
Abstract
Introduction
The world’s older adult population is rising rapidly, leading to an increase in mental health problems such as geriatric depression, which has mainly been studied in high-income countries. Similar studies are scarce in low- and middle-income countries like Nepal. So, this study aims to determine the prevalence of depression and its predictors among the older adults living in Sundarharainha Municipality, Morang.
Methods
A cross-sectional, community-based study was conducted using the Validated Nepali version of the Geriatric Depression Scale short form (GDS-15) to identify geriatric depression among the older adults (≥60 years). Those scoring >5 on GDS-15 were considered depressed. Logistic Regression Analysis explored the associations of geriatric depression with potential predictor variables.
Results
Of the 417 selected older adult participants, more than half were males (52.0%), the majority were illiterate (57.6%), and approximately two-thirds were married (66.7%). The prevalence of geriatric depression was found to be 62.4%. Geriatric depression was significantly associated with gender, marital status, level of education, occupation status, limited time provided by families, chronic physical health problems, and exposure to verbal and/or physical abuse. In logistic regression analysis, geriatric depression was significantly associated with educational status (AOR 3.25), family types (AOR 3.75), perceived respect from family (AOR 2.05), financial support (AOR 2.01), sleep quality (AOR 3.26), and seeking professional help (AOR 1.80).
Conclusion
Geriatric depression is highly prevalent in Sundarharaicha Municipality, Nepal. The findings call for the urgent prioritization of the delivery of mental health care services to older adults in the country.

Keywords
Introduction
Depression is one type of psychiatric disorder presented with feelings of depressed mood, lack of interest or pleasure in activities, and energy loss that lasts for two weeks or more. 1 The individuals could also have symptoms including alterations in appetite or weight, sleep, and motoric activity; feelings of triviality or guilt; difficulty thinking, concentrating, or decision making; or persistent thoughts of death or suicide plans or attempts. 2
The world’s population is rapidly aging, and according to the World Health Organization, by 2050 the number of people aged 60 and above is expected to double, from 1 billion in 2020 to 2.1 billion, with two-thirds living in low- and middle-income countries. 3 Mental and neurological disorders in older adults account for 6.6% of the total disability for this age group, and nearly 15% of adults aged 60 and over suffer from a mental disorder, mainly depression.4,5 WHO stated that depressive disorders among older adults ranged between 10 and 20% globally; nearly 300 million people were affected in 2015. 6 As per WHO 2023 data, Mental disorders in older adults account for 10.6% of the total disability for older adults, and approximately 14% of adults aged 60 and over live with a mental disorder. 7
Depression is common in older adults and is a major public health problem. Previous literature emphasizes that depression, which is the fourth most common illness, can lead to physical, emotional, social, and economic problems. 8 The prevalence rate of depression varies worldwide, and prevalence rates range between 28.5% and 80.7%.9,10 A systematic review and meta-analysis done in 2023 found that the global prevalence of major depression in older adults was 13.3 %. 11 A study shows that depression ranges from 27.7% to 47.8% in old-age homes.12,13 Depression in late life is associated with significant morbidity, including deficits in a range of cognitive functions and considerable influence on functional impairment, disability, decreased quality of life, and has a negative effect on the body’s recovery from illness, increases the rate of suicide, increases use of health care services and expenses and can result in early death and disturbance in the general state of wellness.8,14 Depression in older adults is influenced by a variety of biopsychosocial factors, which have been highlighted in recent studies. Factors associated with depression in older adults include biological influences such as age, gender (with higher prevalence in females), and existing health problems; psychosocial factors like lack of social support, financial difficulties, and living alone; and economic challenges, including financial stress and economic inactivity, which collectively contribute to heightened depression risk.15,16
Nepal, despite being one of the least developed countries globally, is experiencing a rapid rise in its older adult population, both in absolute numbers and as a percentage of the total population. According to the 2021 census, the number of older adults in Nepal has reached 2.97 million, reflecting a 38.2% increase from the 2011 census. As a result, the older adults now make up 10.21% of the total population of the country. 17 A recent systematic review and meta-analysis found that the overall prevalence of depression is 52% in the older adult population in Nepal. 18 However, the government has not given priority to identifying the problems of the older adults through research and implementing existing senior citizen acts for the well-being of the older adults.
