
Abstract
Introduction
Seafarers face substantial mental health challenges related to isolation, high workloads, and limited access to support, with 77% of surveyed seafarers reporting at least one mental health problem such as sleep disorders, anxiety, or loneliness onboard.
Methods
Drawing on the Triple Helix model, through a weighted ratio indicator analysis, this study examines how three stakeholder groups, seafarers, employers, and psychological service providers, perceive seafarers’ mental health challenges and the availability and use of support interventions, based on an online questionnaire completed by 106 respondents (48 seafarers, 44 employers, 14 service providers).
Results
Findings reveal marked misalignment between stakeholders’ understanding of psychological safety, low utilization of available mental health services, and a pronounced imbalance between demand for psychological support and its supply and uptake in employers.
Conclusion
The study’s major contribution is to demonstrate, through an integrated supply–demand analysis, where gaps arise between seafarers’ needs, market offerings, and employers’ implementation practices, and to propose evidence-based recommendations for strengthening regulatory frameworks, enhancing stakeholders’ dialog and collaboration, and contextualizing appropriate training and service provision to strengthen psychological safety and mental well-being at sea.
Keywords
Seafarers face unique psychological stressors due to the nature of maritime work. They have direct health, safety, well-being consequences on seafarers and influence seafarers’ retention rates. However, existing conventions such as Convention on Standards of Training, Certification, and Watchkeeping for Seafarers (STCW) and the Maritime Labor Convention (MLC) insufficiently address psychological safety, leaving it in an ambiguous regulatory space. There is a gap in research on the issue of mismatch between welfare provisions and actual use of them. This study provides empirical evidence from seafarers, employers, and service providers, revealing significant misalignments between mental health service demand, provision, and utilization. The use of weighted ratio indicators ensures comparability across groups and offers a novel methodological contribution. It also integrates qualitative insights showing that organizational practices, not only individual factors, drive mental health challenges. The findings support psychological safety theory by highlighting the role of leadership, organizational conditions, and multi-stakeholder dialogue and cooperation in shaping well-being at sea. Practically, they call for embedding mental health within ISM Code safety systems and prioritizing interventions aligned with seafarers’ actual needs. Policy implications include revising STCW and MLC to mandate mental health awareness as core competencies.Highlights
What Do We Already Know About This Topic?
How Does Your Research Contribute to the Field?
What Are Your Research’s Implications for Theory, Practice, or Policy?
Introduction
The maritime industry, the backbone of global trade, operates under physically and psychologically demanding working conditions. Long deployments, isolation, limited social contact, unpredictable schedules, and rigid hierarchical structures contribute to elevated stress and mental health disorders in seafarers, who are vital to global supply chains. 1 Mental health, as defined by the World Health Organization 2 is a state enabling individuals to cope with life’s stresses, realize their abilities, work well, and contribute to their communities. Psychological safety, defined as the shared belief that individuals can express concerns, admit mistakes, and seek support without fear of negative consequences, 3 extends beyond individual mental health to encompass the collective climate within organizations. The two concepts are interrelated: insufficient psychological safety can increase stress in individuals and lead to mental health problems. Such conditions might affect decision-making, increase possibility of human error, and compromise safety. This can influence seafarers’ job satisfaction, career decisions, and retention in the industry.
While other high-risk sectors such as aviation, offshore oil and gas, and construction industries4-6 share characteristics, such as remote operations and demanding schedules, the maritime industry presents a uniquely isolated environment where crews work and rest together for extended periods without access to shore-based psychological support. The COVID-19 further exposed this vulnerability, as crew change crises and prolonged time at sea intensified isolation, anxiety, and depression, highlighting long-standing gaps in mental health provisions for seafarers. In the maritime context, with existing hierarchical command structures, multicultural teams, and limited connectivity, adequate psychological safety strengthens operational performance and vessel safety by promoting communication, collaboration, and proactive risk reporting.7,8 These conditions underscore the need to move beyond documenting individual stressors toward understanding how systemic factors and organizational arrangements, including diverse support services and interventions such as training courses, social support, and e-counseling, 9 shape psychological safety at sea.
Given that safety culture plays a pivotal role in mediating mental health and access to resources, strengthening international regulatory frameworks is essential. A positive safety culture, characterized by open communication, mutual trust, and non-punitive reporting, encourages seafarers to seek help and ensures that psychological safety is recognized as part of overall occupational safety. Such environments encourage seafarers to seek help and reduce barriers to report concerns. In contrary, in where stigma, fear of blame, or hierarchical barriers prevail, mental health issues often remain hidden and unreported, and access to support remains limited.10,11 Addressing mental health issues must be seen as integral to safety management and training systems and regulatory frameworks rather treated than as a separate welfare issue. Key maritime conventions, such as the International Convention on Standards of Training, Certification, and Watchkeeping for Seafarers (STCW) 12 and the Maritime Labor Convention (MLC) 13 lack clear provisions targeting psychological safety and mandatory mental health training for crews. The International Maritime Organization (IMO) and International Labor Organization (ILO) have begun to address this regulatory gap through recent policy discussions and updates, 14 culminating in recent initiatives related to harassment and shore leave. These developments reflect a gradual but meaningful shift toward embedding psychological safety within the maritime industry’s overall safety culture, a concept that views human well-being as central to effective risk management and sustainable operations. 15
Addressing mental health challenges at sea requires not only regulatory alignment but also coordinated, multi-stakeholder action among seafarers, shipowners and maritime companies, and psychological support service providers, who differ in their understanding of mental health needs, resource availability, and corporate priorities.16,17 Interventions and services must be contextually and culturally suitable to foster psychological safety, 18 yet existing initiatives remain fragmented and unevenly implemented across organizations. Despite growing recognition of seafarers’ mental health, prior studies typically examined either individual stressors, specific intervention types, or single stakeholder perspectives, leaving limited evidence on how the needs of seafarers, the services offered by providers, and the practices of employers align (or fail to align) across the system. 11
This study introduces a novel application of the triple Helix model to seafarers’ psychological safety, positioning seafarers (workforce), employers (industry), and psychological service providers (knowledge/practice) as three interdependent institutional actors whose interactions shape the design and effectiveness of mental health support. Using this framework “now” is timely, as post-pandemic regulatory debates and rapid growth in digital mental health solutions create both new opportunities and new coordination challenges for maritime welfare. Unlike prior research that has largely focused on either individual risk factors, for example, stigma, limited resources on vessels,
19
threat to anonymity,
20
and restricted access to digital care
21
or single interventions, this study combines cross-stakeholder survey data with weighted ratio indicators to analyze supply-demand mismatches in metal health services. Understanding these perspectives will help to reveal where collaboration breaks down and where policy and practice can be targeted to close the psychological safety gap at sea. Following research questions were presented to achieve the study’s aim: • What are the key mental health challenges experienced by seafarers on board vessels? • How do seafarers, employers, and service providers differ in their perceptions of psychological safety and mental health interventions? • How well does the supply of mental health interventions meet the demand among seafarers in the maritime industry?
