
Abstract
Introduction
Infection Prevention and Control (IPC) is a science-based, practical approach that protects patients and healthcare workers by reducing hospital-associated infections (HAIs) and tackling antimicrobial resistance (AMR). The study aims to assess the baseline status of IPC in a provincial hospital in Nepal to help propose an action plan for implementation and mitigate the burgeoning issue of AMR.
Method
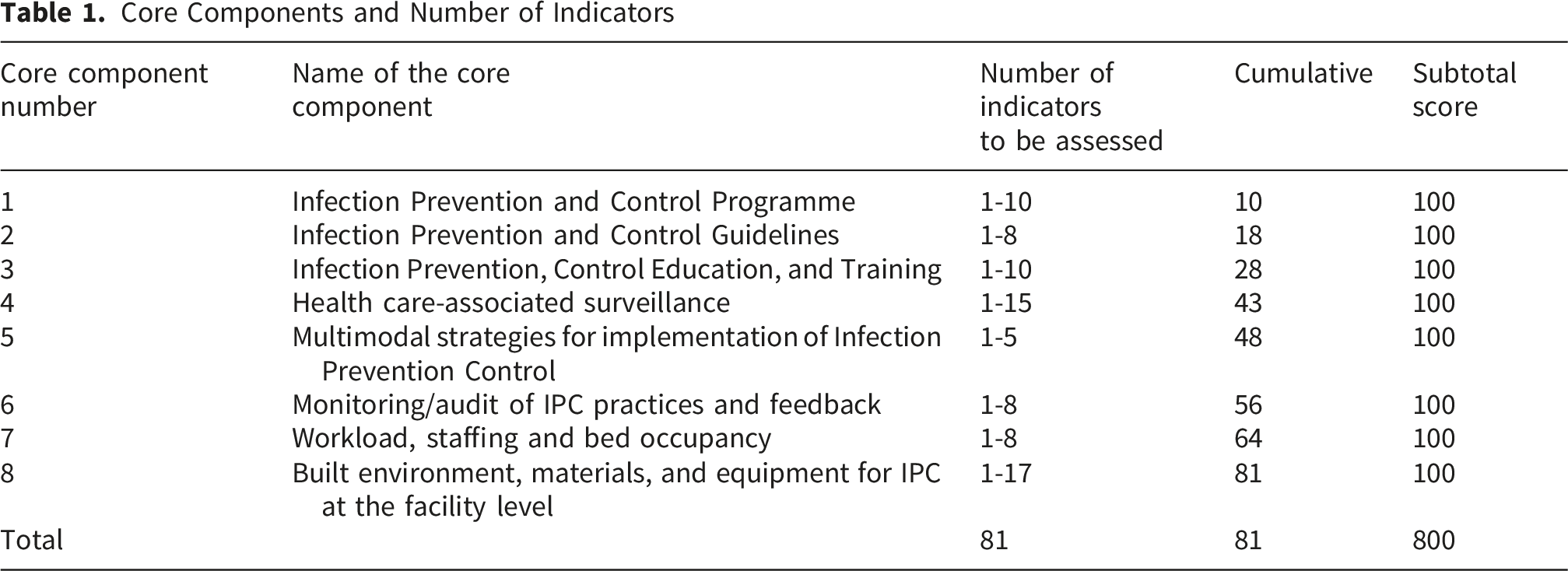
A cross-sectional study was conducted as a quality improvement project at one of the provincial hospital of Nepal using the structured World Health Organization (WHO) Infection Prevention and Control Assessment Framework (IPCAF) tool to perform a baseline assessment. The IPCAF tool’s 8 core components and 81 indicators were assessed to determine the hospital's IPC status and to propose an action plan to facilitate IPC-related activities. After receiving the data, it was entered into MS Excel 2013, analyzed for the indicator scores, and visualized using R Version 4.5.2.