Limited studies have been done in Nepal to assess the prevalence of depression in older adults, and they have revealed a high prevalence of 45.7% in the emergency department of hospitals, 19 80.7% in old age homes, 9 and 60.6% in the central region. 20 Previous studies from both developed and developing countries have consistently shown that depression is prevalent among older adults, often leading to more days of disability than chronic conditions such as heart disease, hypertension, and diabetes. 21 While previous studies in Nepal have reported high prevalence of geriatric depression, they were largely limited to hospital-based, old-age home, or central-region populations. To the best of our knowledge, this study is the first to provide community-based estimates in Sundarharaicha municipality, eastern Nepal, incorporating comprehensive sociodemographic, household, lifestyle, and family-support factors. By examining these diverse predictors within a local context, the study provides nuanced insights that can guide targeted interventions and inform policy for older adults’ mental health in low-resource urbanizing settings. Therefore, this study aims to assess the prevalence of depression and identify its predictors among the older adult population residing in this community.
Method
Study Design and Setting
A cross-sectional, community-based study was conducted in randomly selected wards of Sundarharaicha Municipality, Morang, Nepal. The study included older adult individuals aged 60 years and above. Sundarharaicha is the second-largest city in Morang District, with 121,305 residents in 26,677 households, about 7% of whom are older adults. It is also one of the fastest-growing cities in eastern Nepal. 22 There are altogether 12 wards in this municipality, which are scattered across 110.6 square kilometers of geographical area. 23
Sample Size and Sampling Technique
The sample size was determined using a prevalence-based estimate calculator, with a 95% confidence interval and a 5% margin of error. 24 Based on a 56% depression prevalence among the older adults, as observed in a previous similar study in Kavre district, 25 the estimated sample size was 379. To account for potential non-responses, an additional 10% was added, resulting in a final sample size of 417 participants.
A multi-stage sampling process was employed to select a total of 417 representative samples at the municipality level. Initially, four wards (4, 5, 7, and 8) were selected randomly. Within each randomly selected ward, households were chosen systematically proportional to ward population, and when multiple eligible older adult individuals were present, one was randomly selected using a lottery method; all approached households participated, yielding a 100% response rate among eligible participants. Eligible older adult individuals were identified using household and population records obtained from the Sundarharaicha Municipality Office. The study included both male and female participants aged 60 and above. Since the household was the sampling unit and the unit of analysis was an individual, one individual was randomly selected using a lottery method from households with more than one older adult. If older adult individuals used different kitchens within the same household, all were included in the sample.
Exclusion criteria included individuals who did not provide informed consent, bedridden older adults who were unable to verbalize themselves, and those who were absent from home during three consecutive visits on different days during the data collection period. Data were collected in a two-week period in February 2024.