The following sections of the paper outline the psychological demands of maritime work, explain existing interventions to support seafarers’ mental health, describe the research methodology, and present and discuss the empirical findings. The key contributions are synthesized in the conclusions section.
Psychological Demands of Maritime Work
The seafaring profession has a long-standing history of unique psychological demands and a work environment characterized by distinct and compounding stressors.22,23 Early occupational studies from the 2000s already documented difficult working conditions, long hours, and constrained living spaces on board the ships highlighting how such environments undermine seafarers’ well-being and social life. Subsequent research deepened this picture by linking work-rest imbalances, night work, and high job pressure to chronic fatigue 24 and impaired sleep quality. 25 Fatigue was positioned as a central pathway through which workload and physical stressors affect mental health and well-being of seafarers.22,23,26 Mixed-methods and review studies have since confirmed that noise, vibration, enclosed spaces, and high work demands interact to create sustained psychological strain and poorer sleep among seafarers.25-27 Additionally, research demonstrated that seasickness, as additional physical and psychological factor, was linked to poorer cognitive function, increased agitation and irritability 24 compromising sleep quality, 25 and broader mental health impacts including anxiety and depression. 11
Isolation and loneliness have been identified as equally persistent stressors, stemming from prolonged periods at sea, separation from family, and limitations on shore leave and communication.9,26 Pre-pandemic research emphasized that such social isolation combined with multicultural crews and language barriers, can generate interpersonal tensions, discrimination, and conflicts on board further complicating the psychosocial climate. 26 The pandemic-era studies have documented how coronavirus-related crew-change crises and border restrictions dramatically intensified these long-recognized stressors, reporting heightened levels of depression and anxiety among seafarers,9,27 impact of intensified workplace discrimination and interpersonal conflicts, further complicating the social environment onboard.28,29 Most recent post-pandemic analyses suggest elevated depression, anxiety, and fatigue have not simply reverted to pre-COVID levels, indicating that the crisis has had a lasting effect on mental health burden at sea.11,27
Beyond individual distress, the literature consistently demonstrates that psychological demands have direct safety implications. 30 Studies on fatigue and psychosocial risk factors show that poor mental health impairs attention, decision-making, and situational awareness, increasing the risk of accidents, operational errors, compromising ship’s safety performance. 31 Consequently, these strands of the research conceptualize mental health not only as a welfare concern but a core element of maritime safety, thereby providing the conceptual foundation for examining how interventions and stakeholder arrangements might mitigate these demands, additionally influencing career decisions and retention rates of seafarers. 11
Existing Mental Health Interventions and Stakeholders
Building on this evidence of cumulative psychological demands, the literature has examined a growing range of interventions designed to protect seafarers’ mental health.32-38 Traditional approaches include face-to-face stress management training, 33 resilience-building programs, on board psychological initiatives, and shore-based counseling, often grounded in stress-coping theory, positive psychology, and occupational health models,34-36 On-board psychosocial programs and problem-oriented training have reported improvements in perceived stress, resilience, and job satisfaction, however their reach and consistency depend heavily on company priorities, resources, 16 and regions. 10
In parallel, the literature has increasingly highlighted the role of organizational and regulatory actors in shaping the context for these interventions.10-13,15 Studies on safety culture and employment practices argue that crewing standards, work-rest arrangements, and management attitudes toward welfare strongly condition whether psychological support is prioritized, and they call for mental health to be integrated into core safety management rather than an optional add-on.10,11,15 However, analyses of STCW and MLC point to a continued lack of explicit provisions on psychological safety and mandatory mental health training, and qualitative work suggests that commercial pressures and cost-minimization strategies often limit employer investment in comprehensive mental health support.12-14,16,17
Over roughly the past decade, technological developments have introduced a second major strand of interventions: digital and telemedical solutions.21,37-41 Systematic reviews of maritime telemedicine describe the expansion of remote medical assistance and teleconsultation, while survey-based studies show that the vast majority of seafarers (98,4%) now carry smartphones or tablets, and substantial proportion of them download health-related applications (52.5 %), creating new opportunities for app-based prevention and monitoring. 21 Evidence from broader digital mental health research indicates that technology-mediated psychological services can achieve clinically significant reductions in depression and anxiety,37,38 and marine-specific studies report teleconsultation, email and telephone communication already accounts for a large share of shipboard medical assistance. 39 At the same time, empirical work emphasizes persistent barriers, including limited and unreliable connectivity at sea, low digital literacy among some crews, concerns about piracy, cultural stigma, and skepticism regarding the effectiveness of remote interventions. 40 Additional maritime-specific obstacles, such as extended offline periods and limited recreational time lead to high discontinuation rates of apps use, 21 which together constrain the sustained uptake of digital tools. 41
Appendix A provides a systematic comparison of traditional face-to-face versus innovative digital mental health services and interventions for seafarers across multiple dimensions including delivery methods, theoretical foundations, effectiveness evidence, implementation challenges, and stakeholder perspectives. Traditional approaches, encompassing stress management training, 32 resilience programs,34,35 and on-board psychosocial support, demonstrate high contextual fit and participant satisfaction, with evidence of stress moderation effects.34,36 In contrast, innovative digital interventions leverage widespread device ownership among seafarers (98.4% carry smartphones/tablets, with 52.5% having downloaded health apps) 21 to provide 24/7 accessible telemedicine, e-counseling, and mobile health applications. While digital interventions show significant effectiveness in reducing depression and anxiety 39 and comprise 58.6% of maritime medical assistance cases, they face substantial barriers including high discontinuation rates (>50%), connectivity challenges during extended offshore periods, and digital literacy gaps.21,41 The comparison reveals that both approaches offer complementary strengths. Traditional methods excel in personal interaction and cultural adaptation, while digital solutions provide scalability and continuous access, suggesting that hybrid models integrating both modalities may optimize mental health support for maritime populations. Implementation success for both approaches remains uneven across companies and regions, 10 influenced by management priorities and budget allocations, 16 highlighting the need for comprehensive, multi-stakeholder frameworks to enhance seafarer psychological safety.
The literature also points to notable differences in how various stakeholder groups perceive both mental health needs and appropriate interventions.10,16,37,42-45 Psychological support service providers and welfare organizations tend to stress comprehensive strategies that combine monitoring, education, crisis response, and structural improvements (e.g., increased crew numbers and more reliable connectivity). Whereas, employer-focused studies often reveal tensions between commercial imperatives and welfare investments and suggest that shipowners may underestimate the extent of seafarers’ psychological strain.42-44 Moreover, inconsistencies have been noticed in accessing services, the cultural sensitivity of interventions, and uniformity in policy implementation. 10
Overall, while existing services and interventions reveal valuable insights and promising practices, the research portrays a fragmented intervention landscape in which traditional face-to-face programs, emerging digital solutions, and organizational and regulatory measures each address parts of the problem, but are rarely coordinated across stakeholders.9-11,21,32-45 This conceptual background highlights the need for integrative, multi-stakeholder frameworks capable of aligning seafarers’ needs, employers’ provisions, and service providers’ offerings over time. This study addresses identified gap in the subsequent result and discussion sections. The following section presents the methodological approach of the research.
