
Abstract
Introduction
This study examines how technology-supported services contribute to the reconfiguration of care practices and how these processes shape pathways to outpatient satisfaction in public hospitals. Rather than treating digital technologies as standalone solutions, this study analyzes the pathways linking structural conditions, care processes, and technology-supported services to outpatient satisfaction, with particular attention to differences between urban and rural public hospitals.
Methods
A cross-sectional survey was conducted among 2,084 outpatients attending five public hospitals (two city-level and three rural-level) in East Kalimantan, Indonesia. Patient-reported experiences of care were analyzed using an extended structure–process–outcome framework. In this framework, technology-supported services were incorporated as a process-related component. Partial Least Squares Structural Equation Modeling (PLS-SEM) was used to estimate direct and indirect pathways to general patient satisfaction, with subgroup analyses for urban and rural hospitals.
Results
Care processes, particularly caring attitudes and emotional support, were central determinants of outpatient satisfaction across settings. Structural factors showed both direct and mediated effects, with professional competence more influential in urban hospitals and environment and facilities more salient in rural hospitals. Technology-supported services had a significant direct effect on satisfaction and mediated the relationship between structural capacity and patient experiences, though their relative importance varied by context.
Conclusion
By conceptualizing technology-supported services as embedded care practices rather than standalone tools, this study provides new evidence on the pathways linking care practices to outpatient satisfaction in public hospitals.
Keywords
Introduction
Patient satisfaction is widely recognized as a key indicator of healthcare quality and health system performance. Satisfied patients are more likely to adhere to medical advice, maintain continuity of care, and utilize health services appropriately, ultimately contributing to better health outcomes and system efficiency. 1 However, patient satisfaction is inherently multidimensional and cannot be adequately understood through a single global measure. Consequently, increasing attention has been directed toward Patient-Reported Experience Measures (PREMs), which capture patients’ concrete experiences across various aspects of healthcare delivery and provide actionable insights for quality improvement.2,3
In Indonesia, improving the quality and equity of healthcare services remains a central policy objective, particularly following the implementation of the National Health Insurance scheme. 4 The implementation of the National Health Insurance (JKN) program has substantially expanded population coverage and increased healthcare utilization in Indonesia. However, this expansion has also intensified pressure on public hospitals, leading to overcrowding, prolonged waiting times, and variations in service quality. These challenges are further compounded by significant urban–rural disparities and geographic barriers in the archipelagic health system, which influence patients’ access to hospital care and their experiences during service delivery.5,6
One of the most critical structural challenges in the Indonesian health system is the unequal distribution of health human resources. 6 Health professionals particularly specialist physicians, experienced nurses, and allied health personnel, are disproportionately concentrated in urban and economically developed areas, while rural and remote regions continue to experience chronic shortages. 7 Urban hospitals benefit from higher staff-to-population ratios, better opportunities for professional development, and greater exposure to advanced medical technologies. 8 In contrast, healthcare facilities in rural areas often operate with limited numbers of health workers, higher workloads, and restricted access to training and specialization. 9 These disparities directly influence not only service availability but also patients’ perceptions of professional competence, responsiveness, and continuity of care.
Beyond human resource imbalances, Indonesia’s unique geographical characteristics pose additional challenges to equitable healthcare delivery. As the world’s largest archipelagic country, Indonesia consists of thousands of islands with highly diverse topography, ranging from densely populated metropolitan areas to remote, mountainous, and island communities. 10 Geographic fragmentation complicates transportation, referral systems, and supply chains for medical equipment and pharmaceuticals.9,10
Public hospitals play a dominant role in healthcare delivery in Indonesia, serving as primary providers for both outpatient and inpatient care. Similar to patterns observed in other low- and middle-income countries, many patients bypass primary healthcare facilities and directly seek care at secondary or tertiary hospitals, regardless of disease severity. 11 This tendency further concentrates service demand in urban hospitals and exacerbates workload pressures on health professionals, while rural hospitals continue to struggle with limited resources and lower service capacity. Understanding patient experiences within hospital settings is therefore essential for identifying priority areas for improvement and informing resource allocation decisions. 12
To conceptualize healthcare quality, this study draws on Donabedian’s structure process outcome framework, which has been extensively applied in health services research. Within this framework, structure refers to organizational and physical attributes of healthcare settings, including facilities and the availability and competence of health human resources; process encompasses interactions and activities involved in care delivery, such as communication, caring attitudes, efficiency, and cost-related experiences; and outcome reflects the results of care, commonly operationalized as patient satisfaction in outpatient settings. 13 Previous research suggests that while structural factors establish the conditions for care, patients’ experiences of care processes are often the most proximate determinants of satisfaction. 14
In recent years, healthcare technology has emerged as an increasingly important component of care processes in Indonesia, particularly in urban hospitals. The introduction of electronic registration systems, digital queue management, electronic medical records, hospital information systems, and technology-assisted communication has the potential to mitigate some structural and geographic constraints by improving efficiency, information flow, and service coordination.5,6,15 However, access to and effective utilization of such technologies remain uneven across regions, mirroring broader disparities in infrastructure and human resource capacity.
Although previous studies have examined patient satisfaction and healthcare quality using the structure–process–outcome framework, most studies have primarily focused on interpersonal care, service efficiency, or facility characteristics.16,17 The role of technology supported services, such as electronic registration systems, digital queue management, and hospital information systems, in shaping patient experiences and satisfaction has received comparatively limited empirical attention. Moreover, existing studies rarely examine how these digital-enabled service processes interact with structural conditions and care practices to influence patient satisfaction across different healthcare contexts. In particular, evidence remains limited regarding how technology-supported services contribute to patient satisfaction in public hospitals characterized by urban–rural disparities and unequal resource distribution.
Therefore, this study aims to examine the pathways linking healthcare structure and process factors including technology-supported services to outpatient satisfaction in Indonesian public hospitals, using a conceptual framework adapted from Donabedian’s model. Specifically, this study seeks to assess patients’ experiences of key structural and process-related aspects of hospital care and analyze the direct and indirect effects of these experiences, including the role of technology, on overall patient satisfaction. By incorporating human resource distribution and geographic context into a patient-centered analytical framework, this study is expected to provide policy-relevant evidence to support ongoing efforts to improve healthcare quality and equity in Indonesia.
