
Abstract
Introduction
The interlinked metabolic disorders—obesity and dyslipidemia—significantly increase cardiovascular and mortality risks in adults. 1 The global obesity rate has more than doubled since 1990. As of 2022, approximately 1 in 8 people worldwide are living with obesity, 2 and 1 in 3 Korean adults (34.4%) is now classified as obese. 3 Obesity, especially the central adiposity frequently observed in middle-aged populations, serves as a primary driver of hypertriglyceridemia (hyperTG) through a complex interplay of lipid oversupply and metabolic dysfunction. 1 In South Korea, adult male obesity reached an all-time high of nearly 49.7% post-pandemic, a direct result of decreased physical activity and the rise of the “delivery food” culture during the coronavirus disease pandemic. 4 The prevalence of hyperTG is also increasing in most Asian countries; this trend is particularly alarming among South Korean men in their 40s and 50s, where the prevalence exceeds 50%, signaling a critical public health crisis that correlates with the rising rates of hyperTG and cardiovascular complications.5,6 Older women, who are post-menopausal, also tend to exhibit higher levels of certain lipids. 7
However, regular walking practice plays a pivotal role in mitigating obesity and elevated lipid levels by facilitating the direct utilization of circulating triglycerides (TGs) as a primary fuel source for skeletal muscles. 8 Regular physical activity, such as consistent walking, has been shown to reduce body weight by approximately 2–3 kg and lower serum TG levels by 10–25%, primarily through the activation of lipoprotein lipase and enhanced fat oxidation.9,10 However, World Health Organization data show that the global prevalence of insufficient physical activity among adults has increased from 23.4% in 2000 to 31.3% in 2022, and this prevalence is higher for women (33.8%) than for men (28.7%). 11 Although the lack of walking was evident across all age cohorts, its prevalence was most significant among older adults. Interestingly, although women generally exhibited higher participation in leisure walking than men did, this sex gap diminished or even reversed in the older age groups. 12
Accordingly, the interplay between the obesity rates, TG concentrations, and walking practice within the 40–60-year age group is manifested differently across countries, dictated by their respective life-course and societal changes. Therefore, by examining about two decades of data, in this study, we aimed to elucidate the divergent longitudinal trajectories of walking practice, obesity, and hyperTG, thereby providing a more nuanced understanding of metabolic health disparities among middle-aged South Korean adults.
The Korea National Health and Nutrition Examination Survey (KNHANES) was conducted triennially from its first phase in 1998 through the third phase in 2005. 13 Since 2007, the survey has been conducted annually, with the raw data made publicly available. 13 Trend analysis is primarily conducted to monitor changes in disease prevalence and health behaviors over time, evaluate the effectiveness of public health policies, identify health disparities among population subgroups, provide evidence for future policy planning, and understand the impact of social and epidemiological transitions on population health. 14 In this study, we utilized data from the KNHANES conducted from 2005 to 2023 to compare trends in walking activity, obesity, and hyperTG between men and women.
Methods
This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for observational studies. 15
Study Design
In this study, we performed secondary analysis of the KNHANES data collected from 2005 to 2023. Trends in hyperTG, walking, and obesity were analyzed and compared between men and women using Joinpoint regression analysis.
Data Source
The KNHANES, a statutory survey that collects information on health behavior, prevalence of chronic diseases, and diet, is conducted pursuant to Article 16 of the National Health Promotion Act. It uses the latest population and housing census data as the basic sampling frame to form a sample representative of the whole population. Participants in KNHANES were selected using multi-stage stratified cluster sampling to represent the non-institutionalized Korean population. The extraction frame was systematically stratified by province and housing category, with further implicit stratification by residential area characteristics and household demographics (e.g., age of household head and single-person household ratio). Trained researchers visited the households selected to participate in the KNHANES and conducted face-to-face interviews. From 2005 to 2023, a total of 274,339 participants aged 19 and older (standardized) were initially included: 87,069 for walking practice rates, 105,016 for obesity prevalence, and 82,265 for triglyceride (TG) levels. For the analysis, data from individuals aged 40 to 69 years were used, excluding those under 40 and over 70 years. For the analysis, data from individuals aged 40 to 69 years were used, excluding those under 40 and over 70 years, to focus on populations at higher risk of obesity and hyperTG, where these conditions are more prevalent and temporal trends can be more reliably assessed. In the final analysis, data from men and women aged 40–69 years were extracted and analyzed (total N=149,001).
