
Abstract
Digital health promises a revolution in healthcare delivery, yet in low and middle-income countries (LMICs), a stark digital divide threatens to exacerbate health inequities. While innovations like telemedicine and mobile health apps have surged globally post-COVID-19, millions in LMICs remain excluded due to poor internet access, unaffordable devices, and low digital literacy, especially in rural areas. This perspective piece examines the current landscape, highlighting successes like Uganda’s mTrac for disease tracking alongside systemic barriers such as weak data privacy. Drawing on local experiences from Sierra Leone, the paper underscores the urgency of tailored solutions. We propose a vision for equity through public-private partnerships, community-based digital literacy programs, robust ethical safeguards, and a novel regional digital health equity taskforce to drive coordinated action. Urgent intervention from governments, global health bodies, and the private sector is needed to reframe digital health as a public good, ensuring access for all and transforming care for the most marginalized.
Keywords
Introduction
In a small village in rural Malawi, a mother waits anxiously for news about her child’s persistent fever, but the nearest clinic is a three-hour walk away, and she lacks the means to travel. Meanwhile, in urban centres across the globe, telemedicine platforms connect patients to doctors within minutes, offering diagnoses and prescriptions through a smartphone screen. 1
The rise of digital health, encompassing tools like telemedicine, mobile health applications, and artificial intelligence for diagnostics, has been heralded as a game-changer for healthcare delivery, especially since the COVID-19 pandemic accelerated its adoption worldwide.2,3 Reports suggest that global telemedicine consultations surged by over 60 percent during the height of the crisis, transforming how care is accessed in many settings. 2 Yet, for millions in LMICs, where less than 20 percent of rural populations have reliable internet access, these innovations remain out of reach, confined to those with the privilege of connectivity and resources. 2
In LMICs, barriers such as poor infrastructure, prohibitive costs of devices, and low digital literacy mean that the very communities who could benefit most from these tools are often excluded. 4 While LMICs share common challenges, they are far from homogeneous. Sub-Saharan Africa, for example, faces significant barriers such as limited internet penetration and fragile health systems, whereas South Asia, despite infrastructure gaps, has seen a faster uptake of mobile technology. 5 Additionally, country-specific factors such as urban-rural divides, affordability, and sociocultural norms—like language barriers and gender disparities—further shape the adoption and effectiveness of digital health interventions. 5 Recognizing this diversity is critical for designing context-sensitive strategies that advance equity across LMICs.
In Sierra Leone, for instance, rural health workers in the Western Area often lack basic smartphones to access training apps rolled out during the Ebola recovery phase, depicting how even post-crisis digital initiatives fail without addressing access gaps. 6 A farmer in rural India might miss out on a life-saving teleconsultation because they cannot afford a smartphone, while a woman in sub-Saharan Africa might struggle to use a health app due to language barriers or lack of training.
The urgency to address this issue cannot be overstated. As the world rebuilds health systems in the aftermath of the pandemic, there is a narrow window to ensure that digital health becomes a tool for inclusion rather than exclusion. This perspective piece argues that without deliberate policy interventions, targeted investments, and global collaboration, the digital health revolution will fail to deliver on its promise of universal access. We must reimagine digital health as a public good, not a luxury, and commit to bridging the access gap through a multi-stakeholder approach that prioritizes the needs of LMICs. Only then can we transform the narrative from one of disparity to one of empowerment, ensuring that a mother in Malawi has the same chance to save her child as a parent in a high-income city. This perspective piece explores the current landscape of digital health in LMICs, propose a vision for equity, and issue a call to action for transformative change.