Theoretical Foundation and Hypotheses
This study is grounded in Donabedian’s structure process outcome framework As depicted in Figure 1, which conceptualizes healthcare quality as a sequence in which structural conditions influence care processes, ultimately shaping patient outcomes. This framework has been widely applied in patient experience and satisfaction research and provides a robust theoretical foundation for examining complex service delivery pathways in hospital settings.13,16 Patient satisfaction is treated as an outcome that is jointly determined by both structural attributes of healthcare facilities and patients’ experiences of care processes.
18
Conceptual model Donabedian’s structure process outcome
In this framework, structure represents the foundational characteristics of healthcare organizations that enable or constrain service delivery. Structural components include the moral orientation of medical staff, the physical environment and availability of facilities, and the professional competence of healthcare providers. 18 These elements reflect the institutional and human resource capacity of hospitals and are particularly relevant in contexts marked by urban–rural disparities and unequal distribution of health resources. Structural factors are theorized to have both direct effects on patient satisfaction and indirect effects through care processes, consistent with Donabedian’s original propositions. 16
The process domain captures patients’ direct experiences during healthcare encounters and constitutes the central mediating mechanism in the framework. In line with previous study, key process dimensions include communication and information provision, caring attitudes and emotional support, perceived medical costs, and efficiency and coordination of care. 19 These dimensions represent the interpersonal, informational, and organizational aspects of service delivery that patients encounter during outpatient visits. Prior evidence suggests that process-related experiences are often the most proximal determinants of patient satisfaction, as they directly shape perceptions of responsiveness, respect, and service quality. 20
Building upon the original framework, this study extends the process domain by incorporating technology-supported services as an integral component of contemporary healthcare delivery. Technology-supported services refer to the use of digital and information technologies such as electronic registration systems, digital queue management, electronic medical records, and technology-assisted communication to support clinical and administrative processes.21,22 The inclusion of this variable reflects the growing role of health information technology in shaping patient experiences, particularly in improving efficiency, information flow, and service coordination. Technology is conceptualized not as a structural resource, but as a process enabler that mediates how structural capacities are translated into patient-perceived service quality.
The outcome domain is represented by general patient satisfaction, which reflects patients’ overall evaluation of the healthcare services received during outpatient visits. Satisfaction is treated as a global outcome that integrates patients’ assessments of multiple care dimensions rather than a single isolated attribute. 17 The framework posits that patient satisfaction is influenced directly by both structural conditions and process experiences, while also being indirectly shaped by structural factors through their effects on care processes.
Overall, this conceptual framework hypothesizes that structural attributes of hospitals shape the quality of care processes, including technology-supported services, which in turn influence general patient satisfaction. By explicitly modeling these pathways, the framework allows for the examination of both direct and mediated effects, offering a nuanced understanding of how healthcare quality is experienced by patients across different hospital contexts. This approach is particularly suitable for analyzing urban–rural differences and identifying priority areas for policy and managerial interventions in health systems characterized by geographic and resource heterogeneity.
Research Hypotheses
To address this gap, the present study examines how structural conditions and care practices particularly technology-supported services are associated with outpatients’ general satisfaction in public hospitals. Focusing on differences between urban and rural settings in Indonesia, the study is guided by the following research questions and hypotheses.
Hypotheses
H1: Environment and facilities are positively related to general patient satisfaction. H2: Professional competence is positivelty related to general patient satisfaction. H3: The care process dimension, including (a) caring attitudes and emotional support, (b) communication and information, (c) medical costs, (d) efficiency and waiting time, and (e) technology-supported services are positively related to general satisfaction. H4: Environment and facilities are indirectly related to general patient satisfaction through care process variables, including (a) caring attitudes and emotional support, (b) communication and information, (c) medical costs, (d) efficiency and waiting time, and (e) technology-supported services H5: Professional competence is indirectly related to general patient satisfaction through care process variables, including (a) caring attitudes and emotional support, (b) communication and information, (c) medical costs, (d) efficiency and waiting time, and (e) technology-supported services
Methods
Setting
This cross-sectional study was conducted between August and December 2025 in five public hospitals located in East Kalimantan, Indonesia. The selected hospitals represented both rural and urban healthcare settings, reflecting variations in healthcare infrastructure, availability of health human resources, access to technology, and geographic conditions within the province.
The five hospitals included in the study, three hospitals are located in rural areas and two are located in urban areas. Rural hospitals primarily served populations residing in geographically dispersed and less accessible regions, while urban hospitals were situated in more densely populated areas with relatively better-developed health systems and technological infrastructure. This distribution was intended to capture contextual differences in healthcare delivery and patient experiences between rural and urban settings.
Public hospitals were chosen due to their central role in providing outpatient services under the National Health Insurance scheme. The selected study period allowed for sufficient patient volume to be captured across different hospital settings while ensuring consistency in data collection procedures.
This study was reported in accordance with the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) guidelines for cross-sectional studies, and a completed checklist is provided as supplemental material. 23
Participants
It was planned to recruit a convenience sample of approximately 610 outpatients per hospital through face-to-face interviews using a structured questionnaire developed by the research team. Eligible participants were adult outpatients who had completed their outpatient visits at the time of the interview. Patients who were unable to respond independently were excluded. Convenience sampling was adopted because data collection was conducted within busy outpatient settings, where systematic sampling was operationally difficult due to the continuous flow of patients and variability in consultation schedules. This approach allowed the researchers to efficiently recruit respondents immediately after their clinical visits while minimizing disruption to hospital service delivery.
A total of 3,035 outpatients initially participated in the survey. After data cleaning procedures, including the exclusion of incomplete questionnaires and responses with logical inconsistencies, 2,084 outpatients were included in the final analysis.
The Survey Instrument
The questionnaire consisted of two sections. The first section collected information on respondents’ sociodemographic characteristics, including sex, age, education level, and income group. The second section included items measuring patients’ experiences of care in public hospitals.
