
Abstract
Introduction
Sarcopenia, a progressive skeletal muscle disorder, is common among older adults and is associated with adverse outcomes including falls, fractures, cognitive decline, poor quality of life, and increased mortality. Malnutrition contributes to sarcopenia, and early screening is essential for prevention.
Methods
This cross-sectional study evaluated community-dwelling adults aged ≥65 years in Shanghai. Sarcopenia was diagnosed according to the 2019 Asian Working Group for Sarcopenia (AWGS) consensus, using SARC-CalF, handgrip strength, and bioelectrical impedance analysis. Nutritional status was assessed with MNA-SF and GLIM criteria. Demographics, health, lifestyle, and physical measurements were collected. Logistic regression identified factors associated with sarcopenia. Model calibration was evaluated using the Hosmer-Lemeshow test, multicollinearity via variance inflation factor, and agreement between nutritional tools using the Kappa statistic.
Results
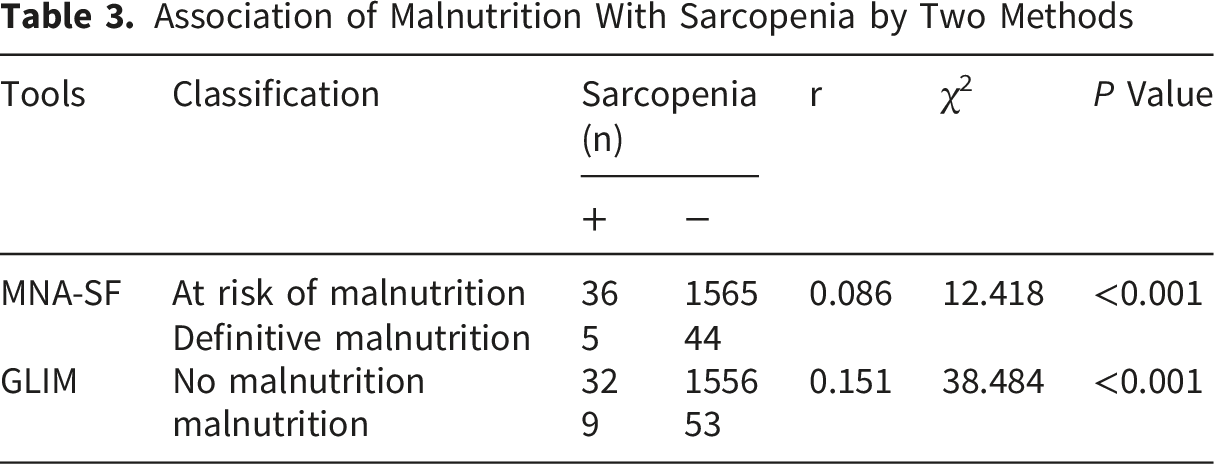
A total of 1,650 adults aged ≥65 years from Shanghai were enrolled in this study. The prevalence of sarcopenia was 2.48% overall (men: 2.42%; women: 2.54%). Independent risk factors included age ≥80 years (OR = 5.089, 95% CI: 2.347–11.037), BMI <18.5 kg/m2 (OR = 4.507, 95% CI: 1.816–11.185), daily sleep <5 h (OR = 3.898, 95% CI: 2.003–7.587), and chronic gastritis (OR = 3.624, 95% CI: 1.234–10.637). Protective factors were BMI ≥24.0 kg/m2 (OR = 0.033, 95% CI: 0.004–0.241) and regular physical exercise (OR = 0.420, 95% CI: 0.216–0.813). Co-occurrence of malnutrition and sarcopenia ranged from 0.30% to 0.55%. Agreement between MNA-SF and GLIM was moderate (Kappa = 0.357, P < 0.001). Their contingency coefficients with sarcopenia were 0.086 and 0.151, respectively (P < 0.05).
Conclusion
In Shanghai community-dwelling older adults, sarcopenia prevalence was 2.48%. Advanced age, low BMI, short sleep, and chronic gastritis increased risk, while higher BMI and regular exercise were protective. Early nutritional assessment and interventions are crucial to prevent sarcopenia.
1. Introduction
Sarcopenia is a progressive and generalized skeletal muscle disorder characterized by decreased muscle mass and accelerated loss of muscle function, commonly occurring in older adults. Sarcopenia in the elderly has become a significant public health problem, with a global prevalence ranging from 10% to 27% in individuals aged over 60 years. 1 The prevalence among community-dwelling older adults in China has reached 17.4%. 2 With advancing age, skeletal muscle mass and strength can decline at a rate of 1%–2% per year, leading to decreased physical function. 3 Sarcopenia is associated with various adverse outcomes, including falls and osteoporotic fractures,4,5 pulmonary insufficiency, 6 sleep disorders, 7 cognitive impairment, 8 poor health-related quality of life, 9 and premature death, 10 imposing a substantial medical and economic burden on patients.