Result
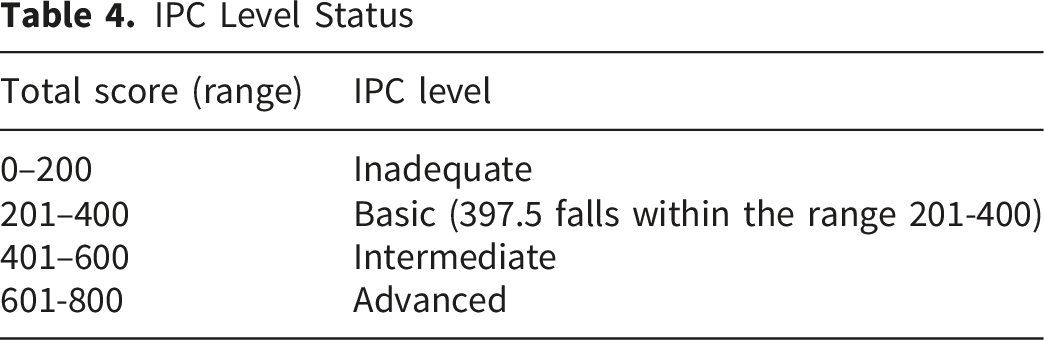
The total score for the eight basic IPC indicators was 397.5/800, indicating that the facility operated at a “basic” IPC level (score range: 201-400). The highest score was in Monitoring/audits of IPC practices and feedback (77.5), indicating relative strength. Moderate scores were seen in IPC programme (60) and IPC guidelines (62.5), followed by HAI surveillance (55) and IPC education and training (50). Three indicators scored below 50, indicating poor adherence to the international guideline (IPCAF) and critical gaps that underscore the need for urgent attention.
Conclusion
This first IPC assessment at one of the provincial hospital revealed a “Basic” IPC status, highlighting critical gaps in areas like Multimodal strategies, workload, staffing and bed occupancy, resources, materials, and equipment for IPC, and IPC education and training. Despite a few strengths, the findings call for an urgent, time-limited, and team-based approach with effective implementation and ongoing monitoring of the IPC action plan.
Keywords
1. What We Already Know
• Infection Prevention and Control (IPC) is significant in protecting patients and healthcare workers, ensuring safer medical environments. • Empowering IPC practices aims to mitigate hospital-associated infections and address the challenge of Antimicrobial Resistance (AMR).
2. What This Article Adds
• The study aims to assess the baseline status of IPC within a provincial hospital of Nepal to help propose an action plan for implementation and help mitigate the burgeoning issue of AMR. • This first IPC assessment, conducted as a quality improvement project, revealed a “Basic” IPC status, highlighting critical gaps in areas like Multimodal strategies, workload, staffing and bed occupancy, resources, materials, and equipment for IPC, and IPC education and training.
Introduction
Infection Prevention and Control (IPC) is a scientifically evidence-based and practical approach aimed at minimizing harm in healthcare settings. 1 IPC plays a vital role in safeguarding both patients and healthcare workers (HCWs), ensuring safer medical environments, as it is a fundamental strategy for combating hospital-associated infections (HAIs) and addressing antimicrobial resistance (AMR).1,2
HAIs are a major concern in medical facilities, causing financial burden and negatively impacting patients’ well-being. 3 The direct medical economic burden is extraordinarily high among the HAIs and within the HAIs-AMR inpatients. 3 The European Center for Disease Prevention and Control reports an estimated 501 disability adjusted life years lost per 100,000 population due to HAIs, with more than 90,000 deaths per year. 4 Low and middle income countries (LMICs) face even greater burden (15.5% prevalence), as highlighted by Nepal’s 2022 rate of 11% as per a health facility survey study. 5
According to Nepal’s National Action Plan (NAP) on AMR (2024-2028) strategies, priority III emphasizes reducing infection rates through robust IPC measures across the human, animal, and community health sectors. 6 Similarly, IPC also supports multiple Sustainable Development Goals (SDGs), particularly SDG 3 (Good Health and Well-being), targets 3.3 and 3.8, by helping to end epidemics and strengthen health preparedness. Similarly, it also contributes to SDG 6 (Clean Water and Sanitation), targets 6.1 and 6.2, through WASH in healthcare; to SDG 8 (Decent Work), target 8.8, by protecting healthcare workers; and to SDG 12 (Responsible Consumption), target 12.4, through safe medical waste management.3,6,7 A comparative study of IPC program assessment tools findings underscores that IPC program evaluation (IPCPE) and Infection Prevention and Control Assessment Framework (IPCAF) revealed strengths in their effectiveness, their relevance to the assess goals, and their capacity to highlight necessary enhancements. 8 The practical manual further provides guidance for healthcare facilities to implement IPC (8 core components) programs in line with the World Health Organization (WHO) guidelines, aiming to enhance the quality, safety, and health outcomes of healthcare service delivery. 8 International literature also highlights the importance of IPC in integration with Antimicrobial stewardship (AMS) programs.9,10 A study from China analyzing the implementation of the AMS program and its barriers noted that the multidisciplinary teams within the AMS included the IPC personnel who are responsible for preventing HAIs, along with the judicious use of antimicrobials and infection control. 9 Another study from Italy identifies the assessment of government frameworks for AMS and IPC, and identifies several targeted interventions. 10 Both of these studies focuse on the integrative role of IPC and AMS, assessment of government models in its feasibility and execution, and underscore the necessity to focus on training programs and multi-collaborative partners.9,10