Definitions
Walking practice was defined as walking for at least 10 min per session for a total of at least 30 min per day, on ≥ 5 days of the previous 7 days. HyperTG was diagnosed when TG levels were ≥ 240 mg/dL. Obesity was defined as a body mass index of ≥25 kg/m2 (excluding pregnant women). Age standardization was applied to walking practice, hyperTG, and obesity.
Ethical Approval
The KNHANES was approved by the Research Ethics Review Committee of the the Korea Disease Control and Prevention Agency. This secondary data analysis was exempted from review by the Institutional Review Board of Chungnam National University (No. 202408-SB-114-01).
Statistical Analysis
Given the complex, multistage sampling design of KNHANES, all analyses incorporated sampling weights reflecting the sampling probability, response rates, and population distribution for each survey year. Weighted means and proportions were calculated to obtain nationally representative estimates. Age-standardized estimates were calculated using the 2005 Korean population to adjust for differences in age distribution across survey years. Standardized results were presented only when the sample size for each age group was ≥20.
Trend changes in walking practice, hyperTG, and obesity over time were evaluated by calculating the annual percent changes (APCs) and average APCs (AAPCs) during the observation period using Joinpoint software version 5.2.0 (National Cancer Institute, National Institutes for Health, Bethesda, MD, USA). 14 Joinpoint regression fits a series of connected linear segments to the data, with each segment representing a different linear trend. 14 A joinpoint is a point on the time axis where the trend significantly changes its direction or slope. Joinpoints are identified by beginning with the simplest model (no Joinpoint, a single straight line) and testing whether adding joinpoints significantly improves the fit. 14
In this study, annual data were modeled with log-transformed percent outcomes using an uncorrelated error structure. A Grid Search algorithm was applied to identify models with 0–3 possible joinpoints, requiring at least 2 observations between the joinpoints and at each segment boundary. The model selection was based on permutation tests (4,499 permutations; overall significance level = 0.05). Age group and sex were included as by-variables, and APCs and AAPCs were estimated using parametric 95% confidence intervals (CIs). Pairwise, parallel trend comparisons were performed using the same permutation-based significance criteria.
Results
Trends in Walking, Obesity, and hyperTG According to Age and Sex

AAPC, average annual percent change; APC, annual percent change; CI, confidence interval; hyperTG, hypertriglyceridemia; N/A, not applicable. The * and bold text indicate values that are statistically significant at p < .05.