The onset of sarcopenia is insidious and progressively worsens, increasing the risk of adverse clinical outcomes such as falls, frailty, and death in older adults. When sarcopenia coexists with conditions like diabetes, 11 cardiovascular disease, chronic obstructive pulmonary disease, renal dysfunction, 12 and cancer, 13 it can also lead to an increased risk of disease progression, higher risk of disease-related hospitalization, and prolonged hospital stays. 14 Compared to non-sarcopenic individuals, those with sarcopenia have a higher risk of disability and mortality, with a worse prognosis observed in patients with severe sarcopenia.15,16 Reported prevalence of malnutrition risk among community-dwelling older adults in Asia ranges from 16% to 73%, while the prevalence of malnutrition can be as high as 22%. 17 The prevalence of malnutrition and risk of malnutrition among older adults in a Shanghai community were reported as 0.47% and 26.52%, respectively. Nutrition is key to preventing sarcopenia; older adults may experience malnutrition due to factors like inadequate protein intake, leading to muscle atrophy and dysfunction.
Therefore, as a disease prevalent among older adults, early identification of sarcopenia in the community and implementing interventions can help improve the quality of life and physical function of older adults, extend healthcare services into communities, and promote the development of elderly healthcare service systems. Simultaneously, early screening for malnutrition or high risk of malnutrition in older adults allows for timely, reasonable, and effective nutritional interventions to prevent its occurrence or improve nutritional status, increasing benefits for older adults and reducing the incidence of sarcopenia.
Previous studies have identified age, chronic diseases, and physical inactivity as major risk factors for sarcopenia in older adults.18,19 Some of these risk factors can be prevented through lifestyle changes; however, environmental support is needed to maintain or achieve a healthy lifestyle. 20 Emerging evidence suggests that environmental factors may also influence muscle health and physical function in older adults. 21 For instance, neighborhoods with good walkability can promote physical activity, reduce sedentary behavior, and help preserve muscle mass, thereby lowering the risk of frailty. 22 However, research on the association between environmental factors and sarcopenia remains limited and inconclusive. Most existing studies have focused on the broader community environment—such as recreational facilities, walking and cycling infrastructure, and neighborhood aesthetics 21 —while the potential impact of the residential environment has been overlooked. In response, increasing research has focused on the indoor and adjacent residential environments, where older adults spend the majority of their daily time. A study conducted in Shanghai demonstrated that each floor above ground level reduced the likelihood of outdoor trips by approximately one third, suggesting that residential floor level is an important factor to consider. 23 Limited research has examined whether living in walk-up buildings (i.e., buildings without elevators, necessitating regular stair climbing) is associated with sarcopenia among older adults.
The Mini-Nutritional Assessment-Short Form (MNA-SF) 24 is a widely used and validated tool for screening and assessing nutritional status in older adults. The Global Leadership Initiative on Malnutrition (GLIM) criteria were released by nutrition experts from various countries in 2019 to maintain a consensus on malnutrition diagnosis. 25 Evidence from hospital-based studies suggests that agreement between MNA tools and GLIM criteria is often suboptimal, ranging from poor to moderate,26,27 but such data in community-dwelling populations are limited, and the relationship between malnutrition diagnosed by these tools and sarcopenia risk remains to be elucidated.
This study was designed to fill critical gaps in the understanding of sarcopenia among community-dwelling older adults. We hypothesized that sarcopenia risk is influenced by a constellation of modifiable factors—including nutritional status, lifestyle behaviors, and housing characteristics—and that the two commonly used nutritional assessment tools (MNA-SF and GLIM) would exhibit significant yet imperfect agreement. By investigating prevalence, associated factors, and tool performance in a Shanghai cohort, we aimed to provide evidence that can inform targeted, multi-domain prevention strategies.
2. Materials and Methods
2.1. Study Design and Participants
This cross-sectional study was conducted among older adults who underwent community health examinations at the Changshou Community Health Service Center, Putuo District, Shanghai, between February 24 and March 28, 2025. Eligible participants were those aged 65 years or older, who provided informed consent, and were cognitively intact, able to communicate clearly, and cooperative with the survey procedures. Participants were excluded if they were unable to undergo multifrequency bioelectrical impedance analysis (BIA), such as those with prostheses, inability to stand steadily, or implanted medical devices including cardiac pacemakers, stents, metal plates, or screws. Additional exclusion criteria included impaired consciousness or inability to communicate, refusal to participate, and incomplete surveys or missing data.
