profile share a similar prevalence of health conditions as those in the Low Social Risk group suggesting that some adverse health outcomes may be more pronounced at higher levels of economic hardship. The relatively higher cancer prevalence observed among individuals in the Low Social Risk profile likely reflects differences in age composition, access to screening, and survivorship. The cumulative effect of socioeconomic conditions may diminish in older age due to several factors, such as increased access to Medicare and survivorship bias.30,31 Older age remains the strongest risk factor for cancer, and the age composition of this profile (the highest proportion of adults 65+) likely contributes to the observed cancer prevalence. 32
Our regression results further demonstrate a graded association between social risk and SRH. Our findings contribute to the emerging literature on the effects of multiple social risks on health. Leung et al. 19 explored the association between multiple social risk factors among diabetic adults and found that an increase in the number of social risks is associated with greater cost-related medication non-adherence, diabetes distress, and anxiety or depression. Nguyen et al. 33 discussed the combination of food insecurity and lack of social support and its associations with cost-related medication non-adherence among adults with inflammatory bowel diseases. While these disease-specific associations have important implications for developing targeted interventions, the non-disease specific nature of SRH provides insights into the broader effects of social risk exposure on overall general health. Our findings closely corroborate recent work by Nelson et al. 34 who found poorer health was associated with a higher summary social risk score using the Massachusetts BRFSS dataset. Similarly, Rhee et al. 35 assessed the association between a cumulative risk measure for social risk exposures and found significant associations between higher social risk scores and poorer SRH. Taken together, previous work examining individual risk factors provides insight into the effects of a specific social risk while studies exploring cumulative risk scores capture the overall burden of multiple social risks in an additive sense. Our study demonstrates the effects of compounding risk by revealing specific patterns and combinations of multiple co-occurring social risks.
Our findings have implications for policy and practice. The interdependent nature of social risk demonstrated in this study underscores the need for a more comprehensive approach to addressing multiple health-related social risks. In this context, states can adopt strategies to streamline the application and recertification processes for social support programs and implement automatic renewal systems to decrease procedural barriers that hinder access to needed benefits. Additionally, integrated systems that automatically check eligibility for multiple social programs through a single application could further increase and maintain access to needed benefits.
However, programmatic and system level interventions alone are unlikely to substantially reduce disparities without boarder structural change. Our findings illustrate how overlapping social risks manifest in the U.S. adult population. Importantly, these risks tend to cluster in socially patterned ways. 36 We observed greater compounding social risk among adults with lower income and educational attainment, adults identifying as women, and those belonging to racial and ethnic minority groups. These findings reflect structural mechanisms that are deeper processes within the socioeconomic and political context that create and generate social stratification and class division in society through policies or discriminatory practices that ultimately influence socioeconomic position. 36 Although these structural mechanisms were not directly examined in this study, the observed sociodemographic patterns are consistent with established evidence.29,37,38 Thus, addressing compounding social risk not only requires identifying multidimensional need but also confronting the forces that produce and sustain racism, gender-based pay gaps, and unequal access to education, employment, income opportunities, housing and other resources. Further, policy solutions that strengthen employment insurance, access to health care, childcare, and affordable housing could lift individuals out of the economic hardship driving multidimensional social risk and poor health. 39
Limitations
This study has several limitations. A key limitation stems from the cross-sectional BRFSS data and the descriptive nature of the LCA approach. As a result, the observed associations between social risk profiles and health outcomes cannot be interpreted causally as poor health outcomes can exacerbate social risk, and social risk can contribute to poorer health outcomes. Longitudinal designs are needed to clarify the temporal associations in this study. Although the dataset may not fully represent the entire U.S. population, the application of weights in this study to approximate national representativeness strengthens the generalizability of the findings. Additionally, the social risk module in BRFSS is not exhaustive, and as a result did not include other important domains such as transportation access. Since the identified profiles in this analysis are conditional on the included indicators, the omission of other domains may influence the observed patterns of social risk. Transportation barriers often co-occur with financial strain and may represent an additional dimension of material hardship not captured in this study. Future research should incorporate a broader set of social risk factors to strengthen our understanding of multidimensional social need. Related to this, since this health conditions captured in this study may necessitate a clinical diagnosis, there is a possibility of overlooking adults who have not sought healthcare services or lack a consistent source of care. As a result, the prevalence of clinical conditions captured in our sample may be underestimated.
Conclusions
We identified three social risk profiles, illustrating how compounded social risks including housing insecurity, food insecurity, financial strain, and stress cluster together and are associated with health outcomes. By using LCA, our approach builds on previous work using population-level data to capture profiles of co-occurring risks that reflect underlying poverty as a fundamental driver of poor health outcomes. The intensifying hardship observed in the profiles reveal challenges adults face navigating competing needs, such as choosing between housing and food under financial strain. These findings hold relevance amidst recent reductions in public assistance programs, most notably the Supplemental Nutrition Assistance Program (SNAP) that can exacerbate housing insecurity given the interdependent nature of social risk. Beyond this, policy solutions that aim to address health-related social risks should target social needs more comprehensively and include solutions that improve socioeconomic conditions that underly multidimensional social risk and health outcomes.
Supplemental Material
Supplemental material - Patterns of Social Risk Factors and Associations With Health Outcomes: Findings From a Latent Class Analysis
Supplemental material for Patterns of Social Risk Factors and Associations With Health Outcomes: Findings From a Latent Class Analysis by Nicole Pereira, Beth A. Glenn, Adam Schickedanz, Xi Zhu in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We thank Dr. Neal Halfon for their valuable contributions and support in writing this research.
Ethical Considerations
This study used de-identified publicly available secondary data and was exempt from Institutional Review Board (IRB) review.
Consent to Participate
Informed consent was not required.
Author Contributions
Conceptualization: N.P., X.Z., Methodology: N.P., Formal analyses: N.P., Data curation: N.P., Writing-original draft: N.P. Writing editing: N.P. X.Z., B.G., A.S., Visualization: N.P., Supervision: X.Z., B.G., A.S.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.