Sociodemographic Characteristics of Outpatients in Urban and Rural Public Hospitals (N = 2,084)
To ensure contextual relevance, the questionnaire was adapted to the Indonesian healthcare setting. The wording of several items was adjusted to reflect local hospital service procedures, such as outpatient registration, queue management, and administrative processes commonly experienced by patients in Indonesian public hospitals. The instrument was reviewed by health services researchers and hospital practitioners to ensure clarity and contextual appropriateness. Minor linguistic adjustments were made to improve comprehension among respondents with different educational backgrounds.
Data Collection and Quality Control
Data were collected through face-to-face individual interviews conducted within the sampled hospitals. A team of trained interviewers was assigned to each study site, supervised by a senior researcher. Prior to data collection, all interviewers participated in a standardized training workshop covering study objectives, eligibility criteria, survey administration, and interview techniques.
Pilot interviews were conducted to ensure consistency in understanding and applying the survey instrument. Each interview lasted approximately 20–30 minutes and was conducted after patients had completed their clinical visits to minimize courtesy bias.
To ensure data quality, completed questionnaires were reviewed daily for completeness and logical consistency. Interviewers performed initial checks in pairs, followed by verification by the team leader. When necessary, missing or unclear responses were clarified through follow-up on the same or subsequent day.
Measurements of Patients’ Experiences of Care
The questionnaire initially included 43 items assessing patients’ experiences of care, developed based on literature on patient satisfaction and Patient-Reported Experience Measures (PREMs), focusing on key healthcare quality dimensions such as communication, caring attitudes, service efficiency, and facility conditions.24,25 To ensure content validity, the items were reviewed by health services researchers and hospital practitioners for relevance and clarity in the Indonesian hospital context. For analysis, the items were organized according to the structure–process–outcome framework and screened based on conceptual relevance and response clarity, resulting in 17 key items retained for the final analysis representing the most salient aspects of patient experiences.
The 17 survey questions included in the analysis are summarized in Suplement table 1. All selected items were measured using a five-point Likert scale, with response options ranging from 1 (most positive) to 5 (most negative).24,25 General patient satisfaction was operationalized as the outcome variable. Responses on the 5-point Likert scale were dichotomized for comparative analysis. Scores of 1 and 2 were categorized as positive, while scores of 4 and 5 were categorized as negative. Neutral responses (score = 3) were excluded from the dichotomized analysis to minimize misclassification bias.
Statistical Analysis
Descriptive statistics were used to summarize respondents’ characteristics and distributions of patient experiences. Likert-scale responses were dichotomized into positive and negative categories for comparative analyses.
Multivariable regression analyses were conducted to examine variations in general satisfaction by sex, age group, education level, income group, and hospital location. Dummy variables were created for categorical covariates. Differences between urban and rural hospitals were assessed using chi-square tests.
To examine the hypothesized pathways between structure, process, and patient satisfaction, Structural Equation Modeling (SEM) was applied using the Partial Least Squares (PLS) approach. PLS-SEM was selected due to its suitability for complex models with multiple latent variables and its minimal distributional assumptions. 26 In addition to the latent constructs included in the structural model, several sociodemographic variables (sex, age group, education level, and income group) were treated as control variables in the analysis to account for potential differences in patient satisfaction across respondent characteristics. The PLS-SEM model specification included structural factors, care process variables, and technology-supported services as predictors of general patient satisfaction, with separate models estimated for urban and rural hospitals.
Measurement model quality was assessed through construct reliability (Cronbach’s alpha, composite reliability, and rho_A), convergent validity (average variance extracted), and discriminant validity (Fornell–Larcker and HTMT criteria). 26 Multicollinearity was evaluated using variance inflation factor (VIF) values. Structural model results were interpreted using standardized path coefficients, bootstrapped significance tests, and the coefficient of determination (R2) for general satisfaction.
All analyses were conducted using SmartPLS (version 3.0) and SPSS (version 22.0), with a significance level set at 5%. Although the conceptual framework included multiple process-related dimensions, only statistically significant paths are presented in the final path models to ensure parsimony and interpretability. 26 Non-significant paths were retained in the estimation process but omitted from the figures.
Ethical Considerations
As this study involved non-invasive individual interviews without physical, chemical, or biological interventions, it posed minimal risk to participants. All research procedures were conducted in accordance with applicable national regulations and the principles of the Declaration of Helsinki. Ethical standards were strictly upheld throughout the study. Participants were fully informed about the purpose of the research, assured of the confidentiality and anonymity of their responses, and informed of their right to decline or withdraw from participation at any time without consequences. Prior to the interview, trained interviewers explained the study objectives, procedures, and voluntary nature of participation in clear and accessible language. In rural hospital settings, particular attention was given to ensuring that participants clearly understood the information provided, considering potential differences in educational background and health literacy. Interviewers were trained to communicate the study information in culturally appropriate ways and to allow participants sufficient time to ask questions before agreeing to participate. Oral informed consent was obtained from all participants before the interview commenced. Oral informed consent was obtained from all participants prior to data collection. The study protocol was reviewed and approved by the Institutional Review Board.