Methodology
This study employed a questionnaire survey to explore stakeholder perspectives on psychological safety interventions for seafarers. The methodology is based on the Triple Helix model, which provides a framework for understanding collaboration among key institutional actors, in this case: seafarers (workforce), shipowners/employers (industry), and psychological service providers (knowledge/practitioners). This design allowed researchers to examine the gaps in the perceptions of the three stakeholder groups regarding the understanding and implementation of mental health support interventions and services.
The questionnaire was tailored to each of three stakeholder groups: 1) seafarers, to capture their personal use and awareness of mental health interventions; 2) employers (shipowners, crewing companies), to assess corporate practices related to mental health and psychological support; and 3) psychological and mental health service providers, to document intervention availability, usage patterns, and perceptions of service needs. The questionnaire was administered in English and was not translated into other languages.
The survey was administered online via Google Forms, which enabled global outreach and asynchronous participation. After the questionnaire was developed in Google Forms, the draft version was pilot-tested with three stakeholders (a seafarer, a shipping company employee, and a support service provider representative) to assess clarity, relevance, and comprehensiveness. Feedback was incorporated into a revised version. The questionnaire was not based on a previously validated instrument; therefore, it should be considered an author-developed tool. No formal psychometric validation (e.g., reliability or factor analysis) was conducted due to the exploratory nature of the study. The survey design included both closed-ended questions (to enable quantitative analysis) and open-ended prompts (to gather narrative insights). This approach supports triangulation by linking frequency-based findings with qualitative patterns and provides a nuanced understanding of mental health promotion in maritime settings. The Triple Helix framework46,47 informed both the sampling and analysis by emphasizing cross-sector dialogue and systemic coordination among the three groups. 48 Involving these distinct perspectives in both data collection and analysis is intended to foster a holistic understanding of psychological safety at sea, 49 consistent with the Triple Helix ethos of cross-sector synergy in addressing complex challenges. 50 This framing was useful given the distributed and multicultural nature of the maritime industry, because it strengthens the validity and practical relevance of the results, in line with calls for coordinated action on seafarer well-being.
A total of 106 respondents represented seafarers (N=48, 45%), service providers (N=14, 13%), and employers (N=44, 42%). Given the exploratory nature of the study and the specialized target groups, a combination of convenience sampling and purposive sampling was used. Participants were recruited through maritime university networks, professional organizations, and maritime training institutions, with outreach facilitated by the World Maritime University students and alumni. Purposive sampling was used to ensure that respondents had experience in at least one of the following three domains: working at sea, managing crews, or providing psychological support to seafarers. Convenience sampling was used to quickly reach participants within established networks and digital platforms. This pragmatic approach ensured the inclusion of relevant experts who have direct experience but limit broad statistical generalizability, as the sample is not representative of the global population, particularly for service providers. The service providers subsample consisted of specialized organizations with niche expertise. Consequently, analyses for this group are primarily descriptive, as frequencies and weighted indicators were used to illustrate tendencies but refrain from drawing firm statistical inferences or over-interpreting non-significant group differences.
The sample was diverse, in terms of nationality and professional background, however heavily skewed toward Asian seafarers (77% predominantly from Bangladesh) with 10% from Africa, and 13% from Europe. This skew reflects the recruitment channels used in this study and the global composition of many contemporary crews. As a result, the findings were interpreted as most representative of Asian-majority trading patterns and employment context, and cannot be generalized to all seafaring populations, particularly those dominated by European crews. Given this regional sew, the survey was sued to explore patterns in perceived mental health challenges and support rather than to generate globally generalizable prevalence rates. Median age was 37 years, and the participants had substantial professional experience of 13 years (seafarers), 15 years (employers), and 20 years (service providers), which enhanced the credibility and maturity of their responses. The majority of seafarers were officers (96%), currently employed or having worked onboard within the past two years.
This study adhered to established ethical standards and was reviewed and approved by the World Maritime University Research Ethics Committee under the protocol number REC-25-50(M), dated June 30, 2025. Prior to commencing the survey, all potential respondents were provided with an informed consent form embedded in the digital survey introduction, explaining their rights, voluntary nature of participation, aims of the research, and data-handling procedures. Respondents were assured of anonymity and confidentiality; no personally identifiable information was collected in the mandatory parts of the survey, and any optionally provided contact details (e.g., email for follow-up) were kept separate and not linked to responses. In summary, the sampling strategy balanced practicality and purposive inclusion of relevant experts, and all steps were taken to ensure ethical treatment of participants. The study was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines. 51 The completed checklist is provided as supplementary file.
Summary of the Questionnaire Sections
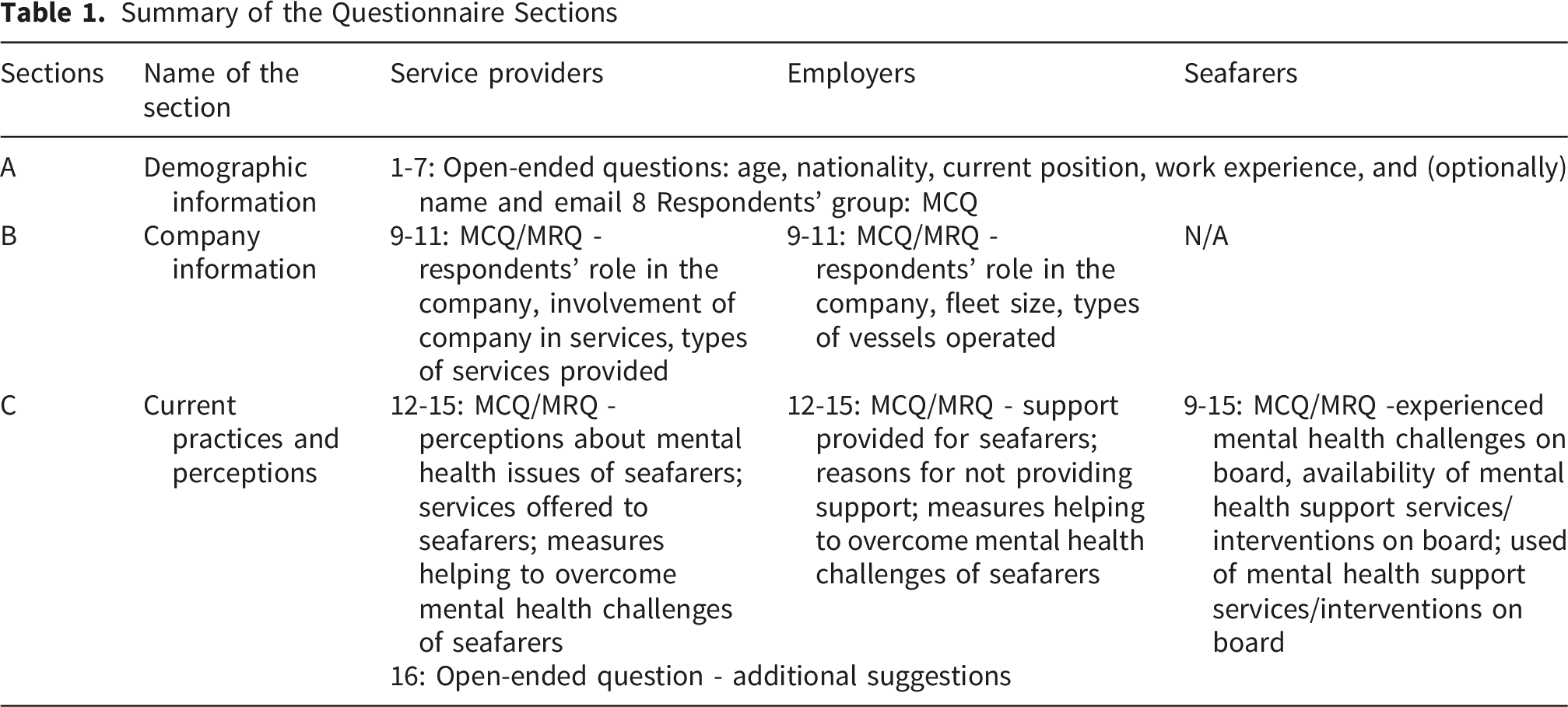
Data Analysis
The data analysis was primarily descriptive and exploratory, as the study aimed to map perceptions and identify key themes rather than test a priori hypotheses. This study employed both quantitative and qualitative analytical techniques to examine survey responses. Quantitative data from closed-ended questions were exported to Microsoft Excel and analyzed using simple descriptive statistics (frequencies, percentages, and cross-tabulations). Weighting coefficients were calculated to adjust the group size imbalance (e.g., N=14 for providers vs. N=48 for seafarers; N=44 for employers) by incorporating the number of organizations or individuals represented (see Appendix C).