Procedure
Data collection was done by trained enumerators through face-to-face interviews with the older adult population above 60 years using a structured interview schedule. The data collection (Supplemental File 1) process was supervised by the research team. The structured interview schedule consists of 6 parts: Socio-Demographic information (age, sex, marital status, religion, ethnicity, education, occupation), Household related information (family type, living with, types of house, current financial situation), lifestyle and behavioral factors (physical exercise, engage in social activities, sleep quality, smoke and alcohol habits), family support factors (respect from the family members, financial support, experience of verbal and physical abuse), physical wellbeing (chronic physical health problems, currently medication for health condition, experience of significant loss or bereavement), and coping and support (availability and use of Briddha chautari, walking distance from home to Briddha chautari). Verbal abuse was defined as any report of being spoken to in a hurtful, insulting, or threatening manner by family members in the past year. Family support was defined as the participant’s perception of receiving emotional, financial, or practical assistance from family members when needed. Social activity was defined as the frequency of participation in community, religious, or leisure activities outside the home, categorized as frequent, occasional, or none. Geriatric Depression Scale short form (GDS-15) in Nepali version was translated by a language expert by considering previously validated Nepali-translated GDS-15,26 and its reliability was calculated by pretest in 10% of the total sample, and Cronbach alpha was found to be 0.86. We used the Geriatric Depression Scale short form (GDS-15) in the Nepali version to scan the potential presence of depressive symptoms. A score of 5 or less was considered to be within the normal range and classified as a “no case” of geriatric depression, while 6 or more endorsements were considered to indicate a case of geriatric depression, according to the tool. 26 Ethical approval to conduct the study was obtained from the Purbanchal University School of Health Sciences-Institutional Review Committee (Ref no. 036-080/81) before conducting the study. The reporting of this study conforms to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement (Supplemental File 2). 27
Statistical Analysis and Software Used