Additionally, gaps in IPC implementation and core components across income levels hinder progress. Therefore, strengthening sustainable IPC programs is essential to reducing outbreak risks, enhancing global health security, and ensuring patient and health worker safety through effective IPC adherence and assessment measures. 11 The lead author (N.P.) was involved in a trainer of trainer’s (ToT) program and training to HCWs program conducted by the Health Directorate, Ministry of Health, Bagmati Province, Nepal, to enhance the awareness regarding the containment of AMR, where the training session was mostly focused on strengthening the NAP-AMR strategic priorities. As such, the training session also focused on strengthening IPC standards and the essence of assessment within the hospital facility. Drawing on insights from the training program, this study aimed to assess baseline IPC capacity to inform intervention, thereby facilitating strategic priority III (reducing the incidence of infection), 6 using a systematic tool developed by WHO as a pilot project for the baseline assessment of IPC indicators. As such, this study is conducted as a quality improvement project to assess the baseline status of the IPC core component at a provincial hospital in Nepal to propose a target action plan for implementation and help mitigate the burgeoning issue of AMR in hospital settings.
Methods
This study was carried out at Hetauda hospital, Madan Bhandari Academy of Health Sciences, Bagmati Province, Nepal, during the month of December (7-8th), 2025, using a cross-sectional facility-based IPC assessment design. While the term “cross-sectional” reflects the single-time-point nature of the data collection, the design is more accurately described as a facility-level audit or assessment using a structured WHO tool, which is the recommended approach for baseline IPC evaluation at the institutional level. Following the quality improvement nature of the study, it is reported as per the SQUIRE 2.0 (Standards for QUality Improvement Reporting Excellence guideline (Supplementary File 1). 12
Study Site and IPC Importance
Hetauda Hospital, Madan Bhandari Academy of Health Sciences, is a secondary class B hospital providing services to more than 800 patients on a daily basis with almost 300 beds and departments ranging from internal medicine, orthopedics, pediatrics, surgery, obstetrics and gynecology, ear, nose, and throat, neurosurgery, and dermatology, with each department having its own inpatient and outpatient section. Secondary hospital (B) means a hospital that provides services as determined by the minimum service standard (MSS) in the context of the Ministry of Health and Food Safety, Nepal, and generally has 100 to 300 beds. The hospital is located almost 76-83 kilometers south of Kathmandu, the capital city of Nepal, and with the city ‘Hetauda’ being the capital city of the province, it has further amassed a massive patient population through the nearby districts and cities of both the urban and rural settings, with a myriad population enrolled in the National Health Insurance Program. The hospital also has its own laboratory, microbiological and pathology department, along with a dedicated pharmacy service. With the initiation of MSS in the context of Nepal to prioritize the growth of hospitals in each component related to clinical delivery, IPC also plays a key part in MSS for hospital safety and its quality, and prevention of HAIs.13-15 Within tertiary care, IPC concepts are included in Clinical services (Section II), such as inpatient care (2.6.14), maternity delivery services (2.7.1.10), and maternity inpatient care (2.7.2.12). Support services (Section III), such as CSSD, waste management, and safety, enhance overall infection control.13,16 In case of secondary class B hospitals like our study site, the concept of IPC is integrated within clinical services (inpatient and outpatient department), area of immunization and growth monitoring clinic, family planning clinic, maternity services to surgery areas to each department, 14 as such, this study also aims to fulfil the gaps and help strengthen the MSS criteria regarding IPC context within the hospital.