The Current Landscape of Digital Health in Low and Middle-Income Countries
The landscape of digital health in LMICs offers a mix of inspiring progress and daunting challenges, reflecting both the potential and the pitfalls of technology in addressing health disparities. Over the past decade, several initiatives have demonstrated how digital tools can transform care delivery in resource-constrained settings. Similarly, in South Asia, projects like the eHealth initiative in Bangladesh have leveraged basic mobile technology to provide health education and reminders for vaccinations, reaching thousands of families who might otherwise slip through the cracks of traditional healthcare systems. 7 These examples underscore the power of even low-cost, low-tech digital solutions to bridge gaps where physical infrastructure falls short. Additionally, several frameworks have been recently launched to inform digital health and equity. For instance, WHO recently launched the Global Strategy on Digital Health (2020–2025) to advance digital health with a focus on equity and universal health coverage. 8 This framework highlighted the need to strengthen digital health governance, capacity building for frontline workers, interoperability and data security, as well as inclusivity. 8 The Lancet Commission on Digital Health and AI, in 2023, highlighted the importance of equity in the design, implementation, and evaluation of digital health technologies, particularly focusing on ethical use of AI and engaging community people in technology development to ensure relevance and accessibility. 9 Furthermore, Africa Centre for Disease Control and Prevention (Africa CDC) recently launched its strategy (2025–2030) on leveraging digital health to strengthen health systems and promote equity across Africa. Interoperability, capacity building, community engagement, and data governance are key pillars of that strategy. 10 While these frameworks provide glimpse of hope for advancing digital health in LMICs, for every success story, there are countless barriers that limit the scale and impact of digital health. One of the most glaring obstacles is the lack of reliable internet connectivity, particularly in rural regions where most of the population often resides. Data from the International Telecommunication Union shows that only about 25 percent of people in sub-Saharan Africa have access to the internet, with even lower rates in rural zones. 11 Without this foundation, tools like telemedicine or web-based health apps become irrelevant for millions. Even when connectivity exists, the cost of devices and data plans remains prohibitive. A smartphone, often seen as a necessity for accessing digital health services, can cost several months’ income for a low-wage worker in a country like Nepal or Mali, creating an economic barrier that excludes the poorest from participating in the digital health ecosystem. 12 This financial hurdle is compounded by issues of digital literacy, as many in LMICs, especially older adults and women, may lack the skills to navigate apps or online platforms, even if they manage to acquire the necessary hardware. 12
Recent scholarly contributions have provided integrated analyses of digital health equity, particularly focusing on the intersection of technology, policy, and structural barriers. For example, a study by Mthabisi Talent George Moyo highlights how AI-enabled telemedicine can transform healthcare delivery in LMICs by addressing workforce shortages and improving diagnostic accuracy. 13 However, the study also underscores the critical need to address structural inequities, such as access to reliable internet and electricity, and policy barriers, including fragmented governance and weak regulatory frameworks. 13 By engaging with such literature, this manuscript situates its discussion within current scholarly discourse, emphasizing the importance of integrating technological innovation with equity-focused policies and structural reforms. Emerging technologies like AI, while promising, must be deployed with caution to avoid exacerbating existing disparities. For instance, algorithmic bias and uneven access to AI-driven tools could reinforce inequities if not addressed through inclusive design and robust governance.
Beyond access and affordability, there are deeper systemic issues that hinder the equitable rollout of digital health. Regulatory frameworks for data privacy and security are often weak or non-existent in many LMICs, raising concerns about how patient information is stored and used. In places like Kenya and South Africa, where mobile health apps have gained traction for managing chronic conditions, there have been reports of data breaches that compromise user trust. 14 Without robust policies to protect vulnerable populations, digital health risks becoming a double-edged sword, offering benefits on one hand while exposing users to exploitation on the other. Moreover, the design of many digital health tools often fails to account for local contexts, with interfaces in foreign languages or features that assume a level of technological familiarity not common in LMIC settings. A health app developed in a high-income country might be useless to a rural farmer in Ethiopia if it is not translated into Amharic or if it requires a high-speed connection that does not exist. 15
The consequence of these barriers is a perpetuation of health inequities, where digital health disproportionately benefits urban, wealthier, and more educated populations within LMICs, while leaving rural communities, women, and low-income groups behind. This mirrors broader patterns of exclusion seen in traditional healthcare systems, but with the added sting of a missed opportunity, digital health was supposed to level the playing field, not reinforce existing divides. If a pregnant woman in a remote village in India cannot access a teleconsultation due to lack of internet or a device, or if a community health worker in Sierra Leone struggles with an app due to poor training. Addressing these challenges requires not just technological solutions, but a fundamental shift in how we prioritize and design digital health interventions for the most marginalized.