This study is reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline for cross-sectional studies. 28
2.2. Sampling Method and Sample Size
A convenience sampling method was adopted. The minimum sample size was calculated as 217 participants based on the formula for cross-sectional prevalence studies, assuming a sarcopenia prevalence of 17.4%, 2 a margin of error of 0.05, and a 95% confidence level.
2.3. General Information Questionnaire
A self-designed questionnaire, developed by the researchers based on relevant literature, was used to collect baseline information. The questionnaire consisted of four parts: (1) demographic characteristics, including age, sex, educational level, and marital status; (2) health status, including presence and number of chronic diseases; and (3) physical examination data, including weight (WT), height (HT), calf circumference (CC), body mass index (BMI), and appendicular skeletal muscle mass index. The diagnostic criteria for overweight and obesity in China differ from those in western countries. 29 According to the Chinese BMI classification,30,31 underweight was defined as <18.5 kg/m2, normal weight as 18.5 to <24 kg/m2, overweight as 24 to <28 kg/m2, and obesity as ≥28 kg/m2.
2.4. Nutritional Status Assessment
2.4.1. Nutritional Status was Evaluated Using Two Approaches
2.4.1.1. Mini-Nutritional Assessment-Short Form (MNA-SF)
MNA-SF includes 6 items: weight loss in the past 3 months, stress/acute disease, dietary change, BMI, mobility, and neuropsychological problems, with a total score of 14. A score of 12–14 indicates normal nutritional status; 8–11 indicates risk of malnutrition; and 0–7 indicates definite malnutrition.
2.4.1.2. Global Leadership Initiative on Malnutrition (GLIM) Criteria
The GLIM criteria include three phenotypic components (non-volitional weight loss, low BMI, and reduced muscle mass) and two etiologic components (reduced food intake or assimilation and disease/inflammation burden). 27 A diagnosis of malnutrition requires the presence of at least one phenotypic and one etiologic criterion. Severity of malnutrition is further stratified according to GLIM recommendations.
2.5. Sarcopenia Screening and Diagnosis
Sarcopenia was assessed according to the 2019 Asian Working Group for Sarcopenia (AWGS) consensus. 32 Initial screening was performed using the SARC-CalF questionnaire (SARC-F combined with calf circumference), with a score ≥11 considered positive. This was followed by handgrip strength testing (cut-off: <28 kg for men, <18 kg for women). Those with both positive SARC-CalF and low handgrip strength were further assessed for skeletal muscle mass using bioelectrical impedance analysis (BIA) with a body composition analyzer (Tsinghua Tongfang BCA-2A, China).
2.5.1. Calf Circumference Measurement
Participants were seated with their trunk upright, legs apart, calves relaxed naturally, feet flat on the floor, and thighs and calves forming a 90° angle. A non-stretchable tape measure was used to measure the circumference of the thickest part of the non-dominant calf.
2.5.2. Handgrip Strength Test
Participants stood during the test. They used their dominant hand to grip the dynamometer with maximum force. The test was performed at least twice, maintaining grip for 3 seconds each time, and the maximum value was recorded.
2.5.3. Bioelectrical Impedance Analysis
Prior to measurement, subjects were required to adhere to the following preparation protocols: they needed to fast for 2 to 4 hours, empty their bladder, and refrain from vigorous exercise within 12 hours before the test. During the measurement, subjects had to remove metallic accessories such as watches and bracelets. They stood barefoot on the activated Tsinghua Tongfang body composition analyzer (Tsinghua Tongfang BCA-2A, China), ensuring that the forefoot and heel of both feet were in full contact with the metal electrode plates. After the weight reading stabilized, they accurately entered their ID number, age, sex, and height on the touchscreen. Subsequently, subjects held the handles with both hands, pressing the top electrodes with their thumbs and gripping the lower electrodes with the other four fingers, while extending both arms approximately 30 degrees away from the body and allowing them to hang naturally in a relaxed state. Upon pressing “Start,” subjects remained still and silent for approximately 20 to 40 seconds until the screen indicated the test was complete. The device then automatically saved the data and could print a report. Sarcopenia was diagnosed when skeletal muscle mass index (SMI) was <7.0 kg/m2 in men or <5.7 kg/m2 in women.
2.6. Statistical Analysis
Data were analyzed using SPSS Statistics version 26. Categorical variables were expressed as frequencies and percentages. Group comparisons were performed using the chi-square test or Fisher’s exact test. Variables with statistical significance in univariate analysis were entered into multivariate logistic regression analysis. For lifestyle factors including smoking, drinking, coffee or tea consumption, and regular physical exercise, participants were asked to report their habits as ‘yes’ or ‘no’. These responses were recorded as binary variables (1 = yes, 0 = no) for subsequent analyses.