Study Tool
For the baseline IPC assessment, the IPCAF tool was used. The proposition of five steps by WHO in the effective implementation of IPC programme within hospital facilities also involves baseline assessment (Step 2), and assessing the impact following an action plan by using a structured tool, IPCAF (Figure 1).
17
WHO five steps for the implementation of infection prevention and control facility programme (Abbreviation: IPC – Infection Prevention and Control; WHO: World Health Organization; IPCAF: Infection Prevention and Control Assessment Framework)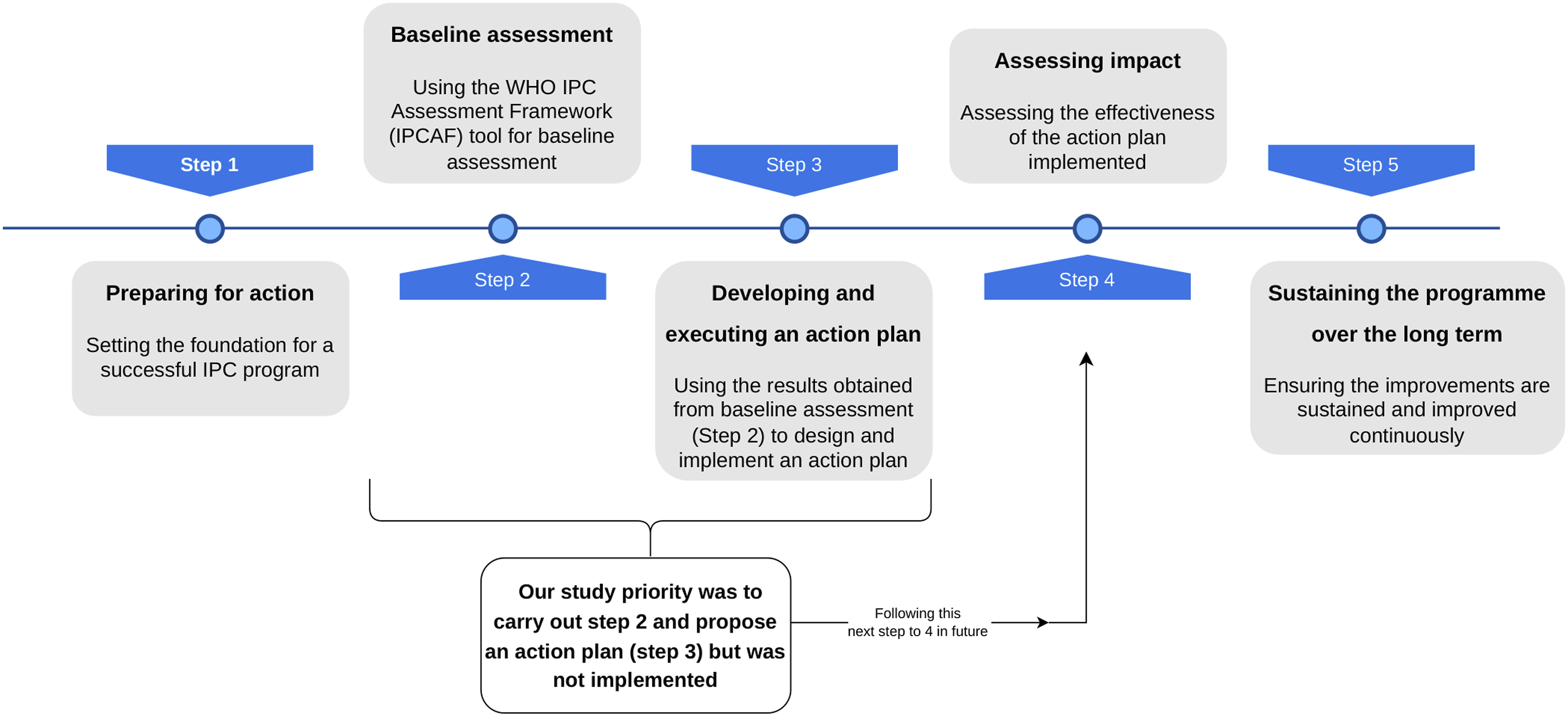
Core Components and Number of Indicators
Data Collection Process
The study was conducted at Hetauda hospital, Madan Bhandari Academy of Health Sciences, Bagmati Province, Nepal during the month of December 2025, where the members of the IPC Committee were purposively selected in accordance with WHO IPCAF guidance on “who should complete and use IPCAF?”, which specifies tool should be completed by individuals with direct knowledge and responsibility for IPC activities, such that the inclusion criteria were: 1) current member of hospital IPC committee and 2) direct involvement in IPC-related decision-making or implementation. This ensured that the data collected were relevant and comprehensive. Participants included the medical director, hospital administrator, nursing in-charge, consultant surgeon, consultant anesthesiologist, laboratory in-charge, and