Result
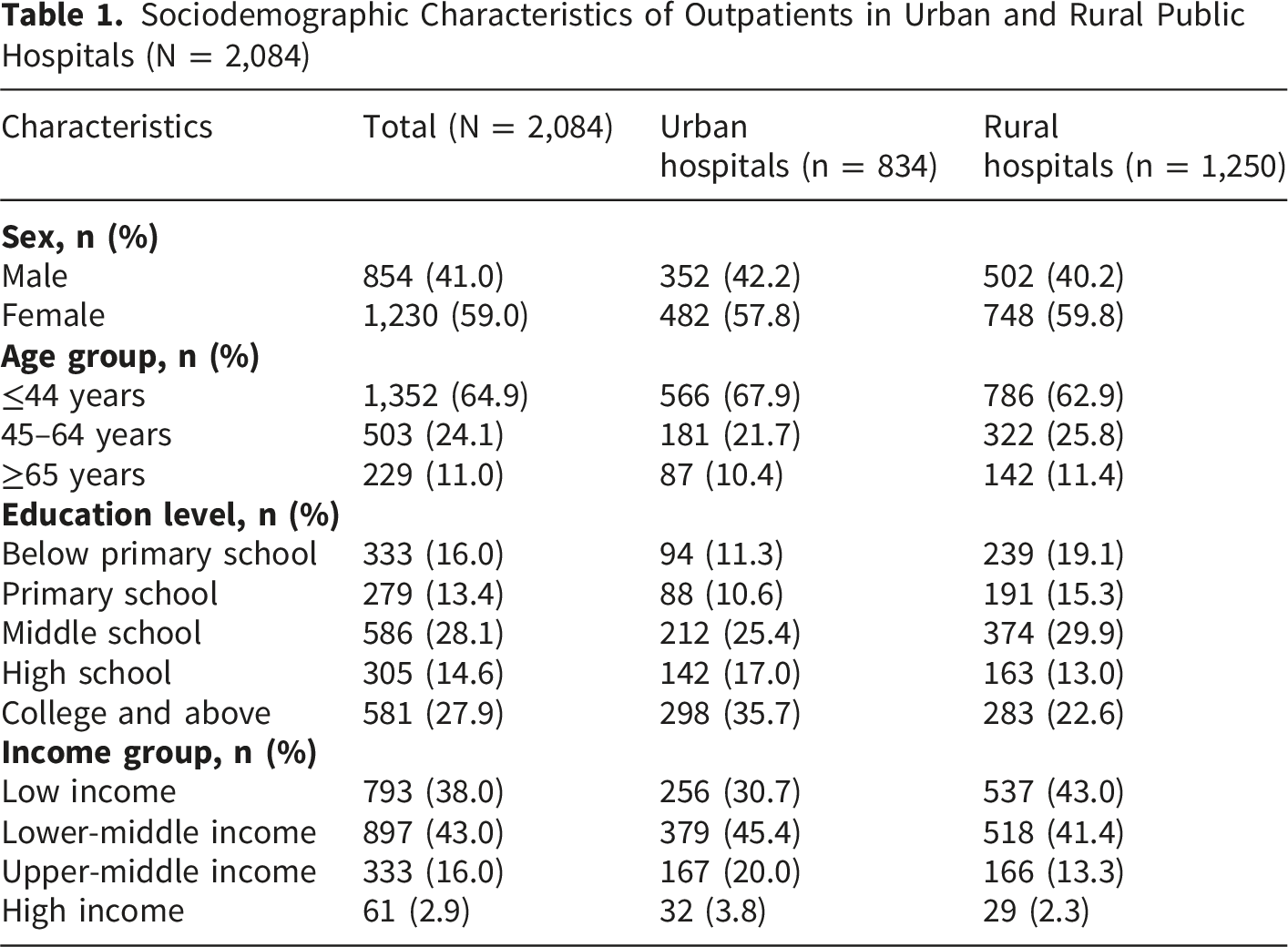
Table 1 presents the sociodemographic characteristics of the outpatients included in the study, stratified by hospital location. Of the 2,084 respondents, 834 attended urban hospitals and 1,250 attended rural hospitals. Overall, females constituted the majority of the sample (59.0%), with a similar distribution observed in both urban and rural settings.
Most outpatients were aged 44 years or younger (64.9%), although a higher proportion of younger patients was observed in urban hospitals (67.9%) compared with rural hospitals (62.9%). Conversely, rural hospitals had a slightly higher proportion of patients aged 45–64 years and 65 years or older. Regarding educational attainment, clear differences were evident by hospital location. Urban hospitals served a substantially higher proportion of patients with college-level education or above (35.7%) compared with rural hospitals (22.6%), whereas lower levels of education were more prevalent among outpatients attending rural hospitals.
Income distribution also varied between settings. A greater proportion of rural outpatients belonged to the low-income group (43.0%) compared with those attending urban hospitals (30.7%). In contrast, upper-middle and high-income groups were more commonly represented among urban hospital attendees. These patterns indicate marked socioeconomic differences between patients attending urban and rural public hospitals, underscoring the importance of accounting for contextual variation in subsequent analyses.
Multiple Regression Analysis of Factors Associated With Outpatients’ General Satisfaction With Care (N = 2,084)

Dependent variable: General patient satisfaction (Likert scale; higher values indicate higher satisfaction). Regression coefficients represent the magnitude and direction of the association between each variable and patient satisfaction. Reference category: aMale, b18–44 years, cNo formal education, dLow income, eUrban hospitals
Model 1 includes sociodemographic variables only.
Model 2 additionally adjusts for hospital location.
p < 0.05*, p < 0.01**, p < 0.001***.
After adjusting for hospital location in Model 2, the positive association between age and satisfaction remained statistically significant. Outpatients aged 45–64 years and 65 years or older continued to report higher satisfaction compared with younger respondents. In contrast, sex was not significantly associated with satisfaction in either model. Educational attainment showed a positive association with satisfaction in Model 1, with outpatients holding a college-level education or above reporting higher satisfaction; however, this association was attenuated and became non-significant after hospital location was included in the model.
Hospital location was significantly associated with patient satisfaction in Model 2. Outpatients attending rural hospitals reported significantly lower satisfaction compared with those attending urban hospitals, even after controlling for sociodemographic characteristics. Income group was not significantly associated with satisfaction in either model. Overall, these findings indicate that age and hospital location were the primary factors associated with outpatients’ satisfaction in this study.