Addressing the digital divide, improving access in rural areas, and tackling governance and infrastructure barriers require a forward-looking strategy that integrates technology, policy, and community engagement. The following section presents a comprehensive vision for digital health equity, outlining practical solutions and collaborative approaches that build on existing frameworks while addressing the gaps identified in the current landscape.
A Vision for Digital Health Equity
Imagining a future where digital health serves as a cornerstone of equity in LMICs requires us to rethink its role not as a shiny innovation for the few, but as a public good accessible to all. The current trajectory, where digital tools often cater to those already connected and resourced, must be redirected with intentional strategies that prioritize the most marginalized. This is not just about scaling up technology, it’s about embedding fairness into every layer of design, deployment, and policy. If we accept that health is a universal right, then the tools that enhance it, including digital health, must be framed as essential services rather than optional luxuries. This shift in perspective demands bold action from governments, global health bodies, and the private sector to ensure that a rural farmer in Ghana or a displaced family in Bangladesh can benefit from digital health just as much as an urban professional in a high-income setting. 11
This paper adopts a conceptual framework based on the Three Pillars of Digital Health Equity: Access, Usability, and Governance. These pillars serve as interconnected mechanisms that influence the success or failure of digital health initiatives in LMICs.
Access: Reliable infrastructure, affordable devices, and connectivity are foundational for digital health adoption. For example, the success of Uganda’s mTrac program was linked to its use of simple SMS technology, which required minimal infrastructure and low-cost phones. Conversely, initiatives like Sierra Leone’s Ebola recovery apps struggled due to gaps in smartphone availability and network coverage. This highlights the need for targeted interventions, such as subsidies for devices and investments in rural internet infrastructure, to address access disparities.
Usability: Digital health tools must be designed to align with local contexts, including language, cultural norms, and digital literacy levels. In South Asia, eHealth initiatives succeeded by incorporating local languages and culturally relevant health education, while failures in sub-Saharan Africa often stemmed from tools that assumed high levels of technological familiarity. Tailored training programs and co-design processes with end-users are critical to bridging usability gaps.
Governance: Effective regulatory frameworks for data security, privacy, and ethical AI are essential to build trust and ensure equitable implementation. In Kenya, data breaches in mobile health apps have undermined user confidence, emphasizing the importance of robust governance mechanisms. Establishing clear policies for data protection and accountability, supported by international bodies, can mitigate risks and promote sustainable adoption. One promising avenue to achieve this is through public-private partnerships that tackle the infrastructure gap head-on. Governments in LMICs often lack the funds to expand internet connectivity to remote areas, but collaboration with telecommunications companies could unlock solutions. Imagine a model where tech firms are incentivized through tax breaks or subsidies to build low-cost, solar-powered internet hubs in rural regions, specifically earmarked for healthcare access. Pilot programs, such as those trialled in Kenya with Safaricom’s rural connectivity projects, demonstrate that such models can be scaled with donor support from entities like the World Bank. Such initiatives could be paired with programs to distribute affordable or subsidized devices, ensuring that cost doesn’t bar entry. For instance, a program in Rwanda has already shown success in distributing low-cost smartphones to community health workers for data collection and patient follow-ups. 12 Scaling similar efforts with a focus on end-users, not just health workers, could transform access.
This vision for digital health equity is achievable with coordinated efforts from governments, global health bodies, and private sector stakeholders. For example, public-private partnerships can provide innovative solutions to address infrastructure gaps, while targeted investments and policy alignment can ensure the financial and operational feasibility of these initiatives. With adequate political will and sustained commitment, these strategies can transform access to healthcare in LMICs and foster long-term equity in digital health. While the proposed strategies offer promising pathways to advance digital health equity, their implementation faces several challenges and trade-offs that must be carefully considered:
Financial Feasibility: Expanding infrastructure and subsidizing devices require significant investments that may strain LMIC budgets. While public-private partnerships can offset costs, reliance on external funding raises concerns about long-term sustainability. Governments must prioritize health spending and explore innovative financing mechanisms, such as blended finance models, to ensure affordability without compromising other critical sectors.