Walking practice, hypertriglyceridemia, and obesity in middle-aged adults according to sex

Trends in walking practice according to age and sex
Trends in hypertriglyceridemia prevalence according to by age and sex

Trends in obesity prevalence according to age and sex
Proportion of Individuals Who Engaged in Walking Practice and Experienced hyperTG and Obesity
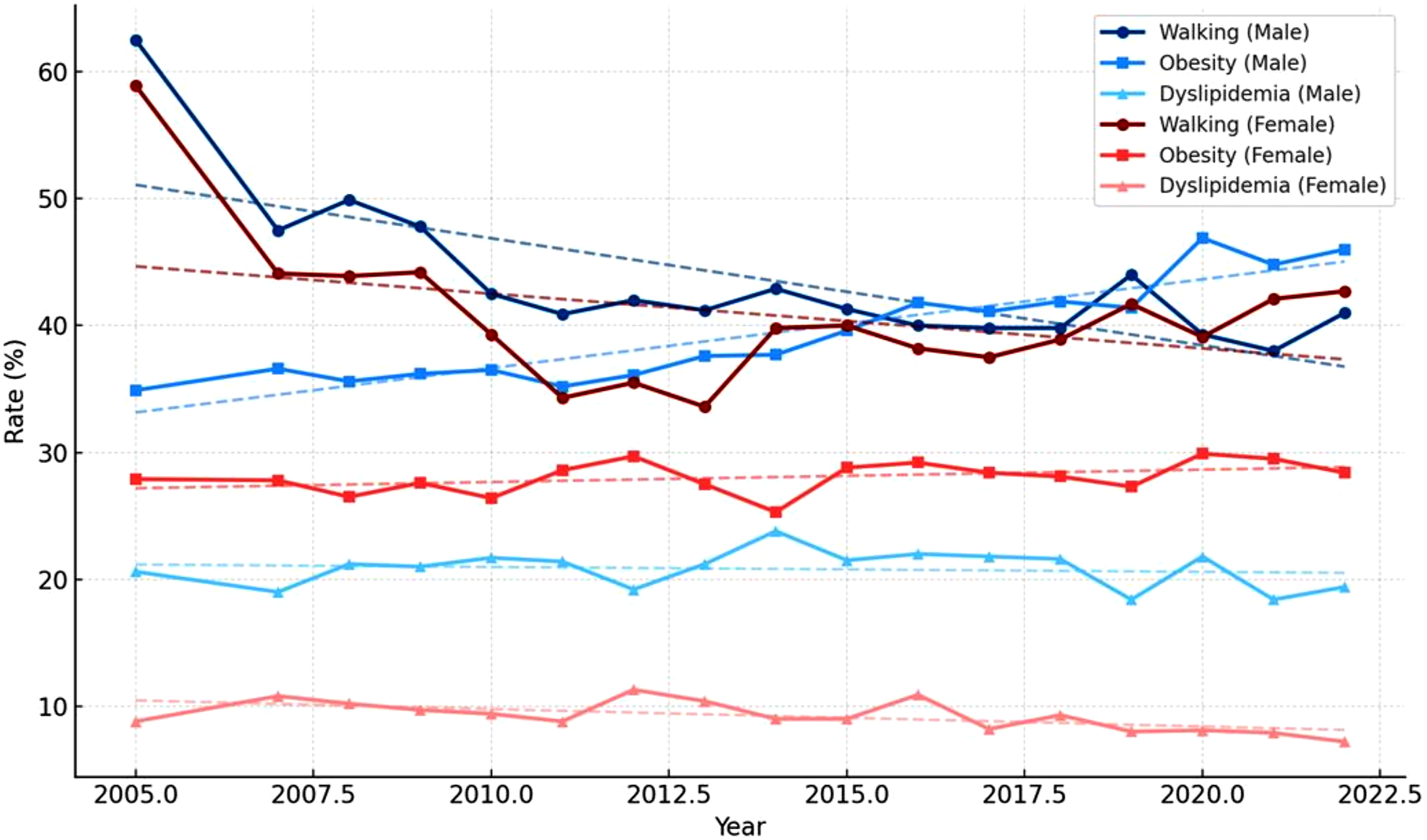
The proportion of men aged 40–69 years who engaged in walking practice declined, from 59.2% in 2005 to 32.6% in 2010, and subsequently fluctuated modestly, to a final value of 37.0% in 2023. The prevalence of obesity in men aged 40–69 years showed a sustained increasing trend over the same time period, rising from 41.1% in 2005 to a peak of 57.7% in 2021, with a slight decrease to 50.2% in 2023. HyperTG prevalence in men fluctuated over time, reaching its lowest level of 22.2% in 2012, peaking in 2020 at 34.2%, before declining again to 22.3% in 2023.
Among women aged 40–69 years, walking practice declined from 64.3% in 2005 to 30.6% in 2011, followed by a partial recovery to 42.1% in 2023. The prevalence of obesity in women aged 40–69 years was substantially lower than that in men and remained comparatively stable over the study period, with 29.0% in 2005, 22.3% in 2014, and a final value of 24.5% in 2023. HyperTG prevalence among women was consistently low throughout the study period, peaking at 14.4% in 2012 and declining to 5.4% in 2020, with a similar level (6.1%) observed in 2023 (Table 1 and Figure 1).