Outpatients’ Experiences of Care by Rural and Urban Level Hospitals
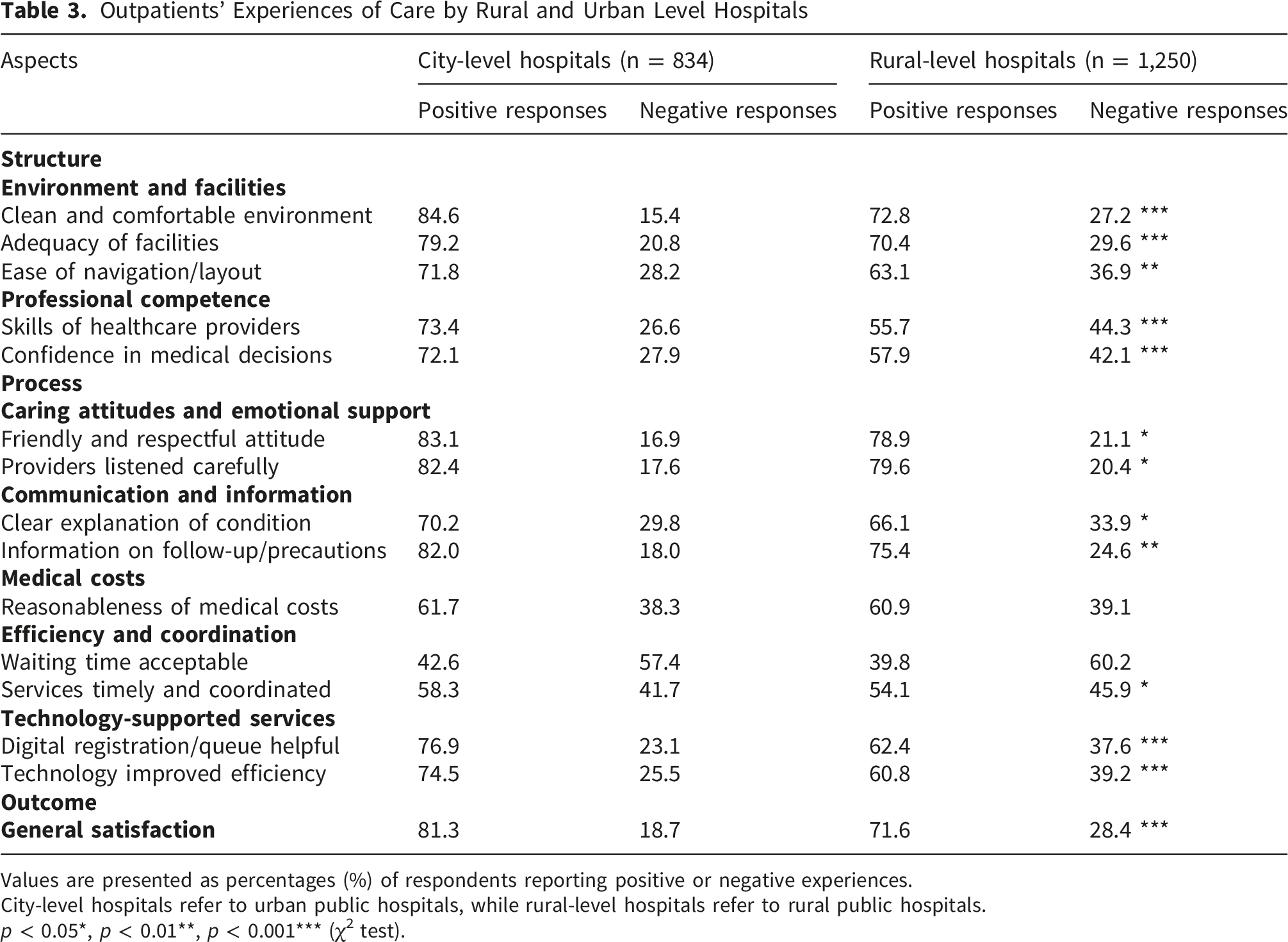
Values are presented as percentages (%) of respondents reporting positive or negative experiences.
City-level hospitals refer to urban public hospitals, while rural-level hospitals refer to rural public hospitals.
p < 0.05*, p < 0.01**, p < 0.001*** (χ2 test).
Marked differences were observed in structural aspects of care. Urban hospitals showed substantially higher proportions of positive responses regarding the hospital environment, adequacy of facilities, and professional competence of healthcare providers. These differences were statistically significant and were more pronounced for perceptions of professional competence, indicating stronger confidence in clinical skills and decision-making among outpatients treated in urban hospitals.
Differences were also evident in process-related aspects of care. Outpatients in urban hospitals reported more positive experiences related to caring attitudes, emotional support, and communication and information provision. In contrast, perceptions of medical costs and waiting time were relatively similar between the two settings, with no substantial differences in the proportion of positive responses. Notably, technology-supported services received significantly higher positive ratings in urban hospitals than in rural hospitals, highlighting disparities in the availability and perceived usefulness of digital-enabled services.
Regarding overall outcomes, general satisfaction was significantly higher among outpatients attending urban hospitals compared with those attending rural hospitals. Taken together, the findings presented in Table 4 indicate consistent urban–rural differences in patients’ experiences of care, particularly in structural conditions, care processes, and technology-supported services. These findings provide descriptive evidence supporting the study’s central research question regarding urban–rural variation in patient satisfaction and service experiences.
Model Fit Assessment
The adequacy of the measurement and structural models was evaluated prior to interpreting the path coefficients. Overall, the results indicated that the proposed PLS-SEM models demonstrated an acceptable fit to the data. The standardized root mean square residual (SRMR) values for both the city-level and rural-level hospital models were below the recommended threshold of 0.08, suggesting a satisfactory approximate model fit.
Construct reliability was supported across all latent variables. The values of ρA, Cronbach’s alpha, and composite reliability exceeded the minimum acceptable level of 0.70, indicating adequate internal consistency of the measurement scales. In addition, convergent validity was confirmed, as the average variance extracted (AVE) values for all constructs were above the recommended cutoff of 0.50. Discriminant validity was assessed using both the Fornell–Larcker criterion and the heterotrait–monotrait ratio (HTMT). The square roots of AVE for each construct were greater than the corresponding inter-construct correlations, and all HTMT values were below the threshold of 1.00, supporting satisfactory discriminant validity. Finally, assessment of multicollinearity indicated no major concerns, as all variance inflation factor (VIF) values were below 5.0. Taken together, these results suggest that the measurement and structural models were statistically adequate for subsequent analysis of direct and indirect effects.