The data were entered using Epi-data Software version 3.1 and analyzed using SPSS version 25. Based on the distribution and variance, appropriate statistical tests were used for analysis. Descriptive analysis was used to describe characteristics. Chi-square (χ2) test was employed to compare the prevalence of depression within different categories of a variable with a 5% level of significance. The depression status of the GDS-15 was used as the dependent variable, and the responses were dichotomized into yes (case of geriatric depression) or no (no case of geriatric depression). Multivariable logistic regression was performed, including both variables found to be significant in the bivariate analysis and key covariates identified a priori based on existing literatures. The variables considered in the regression analysis included gender, marital status, education, occupation, exercise, social activity, sleep, age of the respondents, types of family, close friends to talk about personal matters, time given by family, perceived respect from family, financial support, verbal and/or physical abuse by family, feeling safe at home, chronic physical health problems, seeking professional help for emotional well-being, and living arrangements (family members). This approach was used to adjust for potential confounding factors and enhance the epidemiological validity of the results.
Result
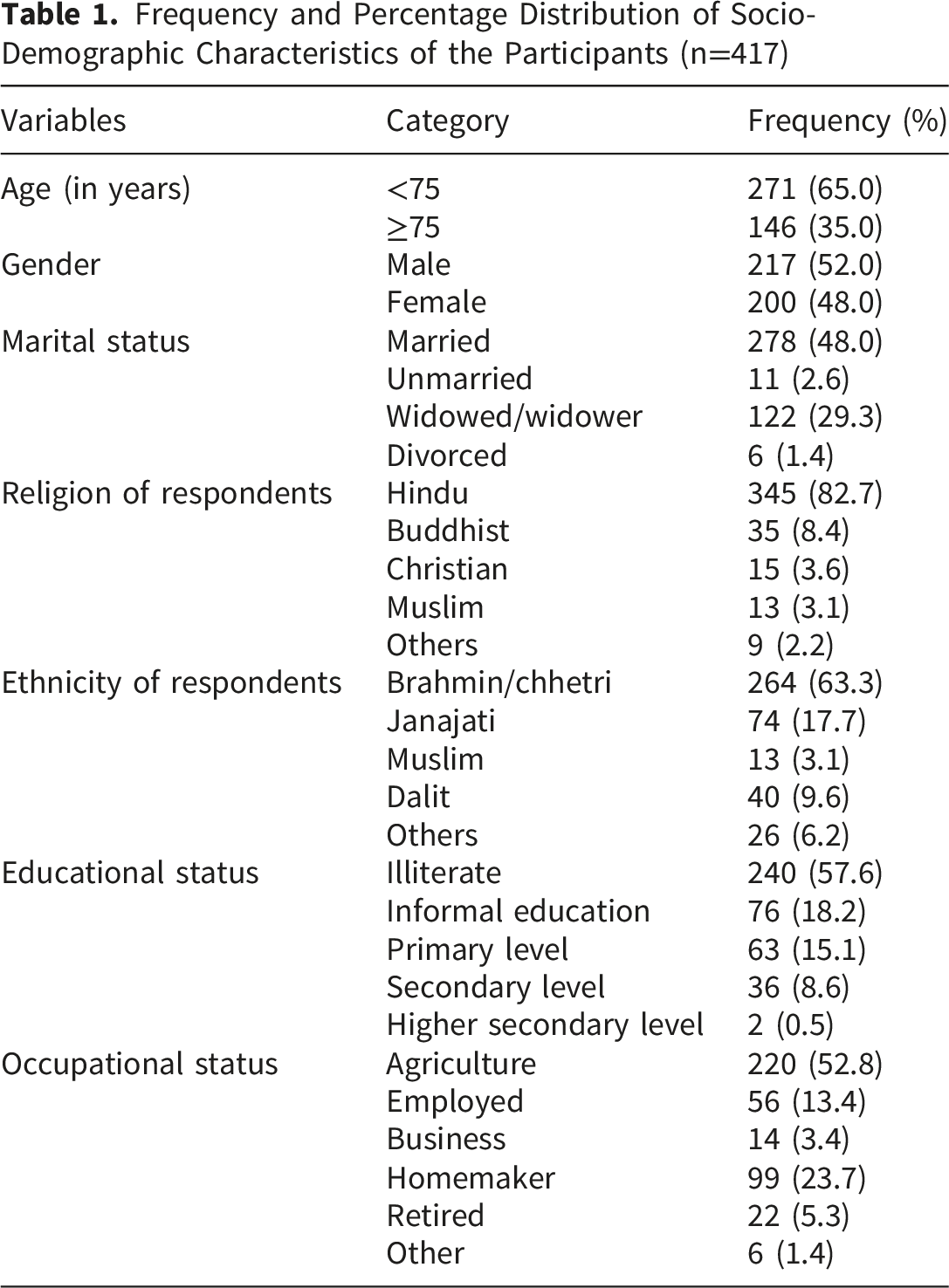
Frequency and Percentage Distribution of Socio-Demographic Characteristics of the Participants (n=417)
Household, Lifestyle and Behavioral Factors, Family Support Factors, Physical Well-Being, Coping and Support Factors Related Information of Participants (n=417)

Association Between Sociodemographic Information, Household-Related Information, Family Support Factors, Lifestyle and Behavioral Factors, Physical Well-Being, Coping and Support Factors, with Prevalence of Older Adults’ Depression

*Significantly associated at p<0.05. f:Frequency.
Table 3 also shows the association of geriatric depression with different variables. Depression among the older adults is significantly associated with Gender, Marital status, Educational status, Occupational status of older adults, type of family, financial situation of older adults, not given time by their family members, not perceived respect from their family members, financial support factor, less engaged in physical exercise and social activity, poor reported sleep quality, chronic physical health problems and those who don’t have close friend to talk about their personal matter.