waste management personnel. Prior to data collection, formal permission was obtained during a Drug and Therapeutic Committee (DTC) meeting (Decision number 4, point number 3: IPC). The lead author facilitated the meeting. During this meeting, the IPCAF tool’s purpose, process, and global applicability were explained to committee members. The IPCAF was administered as a facilitated, consensus-based group assessment in accordance with WHO guidance following the sections “Who should complete and use the IPCAF?” and “How does it work?” as outlined in the WHO IPC Assessment Framework at the facility level. 17 This was supplemented by in-depth discussion with each committee member to clarify how the tool indicator aligns with actual practices and to gather accurate information about the facility’s IPC status. Orientation and explanation sessions were conducted with each IPC committee member prior to data entry to ensure a clear understanding of the core component indicators. Data collection in the IPCAF tool by the participants was checked for any responses left behind and documented. If any discrepancies were observed, they were checked again with the medical director and the IPC in charge.
Data Synthesis
Scores, IPC Assigned Level and the Meaning of Those Levels
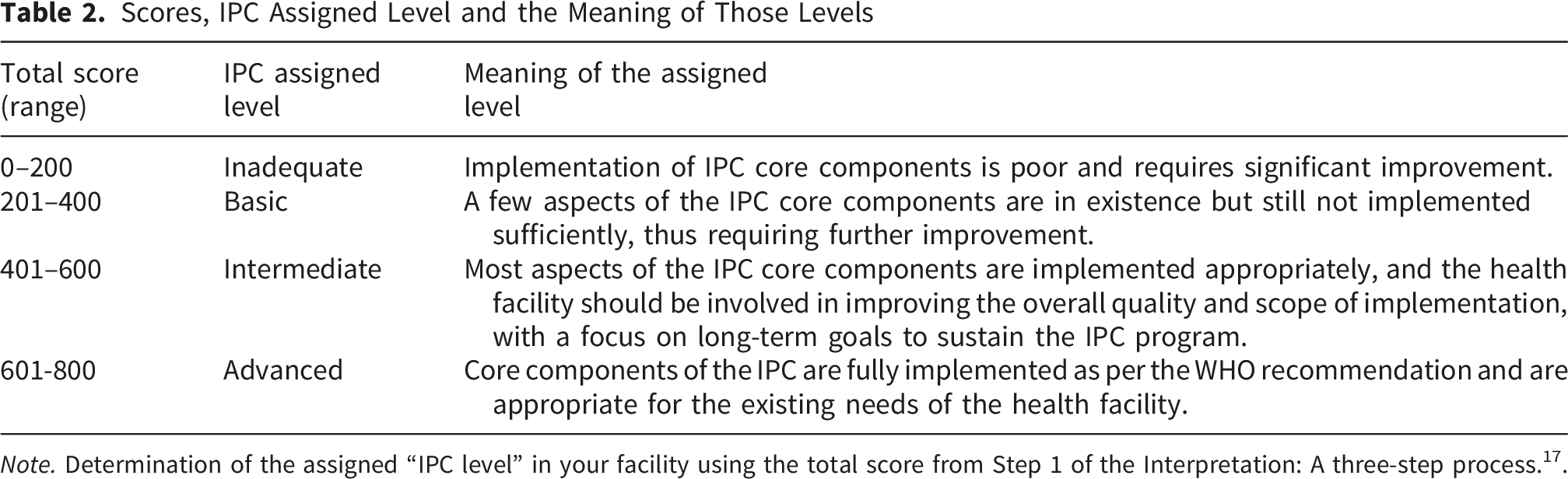
Note. Determination of the assigned “IPC level” in your facility using the total score from Step 1 of the Interpretation: A three-step process. 17 .