The Hosmer-Lemeshow goodness-of-fit test was used to assess the calibration of the final model. A p value greater than 0.05 indicates a well-fitted model. To assess multicollinearity among the independent variables in the final model, we calculated the Variance Inflation Factor (VIF). A VIF value greater than 10 (or a more conservative threshold of 5) was considered indicative of problematic multicollinearity. Consistency was evaluated using the chi-square test and Kappa statistic. A p value of less than 0.05 was regarded as being statistically significant.
2.7. Sensitivity Analysis
To examine whether our findings were influenced by participants with a high burden of multimorbidity, we performed a sensitivity analysis restricted to participants with fewer than three chronic diseases. The multivariate logistic regression model, including all variables identified in the primary analysis, was refitted in this subsample.
3. Results
3.1. Prevalence of Sarcopenia
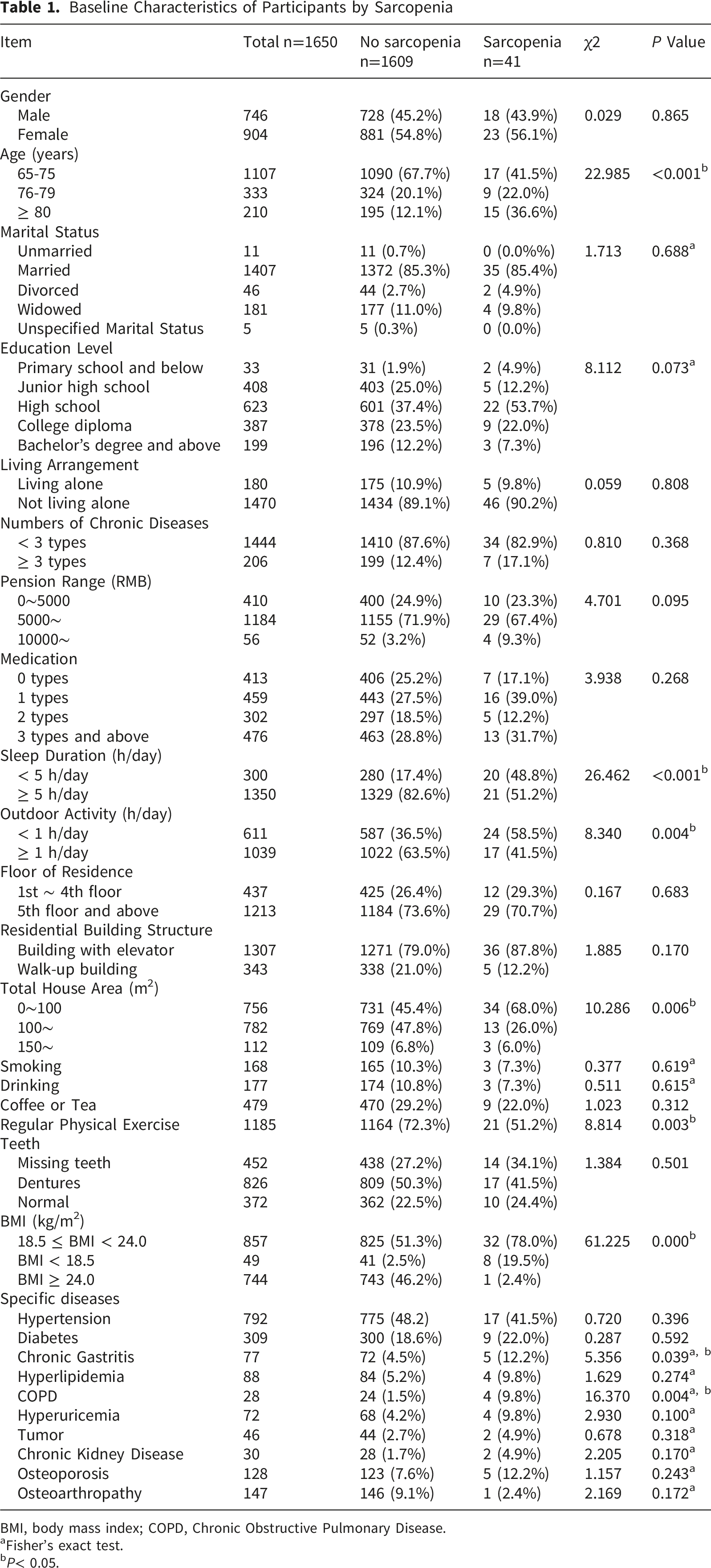
A total of 1,650 older adults participated in the study (746 men and 904 women); 67.1% were 65–75 years old, 20.2% were 76–79 years old, and 12.7% were aged 80 years or above. The overall prevalence of sarcopenia was 2.48% (41/1650), with no significant difference between men (2.42%) and women (2.54%) (P = 0.865) (Figure 1, Table 1). Flowchart Baseline Characteristics of Participants by Sarcopenia BMI, body mass index; COPD, Chronic Obstructive Pulmonary Disease. aFisher’s exact test. bP< 0.05.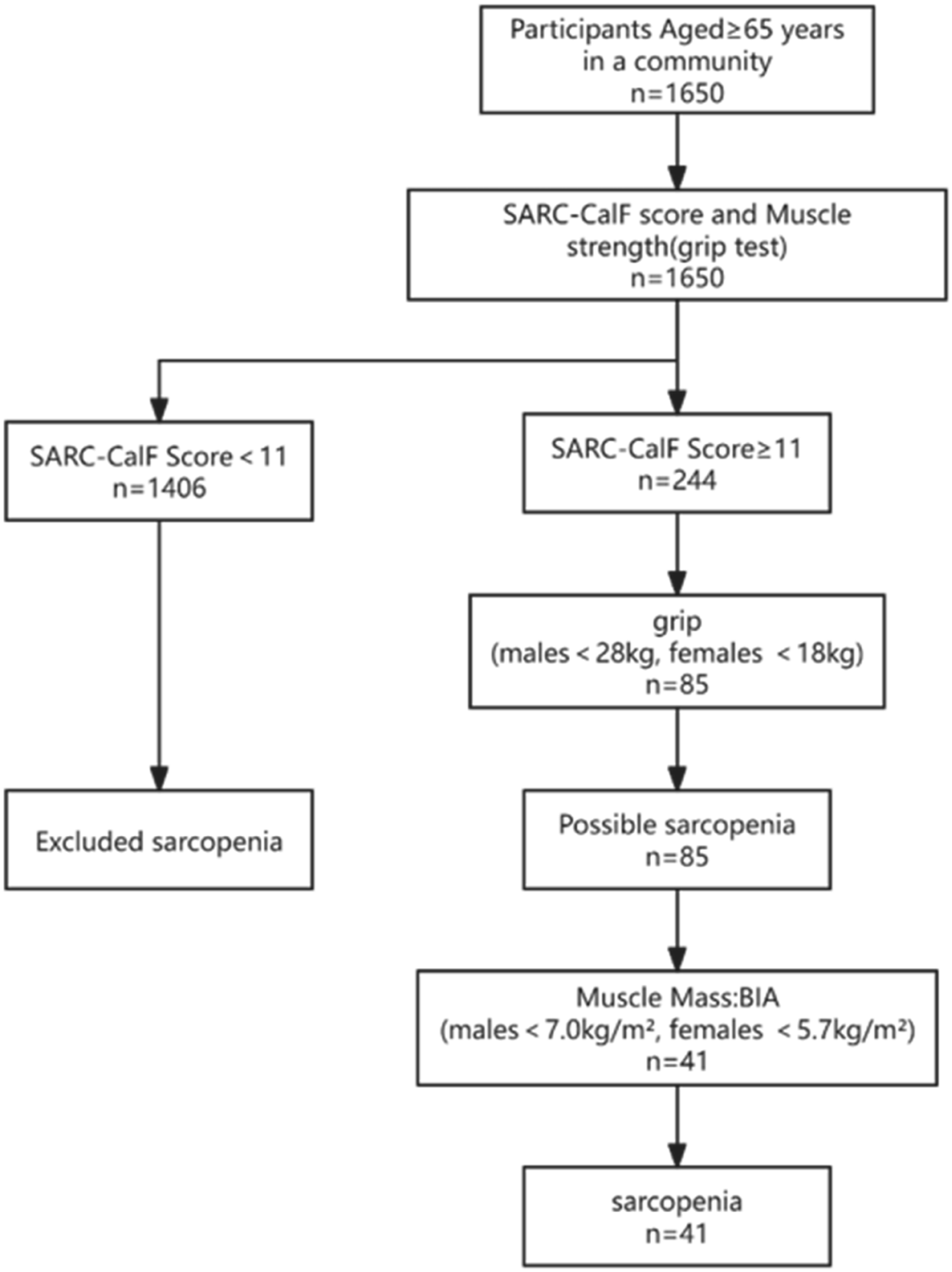
3.2. Factors Associated With Sarcopenia in Older Adults
Participants with sarcopenia were significantly older than those without sarcopenia, particularly in the ≥80 years group (36.6% vs. 12.1%, P < 0.001). No differences were found in marital status, education level, living arrangement, number of chronic diseases, medications or pension range (all P > 0.05).