Figure 2 presents the path model for urban hospitals, showing that structural factors influenced outpatients’ general satisfaction through both direct and indirect pathways. Environment and facilities and professional competence demonstrated significant direct effect toward general patient satisfaction (β = 0.170, p<0.001 and β = 0.197, p<0.001). The result of this study reveals that the care process dimension, including caring attitudes and emotional support, communication and information, (c) medical costs, efficiency and waiting time, and technology-supported services are positively related to general satisfaction. With regard to the mediating effect, this study confirms that caring attitudes and technology supported services mediate the relationship between environment and facilities and general patient satisfaction (β = 0.163, p<0.001 and β = 0.072, p<0.001). In addition, professional competence has indirect effect towards general patient satisfaction through caring attitudes and technology-supported services shows significant indirect effect in the relationship between environment and facilities toward general satisfaction (β = 0.155, p<0.001 and β = 0.068, p<0.001) Overall, the model explained 44.9% of the variance in outpatients’ general satisfaction (R2 = 0.449) table 5 and table 6 present direct and indirect effect. Path coefficient urban level
Figure 3 depicts the path model for rural hospitals, indicating that structural factors influenced outpatients’ general satisfaction through both direct and indirect pathways. Environment and facilities and professional competence demonstrated significant indirect effects on general satisfaction through care process variables, with indirect coefficients of β = 0.190 and β = 0.131, respectively, as shown in Table 6. In addition, technology-supported services also mediated these relationships, although with smaller indirect effects. Caring attitudes and emotional support exhibited the strongest direct association with general satisfaction (β = 0.188, p < 0.001), while technology-supported services also showed a significant but comparatively smaller direct effect (β = 0.121, p < 0.001). Overall, the model explained 46.3% of the variance in outpatients’ general satisfaction (R2 = 0.463). Path coefficient rural area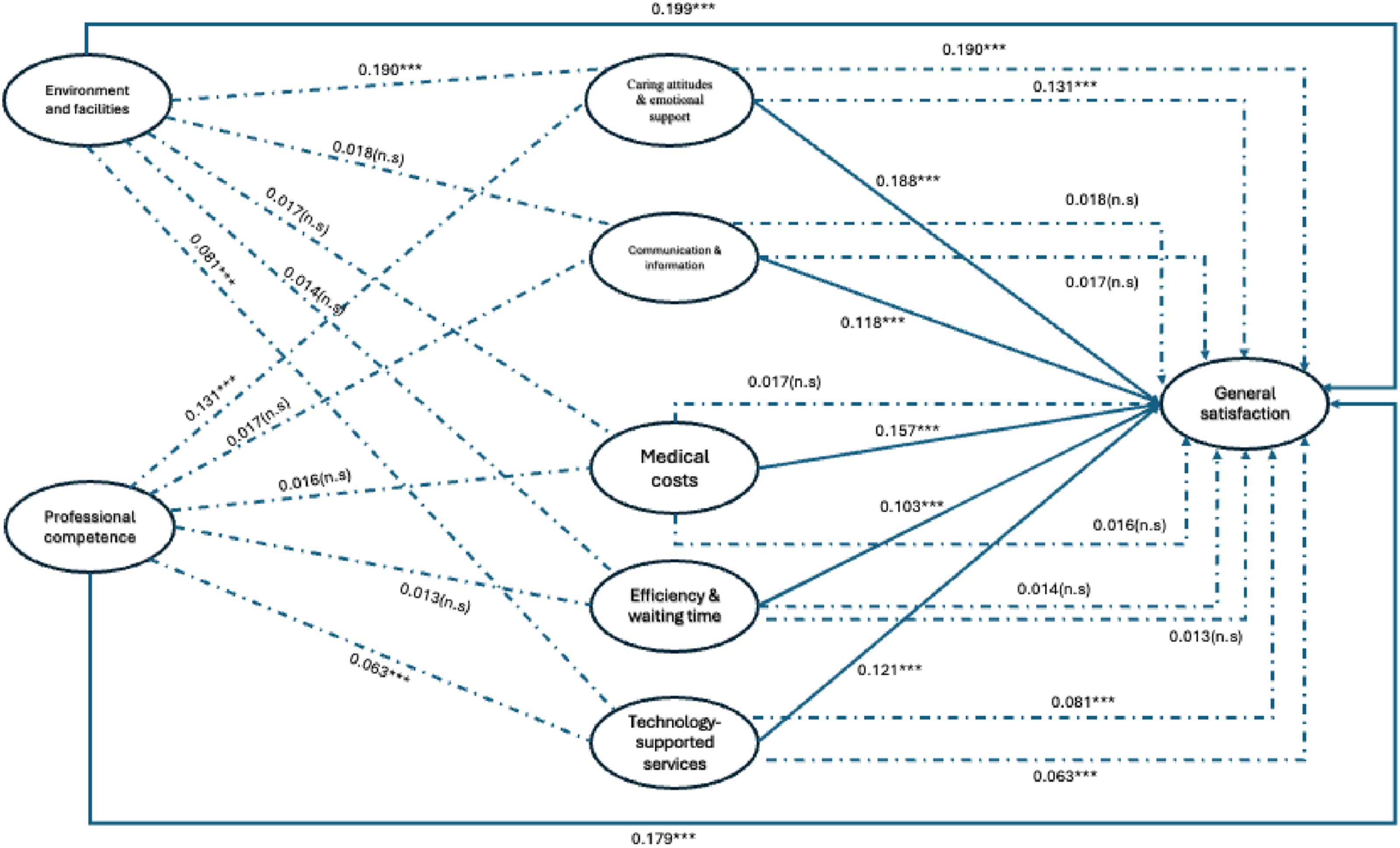
Overall, the results provide support for most of the proposed hypotheses. Structural factors, including environment and facilities and professional competence, were positively associated with general patient satisfaction, supporting H1 and H2. Care process factors, particularly (a) caring attitudes and emotional support, (b) communication and information, (c) medical costs, (d) efficiency and waiting time, and (e) technology-supported services show positive association towards general satisfaction. Therefore, H3 was supported. Regarding the mediating effect, this study reveals that only caring attitudes and emotional support, and technology-supported services mediate the relationship between environment and facilities and general patient satisfaction. Therefore hypothesis 4 was partially supported. Furthermore, this study confirms that only caring attitudes and emotional support, and technology-supported services that mediates the relationship between professional competence and general patient satisfaction. Thus, H5 was partially supported.
Discussion
This study examined the pathways linking healthcare structure and process factors to outpatients’ general satisfaction in public hospitals in East Kalimantan, Indonesia, with particular attention to differences between urban-level and rural-level hospitals. By extending Donabedian’s structure process outcome framework to incorporate technology supported services, this study provides novel empirical evidence on how digital enabled processes shape patient satisfaction in a geographically diverse and resource-constrained health system.