Bivariable and Multivariable Logistic Regression Analysis of Associations of Geriatric Depression With Significant Predictor Variables
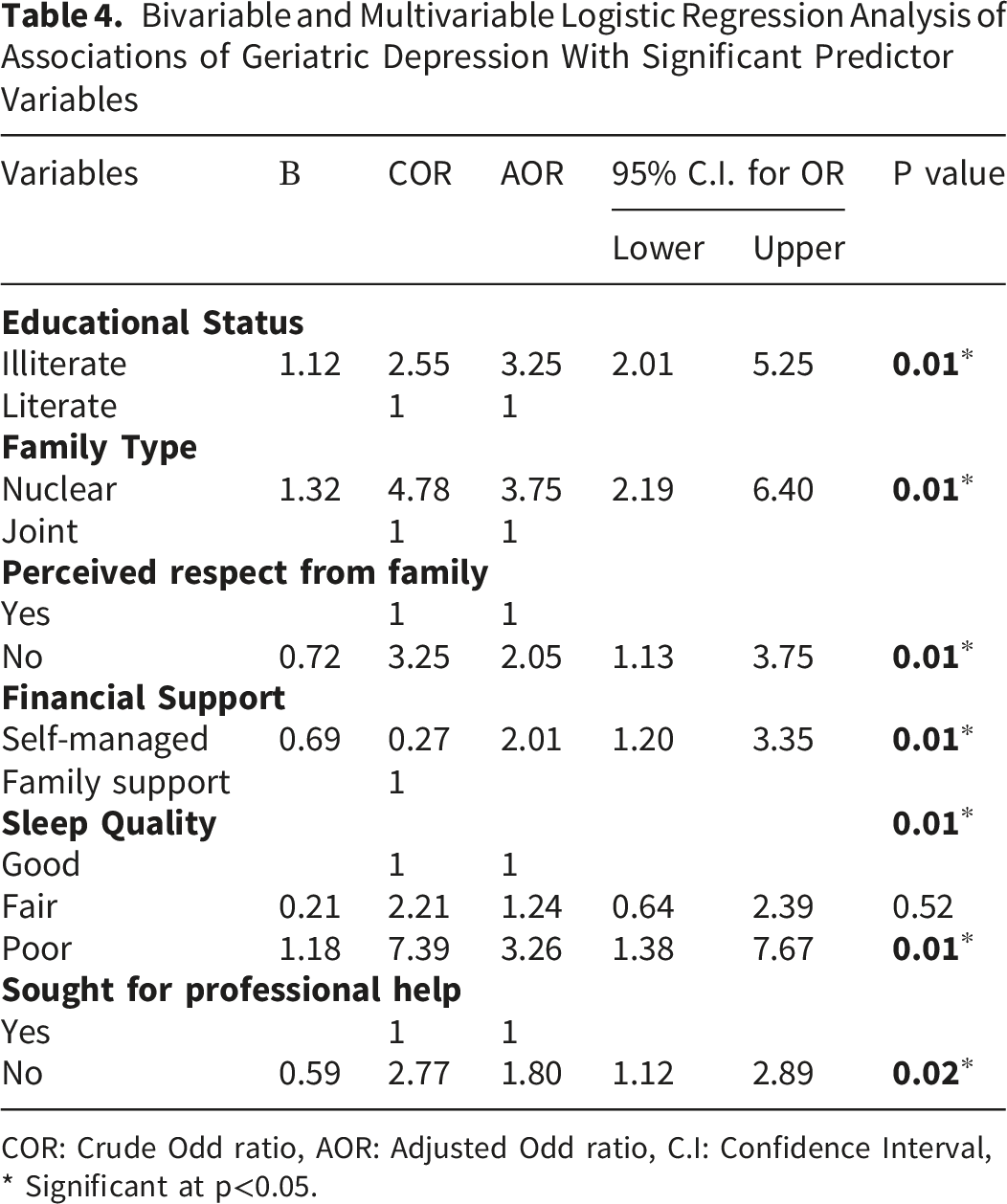
COR: Crude Odd ratio, AOR: Adjusted Odd ratio, C.I: Confidence Interval, * Significant at p<0.05.
The Cox & Snell R2 value of 0.24 and the Nagelkerke R2 value of 0.34 indicate that the model explains approximately 24–34% of the variance in geriatric depression, suggesting a moderate predictive capability for depression status in older adult participants.
Discussion
Sociodemographic information is crucial to our study, as many of these factors significantly influence the prevalence of depression and can serve as key determinants or associated factors in its development. This study showed that the majority of the respondents (65.0%) belong to the age group below 75 years. This finding is similar to the study conducted in Kavre, District, which showed that 69.7% of the respondents belong to the age group below 75 years. 25 Even in the hospital ward setting, older adult patients predominate. 28 Regarding sex, more than half of the respondents were male 52%, which is comparable to the study done in Shivapuri Rural Municipality of Nepal, where the Male population predominates (63.73%). 29 This gender result was inconsistent with the study conducted in the Kavre district, Nepal, where the female population is more prevalent (54.2). 25 This might be due to the variations in gender distribution in different regions of Nepal. The findings of the study showed that more than half of the respondents were illiterate (57.6%), which is found to be higher than the National Population and Housing Census 2021 of Nepal, which reported a 23.8% overall illiteracy rate. 30 However, our illiteracy rate is lower than that of the study conducted in Kavre, District of Nepal (86.1%). 25 This inconsistency reveals variations in literacy rates per geographical location and age groups.