Lifestyle characteristics showed significant differences. A greater proportion of sarcopenic participants reported short sleep duration (<5 h/day: 48.8% vs. 17.4%, P < 0.001), less outdoor activity (<1 h/day: 58.5% vs. 36.5%, P = 0.004), and a lower prevalence of regular physical exercise (51.2% vs. 72.3%, P = 0.003).
Environmental factors also played a role. Sarcopenic participants were more likely to live in smaller houses (<100 m2: 68.0% vs. 45.4%, P = 0.006). However, no significant differences were observed in floor of residence or building structure.
BMI distribution differed markedly between groups (P < 0.001). Sarcopenia was more frequent in participants with BMI <18.5 kg/m2 (19.5% vs. 2.5%), while only 2.4% of sarcopenic participants had BMI ≥24.0 compared with 46.2% in the non-sarcopenia group.
Regarding chronic diseases, chronic gastritis (12.2% vs. 4.5%, P = 0.039) and COPD (9.8% vs. 1.5%, P = 0.004) were more common in participants with sarcopenia, whereas no significant differences were observed for hypertension, diabetes, hyperlipidemia, hyperuricemia, chronic kidney disease, osteoporosis, or osteoarthropathy (all P > 0.05).
Multivariate Logistic Regression Analysis
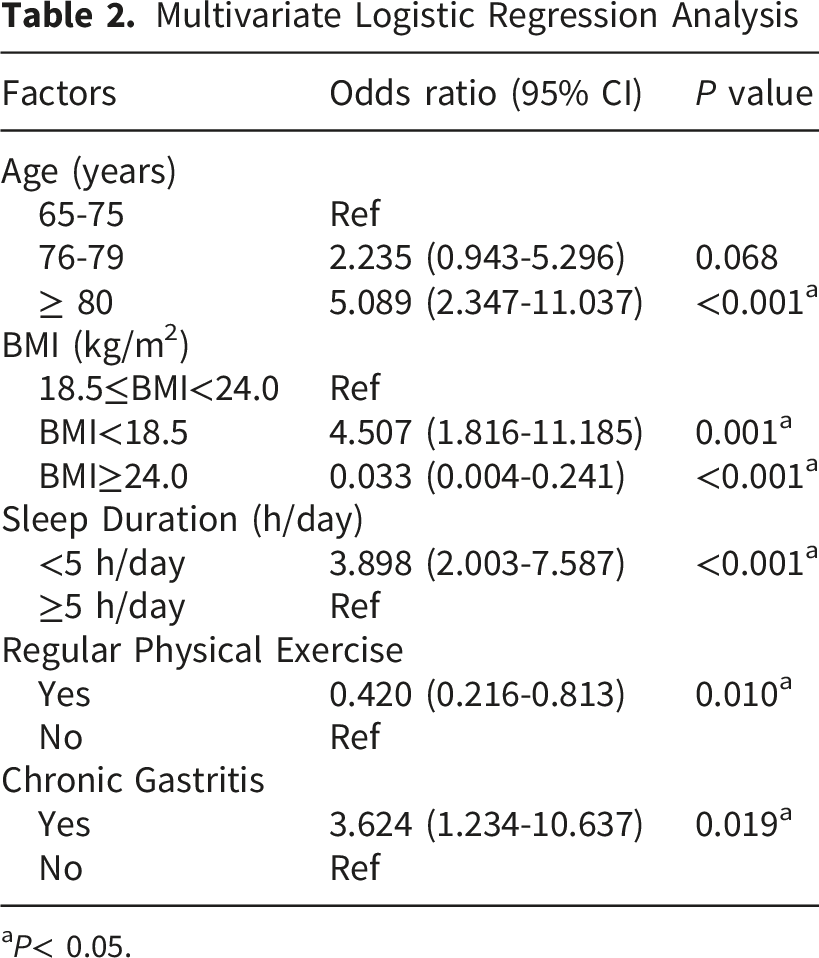
aP< 0.05.
The Hosmer–Lemeshow goodness-of-fit test suggested that the model was well-calibrated (P > 0.05). The Variance Inflation Factor (VIF) for all variables ranged from 1.003 to 1.012, which is well below the commonly accepted threshold of 5 (or 10). This indicates that multicollinearity was not a concern in our analysis, and the estimated regression coefficients are stable and reliable.
3.3. Sensitivity Analysis
In the sensitivity analysis restricted to participants with fewer than three chronic diseases (n = 1444, sarcopenia cases = 34), the results were consistent with the primary findings. Age ≥80 years (OR = 5.236, 95% CI: 2.233–12.279, P < 0.001), age 76–80 years (OR = 2.934, 95% CI: 1.189–7.236, P=0.019), BMI <18.5 kg/m2 (OR = 5.375, 95% CI: 2.041–14.157, P < 0.001), and short sleep duration (OR = 3.265, 95% CI: 1.571–6.867, P = 0.002) remained significant risk factors, while BMI ≥24.0 kg/m2 (OR = 0.043, 95% CI: 0.006–0.317, P = 0.002) remained protective. These findings confirm that the associations observed in the primary analysis are robust and not driven by participants with higher comorbidity burden.