Qualitative data obtained from open-ended responses on mental health interventions were systematically analyzed manually using classical content analysis procedures 52 with a focus on thematic coding. All written responses were first transcribed and read, significant words and phrases were highlighted, and codes representing key ideas or themes were assigned. 53 The keyword frequency analysis to support the coding process extracted recurrent terms such as “company support,” “training,” and “counseling”, which emerged consistently across responses. The coded data were grouped into the following thematic categories: Organizational Support, Health Services, Education & Awareness, and Leadership & Culture (Appendix B). Thematic frequency was counted, and illustrative quotes were selected to contextualize the patterns. To ensure coding reliability, approximately 30% of the total qualitative responses were independently coded by two researchers. The initial agreement rate was approximately 87%, and any differences in coding were resolved through discussion and full consensus. A formal IRR coefficient (e.g., Cohen’s kappa) was not calculated, as the qualitative analysis followed a consensus coding approach. Given the relatively small number of open-ended responses and the interpretive nature of the analysis, the aim was to identify and refine thematic categories collaboratively, rather than to produce independently replicable codes. Such consensus-based methods are well-recognized as valid in qualitative research.
Results
Seafarers’ Mental Health Challenges
An analysis of seafarers’ responses revealed that 77% of participants experienced at least one form of mental health challenge onboard. The most frequently reported issues were sleeping disorders (N=30, 63%), anxiety (N=28, 58%), isolation and loneliness (N=54, 54%) and depression (N=25, 52%). Other reported challenges included physical symptoms of stress (N=23, 48%), burnout (N=15, 31%), feelings of hopelessness (N=12, 25%), and suicidal thoughts or behavior (N=3, 6%), with the latter indicating a critical need for targeted support.
Taken together, this high prevalence underscores the pressing need for robust onboard psychological support, particularly interventions targeting sleep hygiene, emotional regulation, and social isolation. These findings are consistent with seafarers open-ended responses, which stressed that “the issue of mental health in the maritime sector is significant and should be addressed in greater depth by the IMO…..It is extremely important to begin to place greater emphasis on seafarers' working conditions, providing conditions that reduce the risk of developing mental health problems”; called for “training where how to handle stress should be taught to management & operation”; and highlighted that “e-counseling would be one of the necessary tools to provide assistance to seafarers, providing accessibility and flexibility to these support channels for those on board.”
Support Availability and Utilization
Despite widespread experience with mental health issues, access to services remains critically limited. Only 29% (14 out of 48) reported that psychological support services were available on board, and just 6% of the full sample (three respondents) reported having actually these services. Fewer than half of respondents (23 of the 48) indicated that they had participated in the training. Notably, among those who had not participated in training (25 individuals), a significantly higher proportion reported a lack of support in this area or were unsure, with three individuals responding “not sure”. Statistical analysis revealed a moderate to strong positive correlation between training participation and perceived availability of support services (Pearson’s r = 0.566, N = 48). The correlation was statistically significant (t (46) = 4.66, t = 2.013, p < 0.001), indicating that respondents who had received training were significantly more likely to report the availability of mental health support onboard.
At the company level, interestingly, 23 of the 44 respondents stated that such services were available within their organization, covering 21 different companies varying in fleet size. This suggests that approximately half the companies do not provide psychological services. Nonetheless, consultancy and training have consistently emerged as dominant approaches for addressing mental health challenges.
These findings point to both accessibility barriers and underutilization of services, which may stem from factors such as stigma (e.g., a seafarer stated, “admitting stress feels like weakness”), perceived inadequacies in service quality, and limited awareness. Furthermore, the results highlight the need to enhance effectiveness of training initiatives, one respondent suggested that “several counseling sessions with a professional therapist” would be more beneficial. An initial review of employer practices revealed that consultancy services are more commonly implemented than formalized training programs, a trend echoed in employer responses.