Our study found that more than half of the older adult population in Sundarharaicha Municipality suffered from some degree of depression since the prevalence of Depression was found to be 62.4%. The high prevalence of geriatric depression (62.4%) may reflect both the true burden in this community and the inclusive GDS-15 cut-off (>5), which captures mild to moderate depressive symptoms; this cut-off has been validated in the Nepali older adult population and showed high reliability in pretesting (Cronbach’s α = 0.86). Additionally, this result is also similar to the study conducted in Eastern Nepal, which showed that 65.2% of respondents had such type of depressive disorder. 31 Consistent with our results, population-based evidence from large cohorts demonstrates high prevalence of depressive symptoms among older adults and highlights associations with functional impairment and sociodemographic factors, reinforcing the public health significance of identifying and addressing geriatric depression in community settings. 32 However, The most noticeable finding is that the prevalence of geriatric depression in our study is significantly higher than what has been found in the study conducted in older adults from Australia and the United States, 33 where the prevalence of depression is only 9.8%; this inconsistent results might be due to differences in the instruments(CES-D-10 scale), socioeconomic and cultural differences, level of care provided to older adults and methodological differences. There are also differences in the age ranges and the sociocultural settings in which the studies were conducted.
The risk of having geriatric depression was found to be higher among females, widowed/widower/unmarried/divorced, those who are unemployed, and those who are illiterate. The geriatric depression was also higher among those who reported not being given enough time by their families and among those who reported verbal and/or physical abuse by their families. Furthermore, geriatric depression was more likely to be present among those older adults who had chronic physical health problems, among those who reported no close friends to talk about personal matters, and those who manage their personal expenses themselves. In bivariate logistic regression analysis, respondents who had marital status unmarried were 2.0 times more likely to have depressive syndrome as compared to the married. These all are the factors that were found to be associated with depression in previous literature. 18 Therefore, these factors should be given special consideration while screening for depression and applying targeted interventions.
The regression modelling approach in this study included both variables found to be significant in the bivariate analysis and key covariates identified a priori based on existing literature. Our results underscore the significant associations between educational status, family type, perceived respect from family, financial support, sleep quality, and seeking professional help, which are critical predictors of geriatric depression. This study demonstrated that illiterates were 3.25 times more likely to have depression than literates. This result was in line with a similar cross-sectional study conducted in Kathmandu, 20 Nepal, and Kavre district, Nepal, 25 which demonstrated that Illiteracy is a major predictor of depression. Illiteracy in older adults may contribute to depression by restricting their access to well-paying employment, which can lead to financial insecurity and a lower socio-economic status in later life. This financial strain can result in a diminished sense of control over their environment, a negative perception of social support, and prolonged tension. When combined, these factors generate vulnerabilities that elevate the likelihood of depression. Similarly, Family type is also found to be a strong predictor, in which the older adults living in a nuclear family are 3.75 times as likely to have depression as those living in a joint family. Older adults will receive emotional support from other members of the family if it is a large family, unlike a nuclear family, where most members are engaged in jobs and have less time to relate to older adults. Studies have found that the absence or reduction of close social relationships and social engagement is a significant factor contributing to depression among older adults in Western societies. 34
Concerning chronic health illness, this study showed no significant association between chronic health illness and geriatric depression, whereas a previous study conducted in Kavre 25 and Ethiopia 10 showed a significant association between chronic health illness and geriatric depression. These inconsistent results might be because of differences in the study population, setting, and sample size. In this study, occupation of the respondents was not found to be significantly associated with depression. This finding was similar to the study conducted in Northwest Ethiopia. 35
Recent evidence from LMICs shows a high prevalence of depression, anxiety, and sleep disorders among older adults, 36 consistent with our findings. Community-based interventions, including psychosocial support and low-cost therapy programs, have been effective in reducing depressive symptoms and improving well-being, 37 highlighting the need for culturally adapted public health strategies in Nepal. There is also under-detection and a lack of mental disease screening programs in Nepal, coupled with a lack of efficient health care delivery to older adults. Mental diseases like depression are often concealed in the Nepalese population as they are perceived as having social stigma and deny the condition and don’t seek medical advice and help. Policymakers and healthcare service providers should give more focus on screening mental diseases like depression and apply targeted interventions through a multidisciplinary approach.