Political Constraints: Political instability and competing priorities in LMICs can delay or derail digital health initiatives. For instance, governments may prioritize immediate healthcare needs over long-term investments in digital systems. Advocacy efforts and alignment with broader health goals, such as universal health coverage, are essential to secure political buy-in and sustained commitment.
Scalability: Pilot programs often succeed in small-scale implementations but face barriers when scaled nationally or regionally. Challenges include adapting interventions to diverse contexts, ensuring interoperability of systems, and maintaining quality across larger populations. Scalability requires phased implementation with continuous monitoring and evaluation to refine strategies and overcome bottlenecks.
Sustainability: Ensuring the longevity of digital health solutions requires embedding them into existing health systems and building local capacity. Dependency on donor funding or external expertise risks creating unsustainable programs. Investments in workforce training, local manufacturing of devices, and community ownership of initiatives are critical to fostering resilience and reducing reliance on external support.
Additionally, a novel regional digital health equity taskforce, comprising LMIC governments, WHO representatives, and tech innovators, could prioritize cross-border collaboration to share resources and best practices, ensuring that smaller nations like Sierra Leone are not left behind.
The proposed Regional Digital Health Equity Taskforce represents a novel contribution by addressing gaps in cross-border collaboration and resource-sharing specific to LMICs. Unlike existing global health initiatives, this taskforce would focus exclusively on digital health equity, bringing together LMIC governments, WHO representatives, regional health bodies (e.g., Africa CDC, SEARO), and private sector stakeholders. The taskforce would operate as a multi-stakeholder coalition with three core governance components: Leadership Council, Technical Working Groups, and Advisory Board. The leadership council should comprise representatives from LMIC governments, multilateral organizations, and private sector leaders, tasked with setting priorities and allocating resources. The technical working group should focus on thematic areas such as infrastructure development, digital literacy, and data governance, ensuring targeted interventions based on regional needs. Finally, the advisory board should include civil society organizations and community representatives to ensure inclusivity and accountability. The taskforce would leverage regional hubs to coordinate activities, ensuring that smaller countries with limited capacity—such as Sierra Leone—can benefit from shared expertise and resources. Funding could be sourced through partnerships with multilateral organizations like the World Bank and philanthropic contributions from technology companies. The taskforce would also establish a centralized knowledge-sharing platform, enabling LMICs to access best practices, tools, and case studies for scaling digital health solutions effectively.
Equally critical is addressing the human element of digital health through community-based digital literacy programs. Technology is only as effective as the people using it, and in many LMICs, large segments of the population, particularly women and older adults, are unfamiliar with even basic digital interfaces. Tailored training initiatives, conducted in local languages and rooted in cultural contexts, could empower communities to engage with health apps and telemedicine platforms. Picture a network of local trainers in a district of rural India, teaching mothers how to use a maternal health app to track pregnancy milestones or access emergency advice. These programs could be funded through international aid or global health grants, ensuring sustainability. Moreover, involving community leaders in the design and delivery of such training would build trust and relevance, countering the alienation often felt when foreign technologies are introduced without local input. 16
Ethical considerations must also anchor this vision, especially around data protection and patient autonomy. As digital health expands in LMICs, the risk of exploitation through data misuse grows, particularly in regions with weak regulatory oversight. Any equitable framework must include strict guidelines on how patient information is collected, stored, and shared, with clear consent processes that respect individual rights. Global health organizations could play a role here by supporting LMIC governments to draft and enforce privacy laws tailored to digital health. Additionally, the tech industry must be held accountable to design tools that prioritize user agency, ensuring that communities aren’t just passive recipients but active participants in shaping how digital health evolves. This means co-creating solutions with input from local populations, so that a health app is not just a one-size-fits-all product but a tool that reflects the realities of its users. Ensuring robust data privacy and security in LMICs requires addressing critical issues such as data sovereignty, algorithmic bias, and commercialization of health data:
Data Sovereignty: Many LMICs lack control over how their citizens’ health data is stored and processed, as data is often hosted on servers in high-income countries. This creates vulnerabilities related to unauthorized access and misuse by external entities. For example, concerns have been raised about the use of health data by foreign companies for profit-driven purposes without benefiting local populations. Strengthened national policies and investment in local data infrastructure are essential to maintain sovereignty over sensitive health information.