Trends in Walking Practice in Middle-Aged Adults
Age-stratified Joinpoint regression revealed distinct temporal patterns in walking practice between the sexes. Among individuals aged 40–49 years, the walking rates significantly declined in segment 1 (2005–2011 APC: -10.2%, 95% CI: -11.9 to -8.5), but non-significantly increased in segment 2 (2011–2014 APC: 6.4%, 95% CI: -9.4 to 25.1), and stabilized thereafter (2014–2023 APC: -0.01%, 95% CI: -1.3 to 1.2). The overall AAPC of -2.5% (95% CI: -5.1 to 0.1) was not significant. In the 50–59-year age group, the walking rates in men decreased in segment 1 (2005–2011 APC: -8.9%, 95% CI: -12.1 to -5.6), with an overall AAPC of -3.5% (95% CI: -5.0 to -2.0). In contrast, in the women of the same age group, the walking rates declined in segment 1 (2005–2012 APC: -9.2%, 95% CI: -11.7 to -6.6) and then significantly increased in segment 2 (2012–2023 APC: 3.2%, 95% CI: 1.6 to 4.8). Among individuals aged 60–69 years, the walking rates showed no significant change in men (AAPC: -2.5%, 95% CI: -5.1 to 0.03), whereas, in women, they declined significantly in segment 1 (2005–2012 APC: -7.3%, 95% CI: -10.4 to -4.8) and then increased significantly in segment 2 (2012–2023 APC: 3.5%, 95% CI: 2.0 to 5.1) (Table 1 and Figure 2).
Trends in hyperTG Prevalence in Middle-Aged Adults
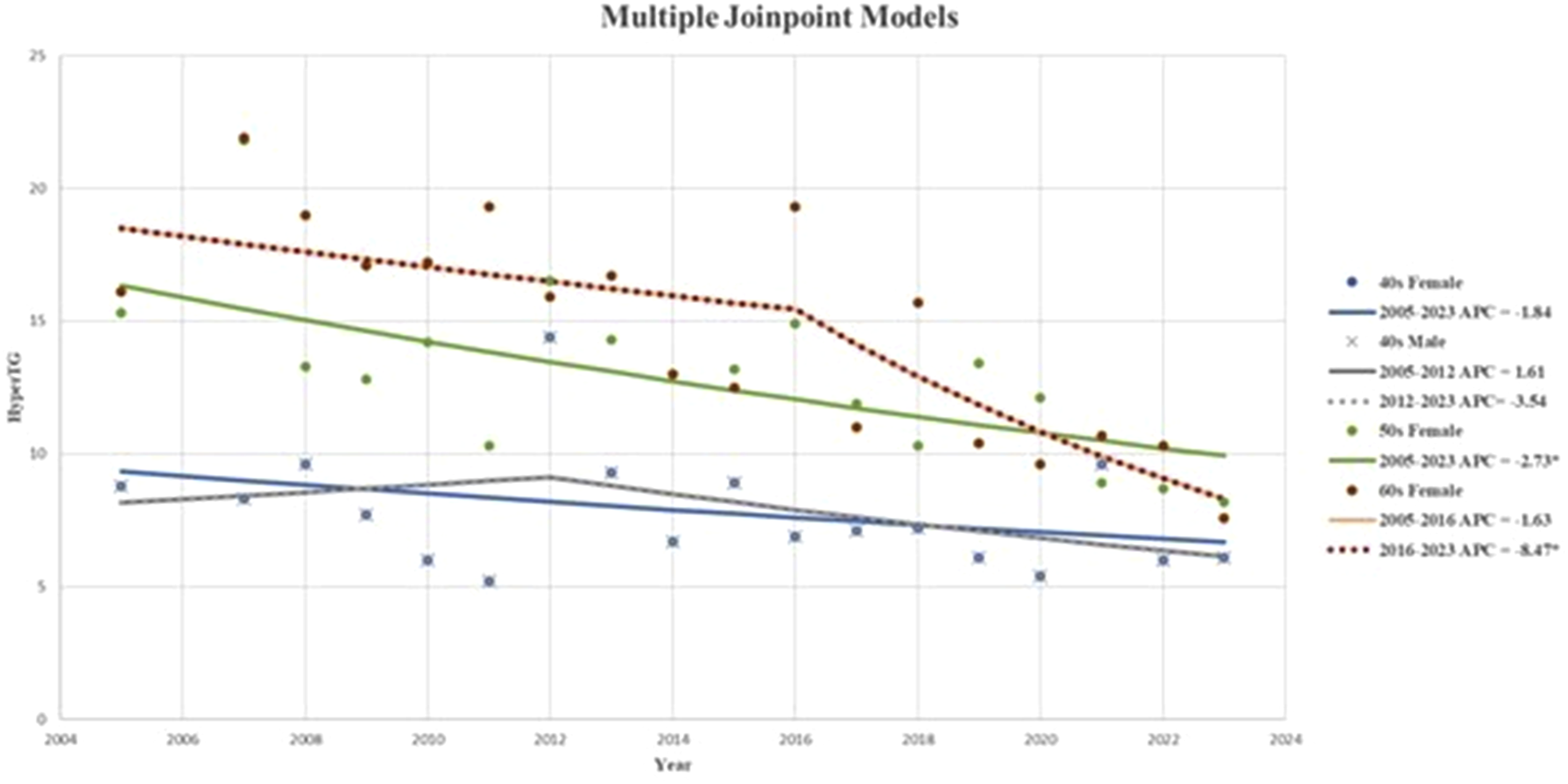
In the 40–49-year age group, hyperTG in men significantly increased in segment 1 (2005– 2020 APC: 1.5%, 95% CI: 0.2 to 2.8), followed by a non-significant decline in segment 2 (2020 –2023 APC: -10.8%. 95% CI: -24.0 to 4.6). but the overall AAPC of 0.6% was not significant (95% CI: -3.1 to 1.9).