Strengths and Limitations
This study has several strengths, including its comprehensive exploration of predictors of geriatric depression, which ultimately improves the quality of life for older adults by reducing the burden of mental illness and promoting mental well-being in later life through targeted interventions. It is the first community-based study in Sundarharaicha Municipality, filling a critical research gap in Eastern Nepal. However, limitations include potential recall bias as some information relied on participants’ memory, limited generalizability to the broader older adult population of Nepal, and the inability to establish causal relationships due to its cross-sectional design. Additionally, excluding bedridden or non-verbal older adults may have led to an underestimation of depression prevalence, and reporting biases could have influenced participants’ responses due to social stigma around mental health.
Conclusion
In Sundarharaicha Municipality, Nepal, geriatric depression is a substantial public health concern, with a high prevalence associated with factors such as illiteracy, living in nuclear families, poor social and familial support, and the presence of chronic physical health conditions. The mental health challenges that older individuals encounter are further exacerbated by poor sleep quality, restricted social engagement, and limited physical activity. These results underscore the pressing necessity for integrated health and social care interventions, such as community-based screening, enhanced family support mechanisms, and targeted mental health programs. In order to address this urgent issue, it is imperative that policymakers and healthcare providers work together to prioritize and support the mental well-being of Nepal’s older adult population through sustainable public health initiatives.
Supplemental Material
Supplemental material - Prevalence and Contributing Factors of Depression Among the Older Adults in Sundarharaincha Municipality of Eastern Nepal
Supplemental material for Prevalence and Contributing Factors of Depression Among the Older Adults in Sundarharaincha Municipality of Eastern Nepal by Pratima Niraula, Binita Kumari Paudel, Rahi Bikram Thapa, Lok Raj Bhatt, Prakash Pathak in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
Supplemental material - Prevalence and Contributing Factors of Depression Among the Older Adults in Sundarharaincha Municipality of Eastern Nepal
Supplemental material for Prevalence and Contributing Factors of Depression Among the Older Adults in Sundarharaincha Municipality of Eastern Nepal by Pratima Niraula, Binita Kumari Paudel, Rahi Bikram Thapa, Lok Raj Bhatt, Prakash Pathak in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgment
We are grateful to the authority of Sundarharaincha Municipality and respective wards for allowing us to conduct this research study, and to all the respondents who participated in this study for their help and cooperation. Furthermore, we extend our heartfelt thanks to Mr. Ravindra Khadka for his excellent creation of the graphical abstract and his continued support.
Ethical Considerations
Ethical approval was received from the Purbanchal University School of Health Sciences-Institutional Review Committee (Ref no. 036-080/81), and permission to collect data was obtained from the municipality and respective wards (Ref no. 979).
Consent to participate
Each participant’s written informed consent was taken before collecting their data. For participants who were illiterate, the informed consent document was read aloud in their presence, and any questions were clarified. Voluntary verbal consent was then obtained, and written consent was documented with a thumbprint on the consent form, in the presence of a witness who also signed to confirm the process. Confidentiality and participants rights were maintained.
CRediT Authorship Contribution Statement
Funding
The authors disclosed receipt of the financial support for the research (fieldwork cost) by Sundarharaicha Municipality [grant number 979].
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data is available from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.