Algorithmic Bias: AI-driven digital health tools often rely on datasets that may not adequately represent LMIC populations, leading to biases that compromise diagnostic accuracy and equity. For instance, studies have shown that AI-powered diagnostic tools trained on data from high-income countries perform poorly when applied to LMIC populations due to differences in genetic, environmental, and socioeconomic factors. Co-developing algorithms with local datasets and conducting equity-focused evaluations can mitigate these biases.
Commercialization of Health Data: The growing involvement of private technology companies in digital health raises concerns about the monetization of health data. Without clear regulations, patient data could be exploited for commercial gains, undermining trust in digital health systems.
Governance Mechanisms and International Standards: Effective governance mechanisms are crucial to address these risks. LMIC governments should adopt comprehensive data protection laws that align with international standards, such as the General Data Protection Regulation (GDPR), while tailoring them to local contexts. International bodies like the WHO can support LMICs in developing these frameworks and ensuring compliance. Additionally, global coalitions should promote ethical AI standards and equitable data-sharing agreements to prevent exploitation and foster trust.
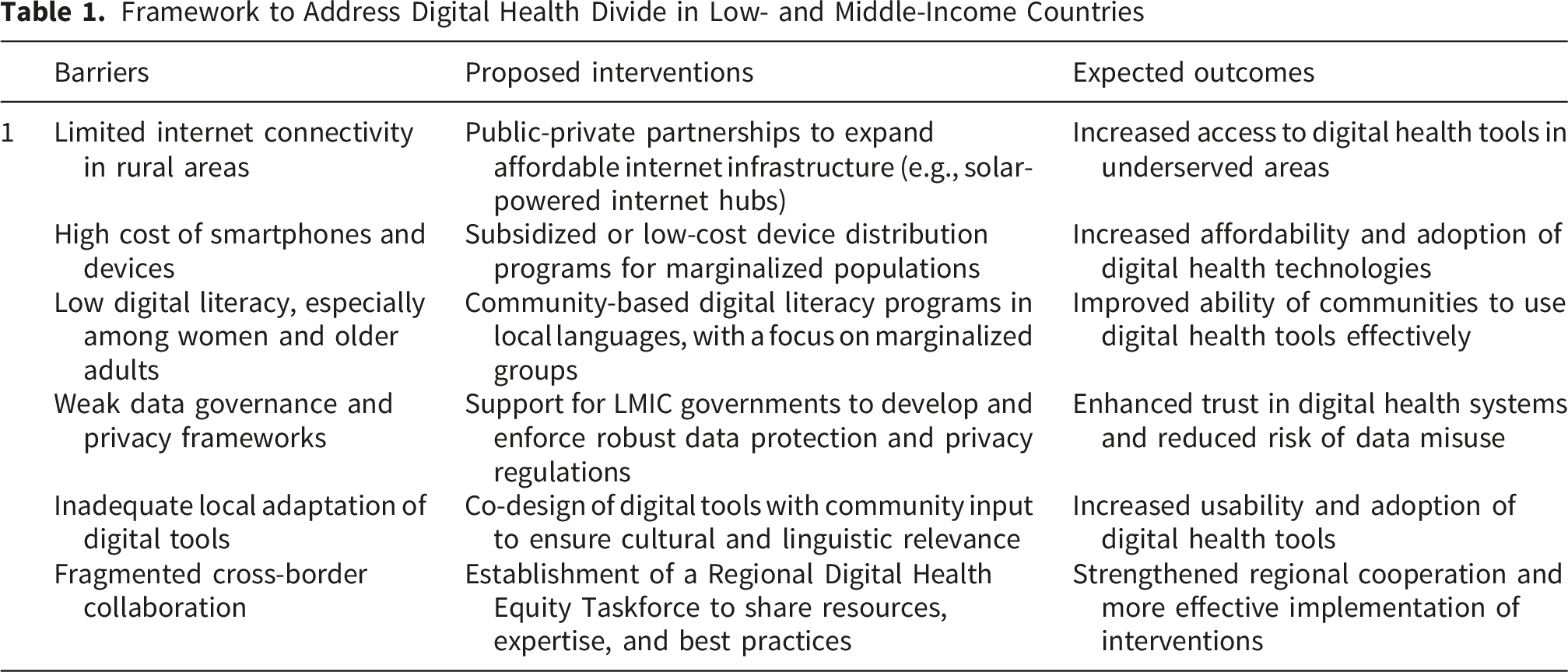
Framework to Address Digital Health Divide in Low- and Middle-Income Countries
Call to Action
The time to act on digital health equity in LMICs is now, before the digital divide becomes an insurmountable chasm in global health. The disparities in access, affordability, and literacy that currently plague the rollout of digital health tools are not inevitable; they are the result of choices made or neglected by policymakers, industry leaders, and global health stakeholders. If we are keen about the Sustainable Development Goal of ensuring healthy lives and well-being for all, then bridging this divide must become a priority, not an afterthought. 15 This requires a collective commitment to reframe digital health as a fundamental right, demanding urgent and coordinated action across sectors to ensure that no one is left behind, whether they live in a bustling city or a remote village.
Short-Term Priorities
Governments in LMICs must take the lead by integrating digital health equity into national health strategies, with clear budgets and timelines for expanding internet infrastructure and subsidizing devices for underserved populations. Phased implementation, starting with pilot districts, as seen in Rwanda’s health worker smartphone program, provides a feasible model for scaling. International donors and organizations like the World Health Organization should prioritize funding and technical support for projects targeting rural and marginalized communities.