Consistent with Donabedian’s theoretical propositions, structural factors demonstrated both direct and indirect effects on patient satisfaction. In city-level hospitals, professional competence showed a strong direct association with general satisfaction, reflecting patients’ expectations for technical expertise and clinical confidence in more advanced healthcare settings.27,28 Urban hospitals typically serve patients with higher educational attainment and greater exposure to alternative healthcare providers, which may heighten sensitivity to perceived clinical competence.29,30
Although this study is primarily grounded in Donabedian’s structure–process–outcome framework, the findings may also be interpreted through broader perspectives on patient satisfaction and healthcare service quality. For example, service quality models such as the SERVQUAL framework emphasize the importance of reliability, responsiveness, assurance, empathy, and tangible aspects of care in shaping patient perceptions.13,16 The strong influence of caring attitudes, emotional support, and communication identified in this study aligns with the relational and responsiveness dimensions highlighted in these models. 13 In addition, the role of technology-supported services in improving efficiency and coordination reflects emerging perspectives in digital health research that view technology as an enabler of patient-centered care rather than merely a structural resource.
In contrast, in rural-level hospitals, environment and facilities emerged as the most influential structural determinant of satisfaction. This finding underscores the importance of basic infrastructure and physical conditions in rural healthcare settings, where limitations in facilities, equipment, and spatial comfort remain prominent challenges.30,31 Improvements in the physical environment may therefore yield substantial gains in perceived service quality and satisfaction in rural hospitals, even in the absence of advanced technologies. 32
Across both urban and rural settings, process-related variables played a central role in shaping patient satisfaction, supporting prior evidence that patients evaluate healthcare quality largely through their lived experiences during care delivery. Caring attitudes and emotional support consistently exhibited strong direct effects on satisfaction in both settings, highlighting the universal importance of interpersonal care, empathy, and respect in patient–provider interactions. This finding aligns with studies in other low and middle-income countries, where relational aspects of care often outweigh purely technical considerations in shaping patient perceptions.33,34
Nonetheless, variation was observed in the relative influence of specific process dimensions. In urban hospitals, communication and information provision demonstrated a stronger influence on satisfaction, reflecting higher patient expectations regarding clarity of explanations, shared decision-making, and informational transparency. Conversely, in rural hospitals, the influence of communication was comparatively weaker, suggesting that patients may prioritize relational warmth and basic service adequacy over detailed information exchange.
A key contribution of this study is the explicit modelling of technology-supported services as part of the care process. The findings indicate that technology-supported services exerted a significant direct effect on patient satisfaction in both urban and rural hospitals, confirming the growing relevance of digital tools in healthcare delivery. In urban hospitals, the effect of technology was relatively strong, likely reflecting more widespread implementation of electronic registration systems, digital queue management, and hospital information systems.
Importantly, technology-supported services also played a mediating role, transmitting the effects of structural factors such as environment and professional competence onto patient satisfaction. This suggests that technology functions not merely as an isolated service feature, but as a process enabler that enhances efficiency, coordination, and patient experiences when supported by adequate structural capacity. 35 In rural hospitals, although the magnitude of the technology effect was smaller, its statistical significance indicates that even modest digital interventions may contribute meaningfully to improving patient satisfaction. 36 However, our findings extend this literature by conceptualizing technology-supported services not merely as technological resources but as process-enabling mechanisms embedded within care practices. This perspective highlights how technology interacts with interpersonal care and structural capacity to shape patient experiences.
The observed differences between city- and rural-level hospitals highlight persistent urban–rural inequities in healthcare delivery in Indonesia. While urban hospitals benefit from better human resources and technological infrastructure, rural hospitals remain more dependent on fundamental structural improvements and interpersonal care processes. These findings reinforce the need for context sensitive policy interventions, rather than one size fits all approaches to healthcare quality improvement.
These urban–rural differences should be understood within the broader context of Indonesia’s healthcare system, which is shaped by its archipelagic geography and the uneven distribution of health resources. Urban hospitals generally have greater access to specialist physicians, more advanced technological infrastructure, and stronger institutional capacity, whereas rural hospitals often face shortages of health personnel, limited facilities, and lower access to digital health systems. 29 These structural inequalities influence both the availability and quality of services, which in turn affect patients’ experiences and satisfaction with care. 29 From a policy perspective, the findings highlight the need to address these disparities through strengthened healthcare infrastructure, more equitable workforce distribution, and expanded implementation of digital health technologies in rural hospitals6, 18. Improving hospital information systems, digital queue management, and telehealth services may help enhance service efficiency and patient experiences, particularly in geographically dispersed regions, while continued investment in communication skills and patient-centered care training for health professionals may further improve satisfaction across both urban and rural healthcare settings.
For urban hospitals, investments in workforce development, communication skills, and advanced digital systems may yield the greatest returns in patient satisfaction. For rural hospitals, prioritizing improvements in physical infrastructure, basic service organization, and staff support alongside gradual integration of appropriate technologies may be more effective and sustainable.
Not all hypothesized process dimensions demonstrated significant direct effects on patient satisfaction in the final path models. Variables such as medical cost transparency and waiting time did not retain independent significance when modelled simultaneously with other process indicators. This does not imply that these aspects are unimportant, but rather suggests that their influence may be indirect, context dependent, or subsumed by broader efficiency and relational constructs.
The findings of this study carry important implications for health system strengthening in Indonesia. First, improving patient satisfaction requires simultaneous attention to structural capacity and care processes, rather than isolated interventions. Second, technology adoption should be viewed as a complementary strategy, integrated with human resources and organizational processes, rather than as a standalone solution. Third, addressing urban rural disparities demands differentiated strategies that reflect local needs, resource constraints, and patient expectations.
Strengths and Limitations
Beyond these methodological strengths, this study makes an important contextual contribution by focusing on public hospitals in East Kalimantan, a province characterized by pronounced geographic dispersion and urban–rural disparities. By explicitly distinguishing between city level and rural level hospitals, the analysis captures heterogeneity in patient experiences that is often obscured in national-level studies. This stratified approach enhances the policy relevance of the findings, as it allows decision-makers to identify setting-specific priorities for quality improvement rather than relying on aggregate indicators that may mask local challenges.