Intervention Categories and Their Frequencies
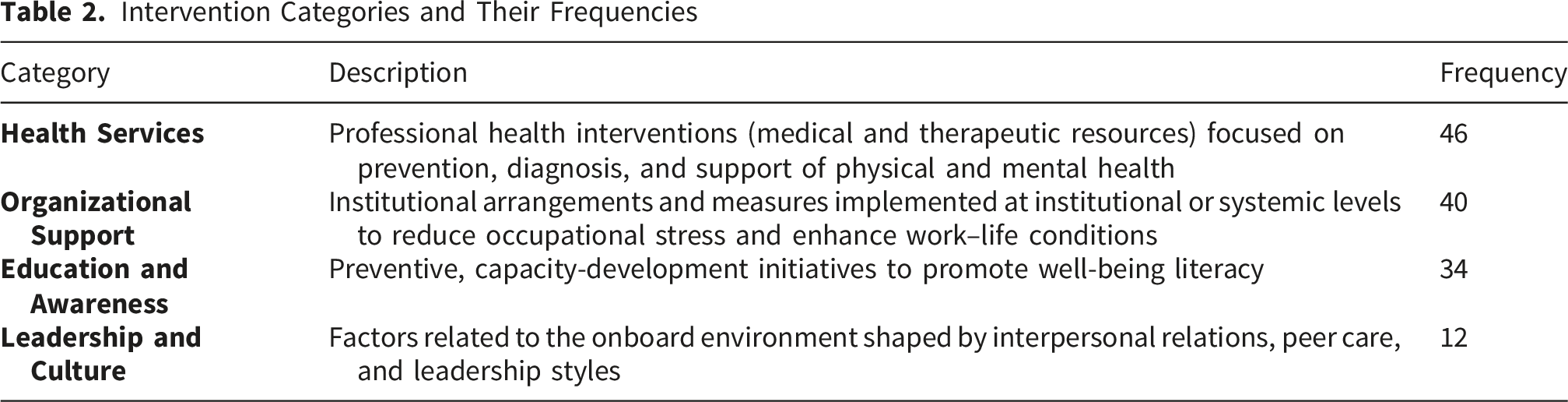
These findings suggest that seafarers are more aware of and utilize both health and medical services and system-level improvements such as better leadership practices and fairer work arrangements to a larger extent.
Stakeholder Comparison: Perceptions, Priorities, and Barriers
This section presents a comparative analysis of three stakeholder groups
From the perspective of service providers, the distribution of their opinions regarding mental health challenges of seafarers differs from seafarers’ own responses. The most frequently cited challenge was isolation/loneliness (N=11, 79%); whereas seafarers themselves most often reported sleep disorders. Service providers also highlighted sleeping disorders (N=10, 71%), depression (N=9, 64%); physical symptoms of stress (N=7, 50%) as prevalent concerns. Anxiety and burnout (N=4, 29%), were reported less frequently, followed by feelings of hopelessness and suicidal thoughts or behavior (N=3, 21%). Although less commonly cited, the latter represents a critical area requiring targeted support.
The analysis of the results revealed different perceptions of service providers and seafarers regarding their understanding of the mental health challenges on board (Figure 1). This discrepancy suggests a possible underappreciation of emotional distress among stakeholders. Although the differences in reported mental health challenges between seafarers and service providers shown in Figure 1 appear visually notable, statistical analysis (Fisher’s Exact Test and Chi-square tests) indicated that these differences are not statistically significant (p > 0.05). This outcome is likely influenced by the small sample size of service providers (N=14), which limits the statistical power of the comparison. Seafarers’ and service providers’ perspectives on mental health challenges on board (X-axis: Challenge Type, Y-axis: Frequency)
The finding suggest that employers and service providers demonstrate different perceptions regarding the utilization of available psychological support services for seafarers. Out of 44 companies, 24 (55 %) reported providing mental health support to the seafarers. The most frequently mentioned types of support were medical treatment (N=19, 43%), welfare support (financial/legal/social) and mental health awareness/training programs (N=16, 36%), Crisis Intervention (e.g. suicide prevention) (N=13, 30%), Mental health counseling (In person) (N=11, 25%), Mental health counseling (online/e-counseling) (N=10, 23%), Hotline (N=6, 14%), Chaplain or spiritual guide (N=3, 7%). Notably, video training was not mentioned at all. In comparison, service providers strongly placed strong emphasis on mental health awareness/training programs (N=11, 79%), crisis interventions (N=10, 71%), hotlines (N=9, 64%), welfare support (financial/legal/social) (N=8, 57%), mental health counseling (in person) (N=6, 43%), mental health counseling (online/e-counseling) (N=5, 36%). The other measures, such as projects, campaigns, advocacy, grants and sector specific guidance were mentioned only once. This reflects an adaptive response to the remote and dispersed working conditions of the seafarers. However, systemic and contextualized interventions, such as sector-specific guidance, projects, and campaigns (e.g., IMO’s 2025 Mental Health initiatives), remain less common, despite the high relevance of the holistic approach and development of the “culture of care” in the maritime industry.
The opinions of employers and service providers regarding measures to overcome seafarers’ mental health challenges also differ (Figure 2). Notably, the measures required by employers might not be adequately offered by service providers, with the biggest gap observed in providing counseling and training programs. Comparison of service providers’ and employers’ views on measures to overcome mental health challenges (X-axis: Measure type, Y-axis: Frequency)
When asked about the reasons for not providing mental health support (open-ended question), the employers mentioned absence of requirements (N=14, 32%); resources constraints (N=9, 20%); cultural resistance (N=7, 16%); not considering mental health a core maritime skill (N=7, 16%); or other factors, e.g., “limited internet access,” “lack of privacy,” and “logistical challenges make it difficult for seafarers to access mental health support while at sea,” “our crew go on ships for specific jobs.”
Comparative Summary Table Contrasting Stakeholder Perspectives

Demand vs. Supply: A Structural Gap
This part of the analysis examined how well three items align: 1) seafarers’ demand for mental health services/interventions, 2) service providers’ potential supply, and 3) employers’ actual provision (see Appendix C for formulas). Because the three stakeholder groups differ in sample size, direct comparison of raw frequences (and percentages) would disproportionally reflect the larger groups and amplify random variation in the smallest group. Weighted ratio indicator framework based on ratio indicators, weighting coefficient, and structural indicators is described in Appendix C. Because the three stakeholder groups were unequally represented (seafarers N=48, service providers N=14; employers N=44), simple proportions could bias the analysis toward the largest group.
Calculation of Ratio Indicators, Weighting Coefficients, and Structural Indicators
Ratio Indicators and Structural Indicators to Assess Mental Health Support Demand and Supply

Summary of Weighting Coefficients

Since seafarers primarily need and use services, in this study, their responses represent demand, whereas service providers and employers primarily offer and implement services so their responses represent supply (potential and realized, respectively). As shown in Table 5, potential demand exceeds realized supply. This suggests that although mental health service providers offer a wide range of interventions, employers do not fully utilize them to support seafarers.
Third, ratio indicators for each intervention were converted into structural indicators (demand D i and supply S i ) by using weighting coefficient (Appendix C, Formula 4) to obtain comparable structural indicators for the research unit (Table 4, columns 2, 4, 6).
Maximum and Average Demand Indicators, and Structural Gap
To characterize overall demand for mental health support, two aggregate metrics were derived from seafarers’ responses. First, the maximum demand incorporates the share of seafarers who experienced at least one mental health challenge onboard. In this sample, 37 out of 48 seafarers reported at least one challenge, providing a proportion of 0.77=37/48. This proportion was then adjusted using the weighting coefficient for seafarers w ij =0.79 to obtain the maximum demand indicator D max = 0.77 x 0.79=0.61. This value (0.61) estimates the intensity of interventions required if all reported challenges were adequately addressed.
Second, the average demand was calculated to capture the typical level of mental health support/interventions need, D av =0.48 x 0.79=0.33, where 0.48 is the average proportion of seafarers experiencing any mental health challenge, and w ij =0.79 is the weighting coefficient. This metric represents a balanced estimate of overall demand, and can be used to assess the alignment between demand and supply. Together, these two indicators allow the analysis to distinguish between peak (maximum) needs and more routine (average) demand in assessing the demand-supply gap.