Women aged 40–49 years showed no significant temporal changes over the study period (APC: -1.8%, 95% CI: -4.1 to 0.5). Among individuals aged 50–59 years, hyperTG prevalence declined significantly in the whole population from 2005 to 2023 (APC: -1.4%, 95% CI: -2.3 to -0.4). In the 60–69-year age group, hyperTG prevalence initially increased between 2005 and 2011 (APC: 2.4%, 95% CI: -3.3 to 8.6) but subsequently decreased significantly between 2011 and 2023 (APC: -4.1%, 95% CI: -6.1 to -2.1). The overall AAPC of -2.0% was not significant (95% CI: -4.2 to 0.2) (Table 1 and Figure 3).
Trends in Obesity in Middle-Aged Adults
Among individuals aged 40–49 years, obesity prevalence in men increased in segment 1 (2005–2023 APC: 1.7%, 95% CI: 1.1 to 2.3); no significant change was observed for women of the same age group in segment 1 (APC: -0.5%, 95% CI: -1.2 to 0.1), resulting in a significant sex difference (p < 0.001). In the 50–59-year age group, the obesity rates in men declined in segment 1 (2005–2012 APC: -1.7%, 95% CI: -4.8 to 1.5) but significantly increased in segment 2 (2012–2023 (APC: 2.4%, 95% CI: 1.1 to 3.7). However, AAPC of 0.8% was not significant (95% CI: -0.5 to 2.1).
In contrast, a consistent decline in obesity prevalence was observed between 2005 and 2023 in women of the same age group (APC: -1.9%, 95% CI: -2.6 to -1.2). Among individuals aged 60–69 years, obesity prevalence in men significantly increased in segment 1 (2005–2021 APC: 2.0%, 95% CI: 1.1 to 2.9) with no significant overall change thereafter (AAPC: 0.6%, 95% CI: -1.4 to 2.7), whereas women demonstrated a sustained decrease between 2005 and 2023 (APC: -1.5%, 95% CI: -2.1 to -0.8) (Table 1 and Figure 4).