3.4. Nutritional Status
Based on MNA-SF, 49 participants had definite malnutrition (score 0–7), including 5 with sarcopenia (prevalence 2.97%; co-occurrence 0.30%). Using the GLIM criteria, 62 participants were diagnosed with malnutrition, 9 of whom had sarcopenia (prevalence 3.76%; co-occurrence 0.55%).
Association of Malnutrition With Sarcopenia by Two Methods
4. Discussion
In this cross-sectional study of 1,650 community-dwelling older adults in Shanghai, the prevalence of sarcopenia was 2.48%, with no significant difference between men and women. The prevalence of sarcopenia observed in our study is considerably lower than the 10–20% range typically reported in Chinese community-dwelling older adults.2,19,33This discrepancy is likely attributable to a combination of methodological and population-related factors. Firstly, the BIA method tends to yield higher estimates of muscle mass, and therefore lower estimates of the prevalence of sarcopenia than the DXA method. 34 In our study, the diagnosis of sarcopenia was conducted in a standing position using a multi-frequency BIA device (Tianjin Tongfang BCA-2A). Studies have shown that the BIA measurements in the standing position are highly consistent with those in the supine position and with dual-energy X-ray absorptiometry (DXA) in the Chinese elderly population. However, due to the use of the instrument, those elderly people who were unable to stand stably were excluded from our study, which undeniably may have led to an underestimation of the prevalence. Secondly, our study population, recruited from routine community health examinations, likely represents a more health-conscious and higher-functioning subset of older adults, as reflected in the high rate of regular exercise (71.8%). Additionally, the AWGS 2019 sequential screening protocol prioritizes feasibility over diagnostic sensitivity; consequently, individuals with low muscle mass but normal screening results may have been missed. 35
Our diagnosis of sarcopenia relied on low muscle mass and low handgrip strength, excluding physical performance measures such as gait speed. This decision was grounded in the recognition that physical function is a manifestation of disease outcome rather than a core diagnostic feature. Notably, this aligns with the AWGS 2025 consensus update, 36 which redefined physical performance (e.g., gait speed, chair stand test) as an outcome indicator rather than a diagnostic criterion.
Consistent with our hypothesis, multiple modifiable factors were independently associated with sarcopenia. Advanced age was strongly linked to sarcopenia. Prevalence rose sharply in those aged 80 years and older. This finding matches evidence that muscle fibers are gradually replaced by fibrous or fatty tissue, and that oxidative damage increases. These changes put older adults at a higher risk for sarcopenia.37,38 Underweight participants (BMI <18.5 kg/m2) had a significantly higher risk, while overweight status (BMI ≥24.0 kg/m2) appeared protective. These findings align with prior studies showing that low BMI increases susceptibility to malnutrition and muscle wasting, whereas higher BMI may buffer against sarcopenia.39,40 Individuals with higher fat mass might have higher protein intake, offering some protection against sarcopenia. 41 However, obesity-related fat accumulation may also coexist with muscle loss, and sarcopenic obesity remains a concern. Sarcopenic obesity in older adults is also associated with various adverse outcomes. 14 Short sleep duration (<5 h/day) was identified as an independent risk factor. Adequate sleep is crucial for rejuvenation, while excessively long or short duration can lead to metabolic dysregulation, resulting reduced muscle mass and physical function. 42 Both short and long sleep durations have been positively associated with the risk of sarcopenia; other sleep-related characteristics, such as poor sleep quality and insomnia, warrant further investigation. 14 Similarly, reduced outdoor activity and lower prevalence of regular exercise were more common among sarcopenic participants. The protective effect of regular physical exercise (OR = 0.420) reinforces the importance of lifestyle interventions, particularly resistance training, which promotes muscle protein synthesis and improves mitochondrial function. These results underscore the importance of maintaining adequate sleep and physical activity in older adults. 43 For older adults who remain independent in daily activities, living in stair-access housing environments may play a protective role against frailty, according to emerging evidence. 44 Although no differences were observed for floor of residence or elevator availability in our study, these variables may influence daily mobility and functional capacity, and warrant further investigation. The results may be limited by the sample size and the single-center study. Among chronic diseases, chronic gastritis and COPD were significantly associated with sarcopenia. Chronic gastritis can impair nutrient absorption, particularly protein and micronutrients essential for muscle synthesis, while COPD is known to promote muscle wasting through systemic inflammation and reduced physical activity. Other chronic conditions such as hypertension, diabetes, and osteoporosis showed no significant associations in our study, suggesting that their effects may be mediated by intermediate pathways or attenuated by the relatively low prevalence of sarcopenia in this population.