Medium-Term Priorities
The global health community must advocate for and invest in capacity building, ensuring that digital literacy becomes a core component of health programs in LMICs. This includes training not only health workers but also communities, with a focus on women, elderly individuals, and other groups often excluded from technological advancements. Grassroots organizations and local governments can play a pivotal role in delivering these programs. Success can be assessed by tracking metrics such as the number of health workers trained in digital health tools and the percentage of community members who can effectively use these technologies.
Long-Term Priorities
In the long term, robust data protection laws and sustainable governance mechanisms must be established to safeguard trust in digital health systems. International bodies should provide templates and technical support for LMICs to adapt and enforce these regulations. The private sector, particularly technology and telecommunications companies, must also be held accountable to contribute through innovative partnerships. Examples include providing low-cost data plans for health-related services or co-developing tools with local input to ensure cultural and linguistic relevance. Success can be measured through the adoption rates of digital health tools, the establishment of data protection frameworks, and the reduction in digital health disparities over time.
Conclusion
The digital health revolution holds immense potential to transform healthcare in LMICs, but only if we consciously steer it toward equity. The stories of mothers waiting for care in rural Malawi or farmers unable to afford a smartphone in India are not just anecdotes, they are urgent reminders of what’s at stake. We stand at a crossroads where digital health can either deepen existing inequities or become a powerful equalizer, but the outcome depends on the decisions we make today. Let us choose a path of inclusion, where technology serves as a bridge rather than a barrier, ensuring that every individual, regardless of location or income, can access the care they deserve. The window for transformational change is narrow, but it is open. It is up to all of us, from policymakers to practitioners to private enterprises, to act with the urgency and vision required to make digital health a reality for all. Only then can we honour the promise of health as a universal right in the digital age. 17
Footnotes
Author Contributions
AO contributed to the study design and conceptualisation. AO developed the initial draft. US critically reviewed the manuscript for its intellectual content. Both authors read and amended drafts of the paper and approved the final version. US had the final responsibility of submitting it for publication.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.