The research findings indicate that the maximum demand for mental health support services among seafarers is 0.61; however, the proportion of seafarers who perceive these services as accessible is significantly lower (average demand of 0.33), as shown in Table 4. Most seafarers identified mental health counseling (online/e-counseling, 0.16) and medical treatment (0.12) as the most used services. Service providers claimed that they could deliver certain interventions/services at comparatively higher rates, such as mental health awareness/training programs (0.20), crisis interventions (0.18), hotlines (0.16), and welfare support services (0.15). Although these supply values do not reach even the average demand (0.33), they fall short of the maximum demand (0.61) and are neither fully utilized by seafarers nor adequately provided by employers.
The findings clearly reveal a mismatch between seafarers’ needs, available services, and the extent to which employers utilize them (Table 5, Figure 3). Employers provide various interventions to prevent and address mental health challenges. However, almost all offerings fail to meet either the maximum or the average demand levels identified by seafarers with exception of medical treatment with the highest employers’ supply indicator 0.1, and seafarers reports of using this service to a bigger extent (0.12). Interestingly, some interventions, such as crisis interventions and hotlines are provided but are not considered useful by seafarers (structural indicator 0.02), possibly due to limited access. Conversely, chaplain or spiritual guidance is considered useful by seafarers (0.06) but is neither provided by service providers nor adequately utilized by employers (0.01). Similarly, online or e-counseling is in demand among seafarers (0.16) but is not adequately addressed by other stakeholder groups. These disparities are illustrated in Figure 3. Demand and supply of mental health support services/interventions from perspectives of three groups of stakeholders (X-axis: mental health support services/interventions; Y-axis: structural indicators)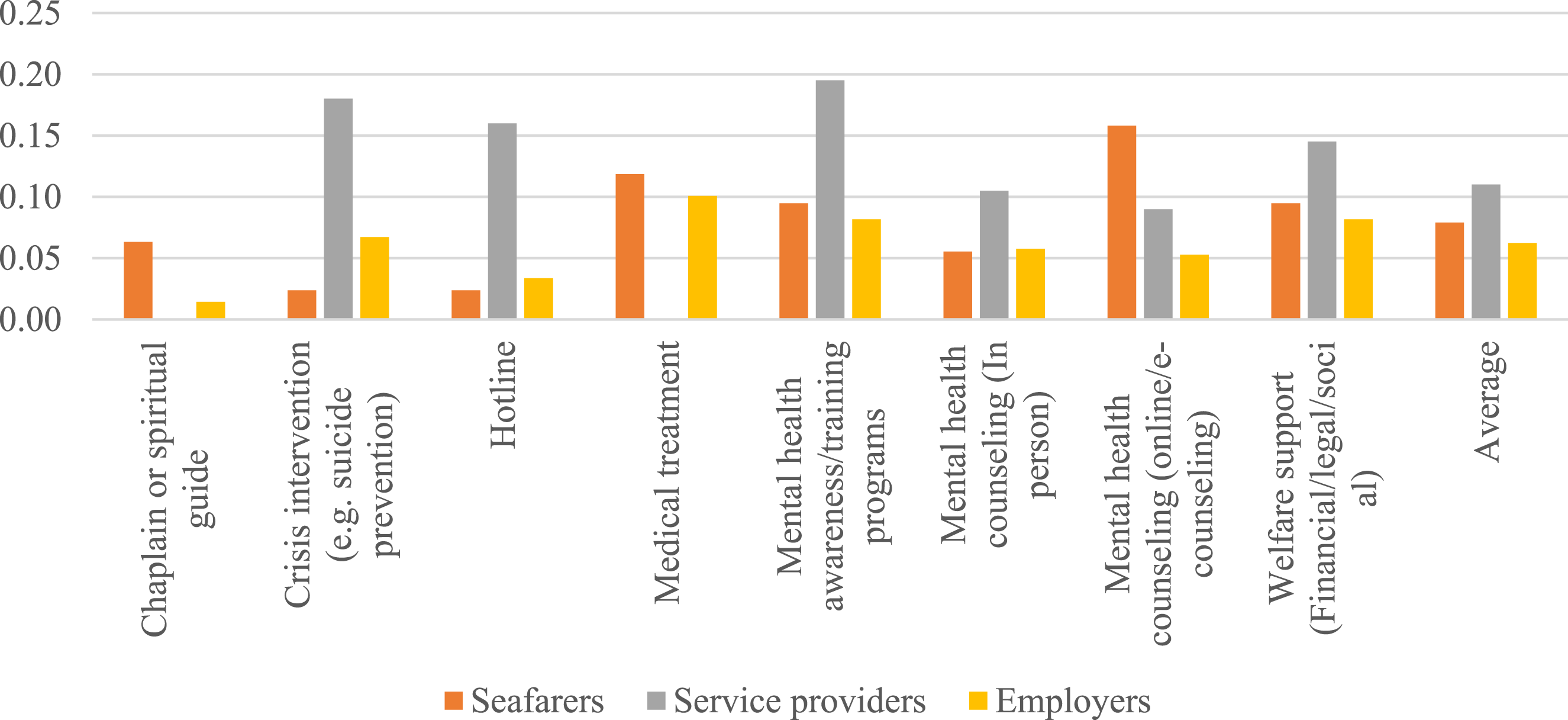
In Figure 3, the orange bars represent demand (the proportion of seafarers indicating a need for each service); the grey bars indicate the potential supply from service providers, and the yellow bars reflect the actual supply from employers (legend provided in figure). The largest imbalance was observed in suicide prevention services, with a demand of 0.02 far below the potential supply of 0.18 and employer provision of 0.07.
Two indices were calculated to assess the relationship between the supply and demand (see Appendix C): Supply–Demand Balance Index (2.59) and Utilization of Suggested Services Index (0.58). Based on these indicators, this study confirmed that the potential services offered by mental health providers are underutilized. Employers meet only one-fifth of average demand, with the widest gaps in counseling (0.11) and suicide prevention (0.12). Employers could enhance the provision of necessary support to seafarers by more effectively leveraging this untapped market potential.