Discussion
Using nationally representative data collected between 2005 and 2023, this study identified clear age- and sex-specific differences in the long-term trends of walking practice, hyperTG, and obesity among South Korean adults aged 40–69 years. The most notable finding was the improvement in walking practice and concurrent decline in obesity among middle-aged and older women, in contrast to persistently unfavorable trends, particularly the increasing prevalence of obesity, among middle-aged men. These results underscore the heterogeneous nature of walking practice and obesity throughout middle aged life and between the sexes.
Walking Practice: Early Decline Followed by Stabilization With Significant Sex Divergence
Walking practice patterns differed according to sex. Although the walking rates declined sharply among adults in their 40s during the early study period, a significant recovery was observed after 2012 among women aged 50–69 years but not among men of the same age group. Walking varies considerably across regions. According to the World Health Organization, approximately 27.5% of adults worldwide were insufficiently active in 2016, with physical inactivity that include walking being more prevalent among women than men. 16 Compared with these global estimates, 16 the walking rates observed in Korea from 2005 to 2023 (during the observation period, the range was between 28.3% and 67.6%) indicate relatively higher levels of engagement, particularly during the earlier years of the study period. 17 In the neighboring East Asian countries Japan and China, walking practice among adults has been reported to range between 40% and 50%, influenced by factors such as urban design, transportation patterns, and social norms.18-20 In the present study, men, particularly those in their 40s and 50s, exhibited an abrupt decline in walking in the early study period followed by a prolonged plateau. Similarly, women showed substantial early reductions; however, unlike men, women in their 50s and 60s demonstrated a significant rebound in walking practices post-2012.
South Korea established a comprehensive policy framework to promote walking as a key public health strategy between 2011 and 2012, which may be temporally aligned with the subsequent improvements in walking practice among women. 21 The Health Plan 2020 marked a shift toward prevention-centered care by prioritizing physical activity such as walking, whereas the establishment of the Korea Health Promotion Institute strengthened the national coordination of health promotion efforts. These initiatives were reinforced by pedestrian-focused legislation and the adoption of integrated community health programs that collectively embedded walkability into public health policies and local urban environments. 22 This policy initiative highlighted the need for targeted interventions in regions where individuals exhibited low walking practice levels, including improvements to the built environment and establishment of community-based walking promotion programs. 21 However, despite these initiatives, overall walking practice among women demonstrated a long-term declining or stagnant trend, consistent with global reports showing higher inactivity rates among women than among men. 11
HyperTG: Stability in Men Contrasted With Meaningful Change in Women
Trends in hyperTG prevalence revealed further sex- and age-related disparities. The increasing prevalence in hyperTG among men in their 40s before 2020 suggests a heightened vulnerability to adverse metabolic profiles during midlife.7,14
For women aged 60–69 years, the decline in hyperTG prevalence was substantial and statistically significant. Among women aged 60–69 years, the decline in hyperTG prevalence was statistically significant in this study. These findings are consistent with those of international studies, which have indicated that women are more likely than men to adopt preventive health behaviors, particularly after midlife transitions. 7 Although this pattern may be influenced by factors such as sex differences in health behaviors and risk awareness,7,12 the present study is limited in its ability to identify the underlying causes. The relatively static trajectory in men is consistent with regional epidemiological patterns across Asia, where a higher dyslipidemia burden has been reported in men than in women. 7 The relatively stable pattern of hyperlipidemia observed in South Korean men aged 40–49 years suggests the potential need for targeted lipid management strategies to help reduce cardiometabolic risk in this population. Several large cohort studies conducted over the past three decades have suggested that TG levels may have different clinical implications in women and men.1,5-7,9,12 Early evidence from case-control and prospective cohort studies consistently identified TG as an independent cardiovascular risk factor, even after accounting for total cholesterol or high-density lipoprotein cholesterol, with some studies indicating a stronger predictive value in women than in men. 1 Collectively, these findings underscore the need for sex-specific TG monitoring, particularly in women, in whom TG elevation may signal a disproportionately higher cardiovascular risk. The trends observed in this study may indicate that population-level lipid control efforts over the past decade have been associated with relatively greater improvements in women than in men.