Another notable strength of this study lies in the extension of the traditional Donabedian framework through the explicit inclusion of technology-supported services as a process-related construct. While previous studies have primarily focused on interpersonal and organizational dimensions of care processes, this study empirically demonstrates that digital-enabled services constitute a meaningful pathway linking structural capacity to patient satisfaction. By modeling technology both as a direct determinant and as a mediator, the study provides novel insights into how digital health interventions can complement human resources and infrastructure in improving patient-centered outcomes, particularly in low and middle-income settings.
A substantial proportion of the initial sample (951 out of 3,035 respondents, approximately 31%) was excluded due to incomplete or inconsistent responses during data cleaning. This level of attrition represents a potential source of non-response bias and may threaten the internal validity of the study. Although data cleaning was necessary to ensure the quality and consistency of the analysis, the exclusion of a large proportion of respondents may limit the representativeness of the final sample and should be interpreted with caution. Another limitation of this study is that detailed information on patients’ clinical conditions or diagnoses was not collected. Since determinants of patient satisfaction may vary across different disease types or clinical specialties, the absence of case-mix information may limit the ability to examine condition-specific variations in patient experiences.
Finally, the use of PLS-SEM with subgroup analyses represents a methodological strength that allows for nuanced examination of complex relationships across different hospital contexts. Compared with conventional regression approaches, PLS-SEM enables simultaneous estimation of multiple latent constructs and indirect effects, offering a more comprehensive understanding of how patient satisfaction is formed. The comparison between urban and rural models further strengthens the robustness of the findings and highlights structural inequities within the health system. Together, these strengths position the study as a valuable contribution to the literature on patient-reported experiences and healthcare quality, while also providing a foundation for future research to build upon and refine the proposed framework.
Practical Implications
The findings of this study suggest that efforts to improve outpatient satisfaction should focus on reconfiguring care practices, rather than relying solely on technological adoption. Hospital managers should prioritize strengthening interpersonal care competencies, including empathy, communication, and patient engagement, as these factors consistently shape patient satisfaction across settings. Investments in technology-supported services should be aligned with existing workflows and staff capacity to ensure that digital tools enhance, rather than complicate, care delivery. For rural hospitals, practical interventions may include improving basic facilities, simplifying digital registration or queue systems, and providing targeted training for health workers to integrate technology into daily practice. In urban hospitals, greater emphasis on professional development, advanced information systems, and coordinated digital services may further enhance patient experiences. Collectively, these findings highlight the importance of context sensitive managerial strategies that integrate human resources, infrastructure, and technology to reduce urban rural disparities in public hospital services.
Conclusion
Using a structure process outcome framework, this study demonstrates that outpatients’ general satisfaction in public hospitals is shaped by interconnected pathways linking structural conditions to patients’ experiences of care. Care processes particularly caring attitudes and emotional support emerged as central determinants of satisfaction across both city and rural hospitals. However, the relative importance of structural factors differed by context, with professional competence playing a more prominent role in urban hospitals and environment and facilities being more influential in rural hospitals. By extending the framework to include technology-supported services, this study provides new evidence that digital-enabled processes contribute meaningfully to patient satisfaction and mediate the effects of structural factors. These findings highlight the need for context-sensitive strategies to improve healthcare quality, combining investments in infrastructure, human resources, and appropriate technologies to address persistent urban rural disparities in public hospital services. From a policy perspective, improving patient satisfaction in Indonesia requires targeted investments in rural healthcare infrastructure, equitable distribution of health professionals, and expansion of digital health systems such as electronic registration and queue management. Strengthening communication skills and patient-centered care training for healthcare workers may further enhance patient experiences across hospital settings. These strategies may help reduce urban–rural disparities and support ongoing efforts to improve healthcare quality in Indonesia’s public hospital system. Future research should further explore the long-term impact of technology-supported services on patient satisfaction, particularly through longitudinal designs that can capture changes in patient experiences as digital health systems continue to evolve.
Supplemental Material
Supplemental Material - Reconfiguring Care Practices Through Technology-Supported Services: Pathways to Outpatient Satisfaction in Urban and Rural Public Hospitals
Supplemental Material for Reconfiguring Care Practices Through Technology-Supported Services: Pathways to Outpatient Satisfaction in Urban and Rural Public Hospitals by Ferry Fadzlul Rahman, Herni Johan and Jovi Sulistiawan in Inquiry: The Journal of Health Care Organization, Provision, and Financing.
Supplemental Material
Supplemental Material - Reconfiguring Care Practices Through Technology-Supported Services: Pathways to Outpatient Satisfaction in Urban and Rural Public Hospitals
Supplemental Material for Reconfiguring Care Practices Through Technology-Supported Services: Pathways to Outpatient Satisfaction in Urban and Rural Public Hospitals by Ferry Fadzlul Rahman, Herni Johan and Jovi Sulistiawan in Inquiry: The Journal of Health Care Organization, Provision, and Financing.
Supplemental Material
Supplemental Material - Reconfiguring Care Practices Through Technology-Supported Services: Pathways to Outpatient Satisfaction in Urban and Rural Public Hospitals
Supplemental Material for Reconfiguring Care Practices Through Technology-Supported Services: Pathways to Outpatient Satisfaction in Urban and Rural Public Hospitals by Ferry Fadzlul Rahman, Herni Johan and Jovi Sulistiawan in Inquiry: The Journal of Health Care Organization, Provision, and Financing.
Footnotes
Acknowledgments
The author gratefully acknowledges the support of the participating public hospitals in East Kalimantan and thanks all outpatients who voluntarily took part in this study.
Ethical Considerations
This study was conducted in accordance with the Declaration of Helsinki and relevant national regulations. Ethical approval was obtained from the
Consent to Participate
All participants were informed about the purpose of the study, assured of anonymity and confidentiality, and provided oral informed consent prior to participation.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The author declares that there is no conflict of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Anonymity for Peer Review
In line with SAGE’s double-blind peer review requirements, all identifying information related to the author(s), institutions, ethics committees, and funding sources has been removed from the main manuscript and is provided only on this title page.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.