As a summary of the findings, Figure 4 illustrates how seafarers (workforce), employers (industry), and service providers (knowledge/practice) interact within a Triple Helix model, showing that seafarers psychological needs and help-seeking are constrained by stigma, employers provide only partial support due to costs, weak regulations and logistics; and service providers hold underused expertise and digital tools. All of this results in misalignment: unmet needs and untapped capacity for mental health support services and interventions for seafarers as well as underutilized available support services by seafarers. Triple Helix model: Misalignment in seafarer mental health support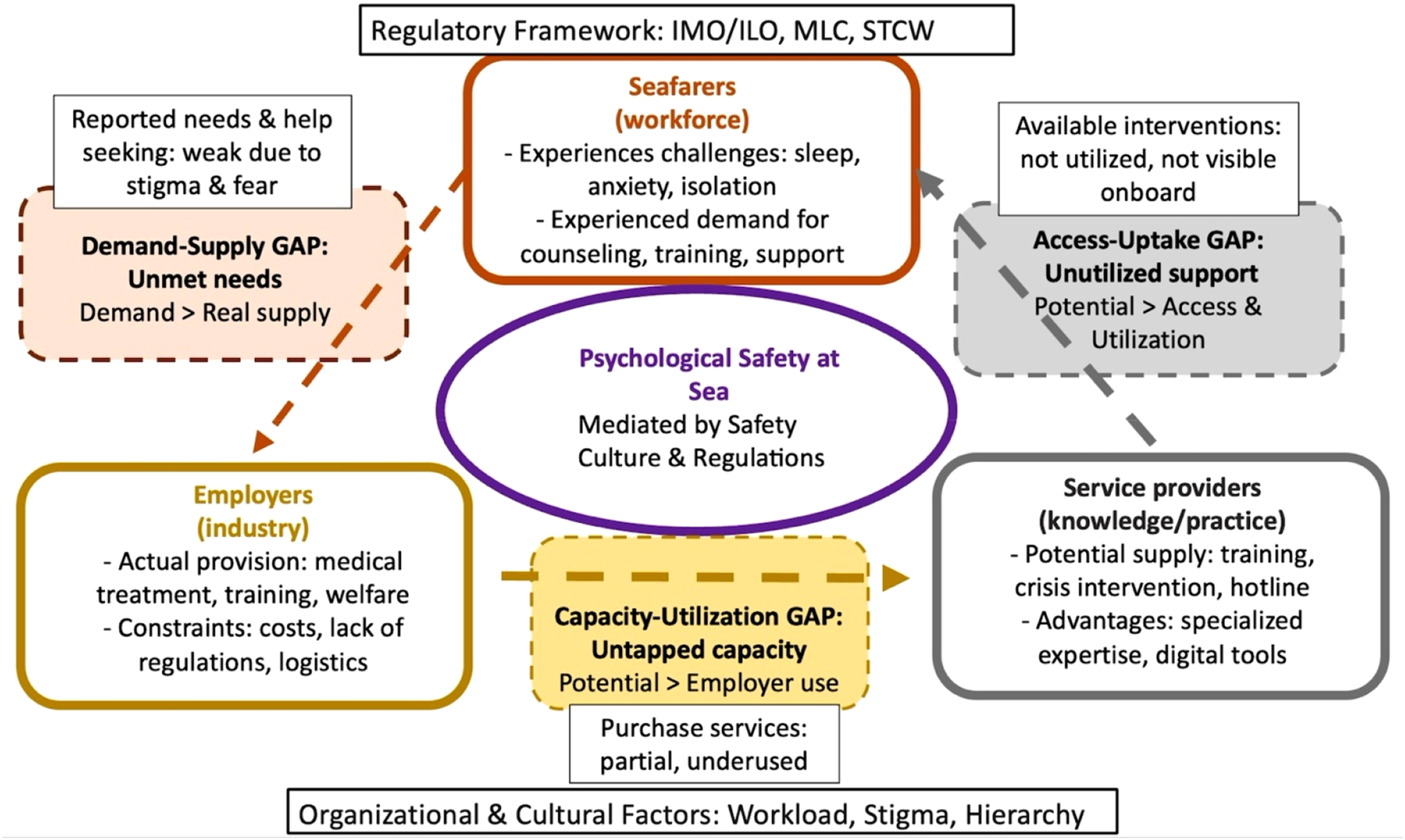
Discussion
This study provides one of the first comprehensive multi-stakeholder analyses of psychological safety and mental health support in the maritime industry, combining seafarers’, employers’, and service providers’ perspectives within a Triple Helix model. By integrating weighted structural indicators with qualitative insights, the study demonstrates how misalignment between industry (employers), knowledge and practice actors (service providers), and the workforce (seafarers) produces systematic gaps between the needs for mental health support interventions, available services, and actual implementation. Rather than focusing on prevalence or single interventions, the analysis highlights three interrelated domains where gaps emerge: regulatory arrangements, organizational and cultural conditions, and stakeholder coordination.
Regulatory Gaps and Ambiguous Spaces
The findings confirm that international maritime regulation still treat psychological safety in a fragmented and implicit manner. There is currently no clear mandatory requirements under the STCW or MLC conventions for mental health of psychological safety training, leaving these issues to interpretation within more general provisions on competence and welfare.12,13 This ambiguity makes it easier for organizations to treat psychological safety as optional rather than a core component of operational risk management, echoing earlier critiques that mental health has not been systematically integrated into maritime safety governance.10,11,18 The division of responsibilities between training-oriented (STCW) and labor-oriented (MLC) instruments further diffuses accountability and makes it difficult for companies to know which standards to follow when designing mental health programs. Our results therefore support calls for clearer regulatory anchoring of psychological safety, including explicit guidance on minimum training content, support structures, and monitoring requirements.11,15
Organizational Barriers and Cultural Constraints
The qualitative findings underscore that seafarers perceive mental health challenges not merely as individual issues but as direct outcomes of organizational conditions, such as excessive workloads, poor management practices, and limited shore leave. As one seafarer noted, “Long hours and no break leave us exhausted”. These accounts are consistent with earlier work that associates long working hours, unsafe crewing levels, and rigid hierarchies with fatigue and psychological strain at sea.16,17,22,23 Seafarers’ requests for more supportive leadership, fairer work–rest arrangements, and normalized access to counseling resonate with Edmondson’s concept of psychological safety as a climate of interpersonal trust and respect that enables people to speak up and seek help without fear of blame. 3 At the same time, cultural taboos and stigma continue to constrain help-seeking in multinational crews, where mental health problems may be viewed as weakness or a threat to employability.10,19,20 Employers’ emphasis on commercial pressures, the absence of explicit regulatory requirements, and limited budgets reinforces these barriers by deprioritizing investment in psychological support.10,16 The result is a mutually reinforcing cycle in which organizational conditions generate distress, stigma discourages disclosure, and companies under-invest in support because needs remain partly invisible.
Stakeholder Misalignment and Implementation Challenges
The structural indicator analysis adds a new dimension to prior research by quantifying how demand and supply diverge across stakeholders. Whereas earlier studies have described under-utilization of welfare services and inconsistent company initiatives,9-11,21,32-41 our weighted indicators show that, after adjusting for unequal sample sizes, potential supply from specialized service providers substantially exceeds the level of support that employers report offering and that seafarers say they can access. Providers report capacity for high-intensity services such as crisis intervention, hotlines, and training, yet employers draw on only a subset of these options, and many seafarers remain unaware of or unable to use them.