The prevalence of malnutrition among community-dwelling older adults varies based on the screening tools applied and the characteristics of the population studied. In our study, the prevalence of malnutrition ranged from 2.97% (MNA-SF) to 3.76% (GLIM), yet the overlap between the two classifications was limited. This suggests that relying on a single tool may lead to misclassification of nutritional risk. The literature shows considerable variability in the agreement between MNA-SF and GLIM across different populations. In community-dwelling older adults, Win et al. 45 reported a low agreement (kappa = 0.26–0.32) in the Singapore Longitudinal Aging Study, suggesting that the two tools capture distinct dimensions of nutritional risk in relatively healthy older populations. Conversely, studies in hospitalized older adults have reported moderate to high agreement between MNA-SF and GLIM, with kappa values of 0.668 46 and 0.629, 27 respectively. The two tools may converge more closely in clinical populations with higher nutritional vulnerability. Our observed moderate agreement (kappa = 0.357) falls between these two estimates, reinforcing the concept that the concordance between MNA-SF and GLIM is not fixed but varies with population characteristics. This highlights the importance of considering the clinical context when interpreting nutritional assessments and supports the complementary use of both tools in community settings to achieve a more comprehensive evaluation of nutritional status.
The co-occurrence of malnutrition and sarcopenia was low, ranging from 0.30% (MNA-SF) to 0.55% (GLIM). This low co-occurrence aligns with the weak contingency coefficients (0.086 and 0.151) observed between malnutrition and sarcopenia, suggesting that malnutrition alone does not account for the majority of sarcopenia cases. The fact that only a small proportion of sarcopenic individuals were identified as malnourished by either tool suggests that relying solely on nutritional status to identify sarcopenia risk would miss a substantial number of at-risk older adults. These findings underscore the multifactorial etiology of sarcopenia, consistent with the broader literature. While malnutrition is an established contributor to muscle loss, our results indicate that other factors—such as advanced age, low BMI, short sleep, and chronic gastritis—play equally important roles. From a clinical perspective, this implies that screening for sarcopenia should not be limited to individuals with overt malnutrition; rather, a broader assessment encompassing nutritional, lifestyle, and clinical factors is warranted. Importantly, several of these factors are modifiable, offering potential targets for community-based prevention strategies. Early nutritional assessment, promotion of balanced diet, encouragement of resistance exercise, adequate sleep hygiene, and management of gastrointestinal disorders may help reduce the burden of sarcopenia in community settings. Nutritional screening using both MNA-SF and GLIM criteria can guide timely interventions to improve overall health outcomes.
This study has several limitations. Given the limited number of sarcopenia cases (n = 41), statistical power may have been constrained. Selection bias may have arisen from two sources: recruitment from routine health examinations at a single community health center, and exclusion criteria related to BIA measurement that systematically excluded frailer individuals (e.g., those with implanted devices or unable to stand unassisted). Future research should employ more representative sampling strategies (e.g., multi-center recruitment) and alternative body composition assessment methods (e.g., dual-energy X-ray absorptiometry [DXA]) to validate and extend our findings.
5. Conclusions
This cross-sectional study found a sarcopenia prevalence of 2.48% in community-dwelling older adults. Modifiable risk factors (low BMI, short sleep, chronic gastritis, physical inactivity) and protective factors (higher BMI, regular exercise) were identified, offering actionable targets for community prevention. The findings of this study should be interpreted with caution given the modest number of sarcopenia cases and the potential for selection bias. The moderate agreement between MNA-SF and GLIM suggests these tools capture different nutritional risk dimensions and may be complementary in screening. These findings reinforce the multifactorial nature of sarcopenia and support integrated prevention strategies addressing nutritional, lifestyle, and clinical factors. Further longitudinal and adequately powered studies are needed to establish causality and to determine the generalizability of these findings beyond relatively healthy community-dwelling older adults.
Footnotes
Ethical Considerations
Consent to Participate
All participants signed an informed consent form at the time of participation. The study followed the guidelines of the Declaration of Helsinki.
Consent for Publication
All participants provided informed consent for participation and publication of anonymized data.
Author Contributions
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded in part by Shanghai Municipal Health System Key Discipline—General Surgery (2024ZDXK0044), Shanghai Municipal Health Commission Clinical Research Project (202540062), and Shanghai Putuo People’s Hospital Talent Development Program (2025AX03).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.