Obesity: Progressive Increase in Men Versus Declining Trend in Women
Obesity trends demonstrated the clearest sex difference. Among men, obesity prevalence consistently and significantly increased over the study period across all age groups, with the steepest increase occurring after the mid-2010s. This finding is consistent with previous studies reporting that obesity rates among Asian men are increasing at the fastest pace globally, despite the implementation of public health measures. 16
In contrast, decreased obesity rates were observed in women across all three age groups, with significant long-term declines in those aged 50–69 years. These trends correspond with the results of previous Korean studies that documented greater adoption of weight-control behaviors among middle-aged women, shaped by strong sociocultural norms emphasizing thinness and body management. 23 Additionally, the later-life improvements in walking practice observed among women may have had positive effects on their weight and metabolic profile. 23 Collectively the simultaneous increase in obesity and hyperTG among men, in contrast to the decline in hyperTG and obesity among women, highlights the emergence of a gap between the sexes. The walking behaviors of women indicate successful risk reduction over the study period, whereas men appear to be moving in the opposite direction, with a persistent increase in obesity and limited improvement in TG. 24 According to recent studies, the prevalence of overweight and obesity has increased globally across all countries, with no nation successfully reversing this trend, and the rise in obesity has been more pronounced in men than in women. 25
Notably, improvements in walking practice were not consistently associated with favorable changes in metabolic indicators across all groups, suggesting that walking alone may be insufficient to address the broader determinants of metabolic health. Accordingly, more comprehensive approaches that consider factors such as diet, alcohol consumption, occupational activity, and obesity may be warranted.
Limitations
This study has some limitations that should be considered. First, walking practice was assessed using self-reported questionnaire data, which may be subject to recall and social desirability biases. Second, although this study examined long-term trends using repeated nationally representative cross-sectional data, causal relationships among walking practice, hyperTG, and obesity could not be established. Individual-level longitudinal changes in lifestyle behaviors and metabolic outcomes were not captured, limiting the ability to assess within-person trajectories over time. Third, important lifestyle and clinical factors that influence TG levels and obesity, including dietary intake, alcohol consumption, medication use, and menopausal status, were not explicitly adjusted for in the trend analyses. Changes in these factors over time may have contributed to the observed trends, particularly the decline in hyperTG prevalence among older adults. Finally, although age standardization was applied, residual confounding factors related to socioeconomic status, occupational physical activity, and regional disparities may persist.
Conclusions
This study demonstrates pronounced age- and sex-specific divergences in the long-term trends of walking practice, hyperTG, and obesity among South Korean adults. Although walking practice was improved mainly in older women, obesity continued to worsen in middle-aged men. These findings suggest that men aged 40–69 years may benefit from regular monitoring of metabolic indicators, including triglyceride levels, along with lifestyle counseling focused on walking and sustained, individualized interventions for obesity management. Moreover, sustained environmental and community-based strategies—such as improving neighborhood walkability, implementing workplace programs, and delivering sex-specific health messaging—may play an important role in promoting walking and reducing obesity risk.
Footnotes
Ethical Considerations
The KNHANES was approved by the Research Ethics Review Committee of the Korea Disease Control and Prevention Agency. This secondary data analysis was exempted from review by the Institutional Review Board of Chungnam-National University (No. 202408-SB-114-01).
Consent to Participate
This study was a secondary analysis of data obtained from the KNHANES, a publicly available dataset. Written informed consent was obtained from all participants by the Korea Disease Control and Prevention Agency at the time of the original data collection. No additional informed consent was required for the present study.
Author Contribution
YS supervised the entire study process and critically revised the manuscript. YS, HS, and NK conceived the idea, performed the analysis of the included studies, and drafted the manuscript. HS selected and searched for relevant studies. YS and NK analyzed the data and interpreted the results. NK illustrated the graphs. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT)(RS-2026-25476867) and Chungnam National University.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.