This misalignment is also perceptual. Service providers place particular emphasis on isolation, loneliness, and suicidality, while seafarers more frequently mention sleep disturbance and anxiety, and employers highlight generic “training” or “consultancy” without specifying psychological content. These differences mirror findings in other sectors where professionals, managers, and workers prioritize different aspects of mental health risk,39-41 but the Triple Helix lens clarifies the structural consequences: when stakeholders are not aligned on which problems are most salient, they design and commission different types of interventions, leading to partial or misplaced responses.
Our Supply–Demand Balance and Utilization indices suggest that employers currently mobilize only a fraction of the available support and that coordination between employers and service providers is occasional rather than strategic. This extends prior maritime work by moving beyond descriptive lists of services to an explicit measurement of how far demand exceeds real supply and which service categories (for example, counseling and suicide prevention) are most affected.
Safety Culture as a Mediating Factor
Safety culture emerges from the data as a key mediator between structural conditions and individual experiences. In companies where communication is open and reporting is non-punitive, seafarers are more likely to view training and support services as legitimate and to perceive help as available, reinforcing earlier evidence that strong safety cultures foster both psychological and operational safety.7,8,10,11,15 Conversely, where blame, fear of sanctions, or rigid hierarchy dominate, seafarers describe reluctance to admit difficulties and uncertainty about how to access support, even when services formally exist. Integrating mental health explicitly into safety management systems through procedures, briefings, and debriefings could therefore shift support from an ad hoc welfare activity to a routine element of risk control.
Lessons From Other High-Risk Sectors
Comparisons with aviation, offshore oil and gas, and other high-risk industries suggest that the maritime sector is at an earlier stage of institutionalizing psychological safety.4-6 In those sectors, regulatory authorities and companies have progressively embedded mental health within safety cases, crew resource management, and fatigue-risk management systems, supported by structured training and confidential reporting mechanisms. Our findings indicate that similar trajectories are only beginning in shipping: digital counselling, telemedicine, and resilience programs exist but remain unevenly deployed and poorly integrated with company safety processes.9,21,32-39 The mismatch patterns identified here can therefore be seen as a diagnostic snapshot of a sector in transition, with emerging tools but incomplete governance and coordination.
Contribution to Psychological Safety Research
Taken together, the results reinforce the view that mental health support is not a peripheral welfare issue but a central determinant of psychological safety and, by extension, maritime safety performance. In line with Edmondson’s definition, 3 effective support enables seafarers to raise concerns, admit mistakes, and seek help without fear of negative consequences, thereby reducing the risk of error and improving teamwork and communication.7,8,30,31 The distinctive contribution of this study lies in showing, through a Triple Helix and structural-indicator approach, where the chain between distress, service capacity, and organizational implementation breaks down, and how those breakpoints are patterned across stakeholder roles. This provides a foundation for more targeted governance reforms and partnership models aimed at closing the psychological safety gap at sea.
Conclusion
This study shows that psychological distress is widespread among seafarers and that support structures remain fragmented and unevenly implemented across the maritime sector. Weighted indicators and multi-stakeholder data reveal that seafarers’ demand for mental health support substantially exceeds the services that employers currently provide, even though specialized service providers report considerable unused capacity. Interpreted through a Triple Helix lens, these findings point to systemic misalignment between workforce needs, industry practices, and knowledge-provider offerings, rooted in regulatory ambiguity, organizational constraints, and cultural stigma.
To move from fragmented welfare initiatives toward integrated psychological safety systems, the following actions cab be recommended: - embed explicit psychological safety and mental health requirements in international and national maritime regulations (eg, through STCW and MLC revisions), including minimum training content and expectations for company support structures; - integrate mental health into company safety management systems, linking leadership practices, work–rest arrangements, and confidential reporting mechanisms to both safety and welfare performance indicators; - develop structured partnerships between employers and specialized mental health service providers, using digital and face-to-face services in combination and actively monitoring uptake to ensure that available capacity matches seafarers’ expressed needs; - invest in stigma-reducing education and leadership development for officers and shore-based managers, so that seeking support is normalized, and seafarers feel safe to raise concerns without jeopardizing their careers.
Together, these measures can help align demand, potential supply, and actual provision of mental health services, thereby strengthening psychological safety and contributing to more sustainable and resilient maritime operations.
Limitations and Implications for Future Research
This study had several limitations. First, although it engaged diverse respondents across three continents, the sample was skewed toward Asian seafarers (77%), limiting generalizability across other cultural and organizational contexts. The sample size/power analysis was not performed for this study. The predominance of Bangladeshi/Asian respondents may amplify region-specific factors such as employment conditions, cultural norms surrounding help-seeking, and access to welfare infrastructure. These patterns might differ in labor markets where unionization, social security, or employer support regimes are stronger. Future research should replicate this analysis with more geographically balanced samples to assess the transferability of the Triple Helix insights.
Second, the questionnaire was not formally validated using psychometric methods. Although pilot testing supported clarity and relevance, future research should establish reliability and construct validity.
Third, the relatively small number of service providers (N=14) also restricts the conclusions regarding the global intervention market. Very small number of service providers may underrepresent the diversity of commercial and welfare models in the broader market. Future research should enlarge this stakeholder group, for example by targeted sampling of global telemedicine, welfare, and insurance providers, to test their supply-demand mismatches identified.
Moreover, the questionnaire survey design captures only a snapshot in time, without longitudinal evidence of how interventions affect psychological well-being at sea. Future research should include longitudinal studies.
Supplemental Material
Supplemental Material - Bridging the Gap: A Triple Helix Perspective on Interventions to Strengthen Seafarers’ Mental Health
Supplemental Material for Bridging the Gap: A Triple Helix Perspective on Interventions to Strengthen Seafarers’ Mental Health by Inga Bartusevičienė, Farzana Yasmin in The Journal of Health Care Organization, Provision, and Financing
Supplemental Material
Supplemental Material - Bridging the Gap: A Triple Helix Perspective on Interventions to Strengthen Seafarers’ Mental Health
Supplemental Material for Bridging the Gap: A Triple Helix Perspective on Interventions to Strengthen Seafarers’ Mental Health by Inga Bartusevičienė, Farzana Yasmin in The Journal of Health Care Organization, Provision, and Financing
Footnotes
Acknowledgements
We would like to thank the respondents who participated in the study.
Ethical Considerations
This study adhered to established ethical standards and was reviewed and approved by the World Maritime University (WMU) Research Ethics Committee under the protocol number REC-25-50(M), dated June 30, 2026. The email from the research office is provided as a supplementary file.
Consent to Participate
The declaration of consent was included in the online questionnaire: “By completing this survey, you are consenting to participate in the research study.”
Author Contributions
FY contributed to the design and implementation of the research and editing of the manuscript, IB contributed to the design of research, analysis of the results, and to the writing of the manuscript.
Funding
The funders had no role in the study design, data collection and analysis, decision to publish, or manuscript preparation.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and analyzed during the current study are not publicly available because of the nature of the subject under investigation and the willingness of respondents to answer the questions subject to confidentiality being respected. The datasets are available in anonymous formats from the corresponding author upon reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.