Result
Interpretation: A Three-step Process
Step 1. Add up Your Points: Finding out the Total Score
Scores of Eight Core Components and Status of IPC
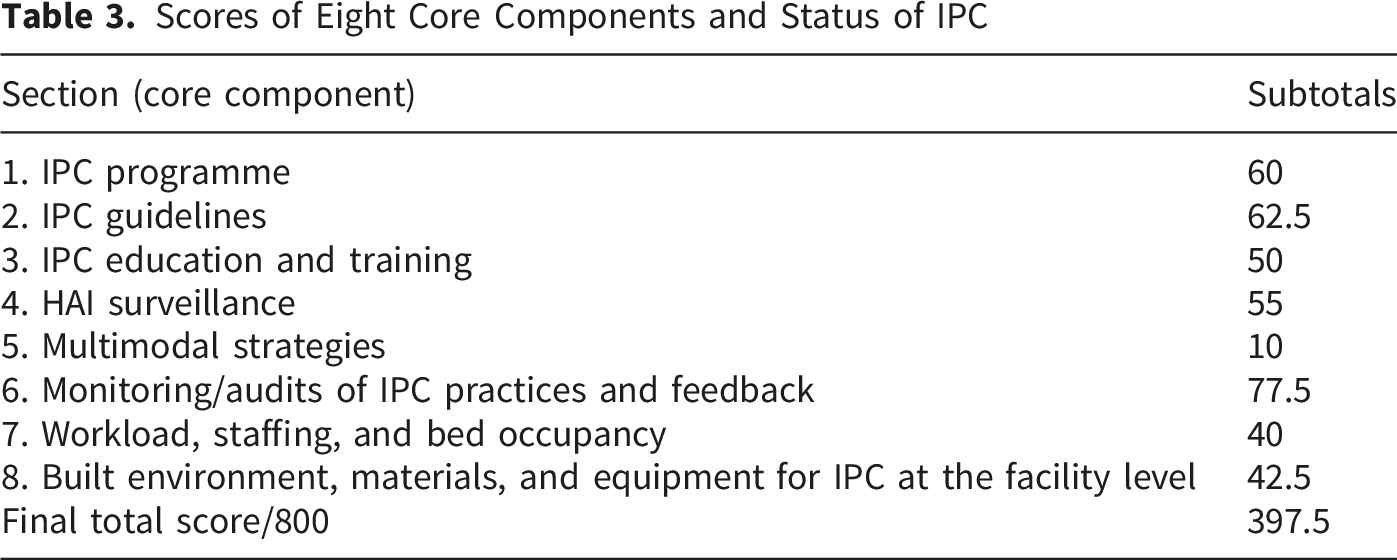
A score of 397.5 falls within the range of 201-400, thus depicting a “basic” level status of IPC of the hospital. These scores of 8 different indicators help in executing the “review the framework results and develop an action plan” mentioned within the “Interpretation: A three-step process section”. 17 This helps in fulfilling the goals of the 5 steps involved in the implementation of IPC facility programs.
The highest score was achieved in Monitoring/Audit of IPC Practices and Feedback (77.5/100), and the lowest in Multimodal Strategies (10/100), indicating important gaps in integrated strategies. Multimodal strategies core component 5 received low scores as the majority of the elements were not included within the strategic model, including low to moderate education and training, monitoring and feedback, and with no inclusion of elements regarding communication and reminders, safety climate, and culture change. The scores for five components including Monitoring/audits of IPC practices and feedback (77.5/100), IPC programmes (60/100), IPC guidelines (62.5/100), HAI surveillance (55/100) and IPC education and training (50/100) were found to be equal and above mid-value, while three components were found to be below mid-value score of 50/100 (Figure 2) indicating that the current infrastructure requires greater operationalization. The scores for each core component are as depicted in Supplementary File 2. Score-wise bar diagram of 8 different core components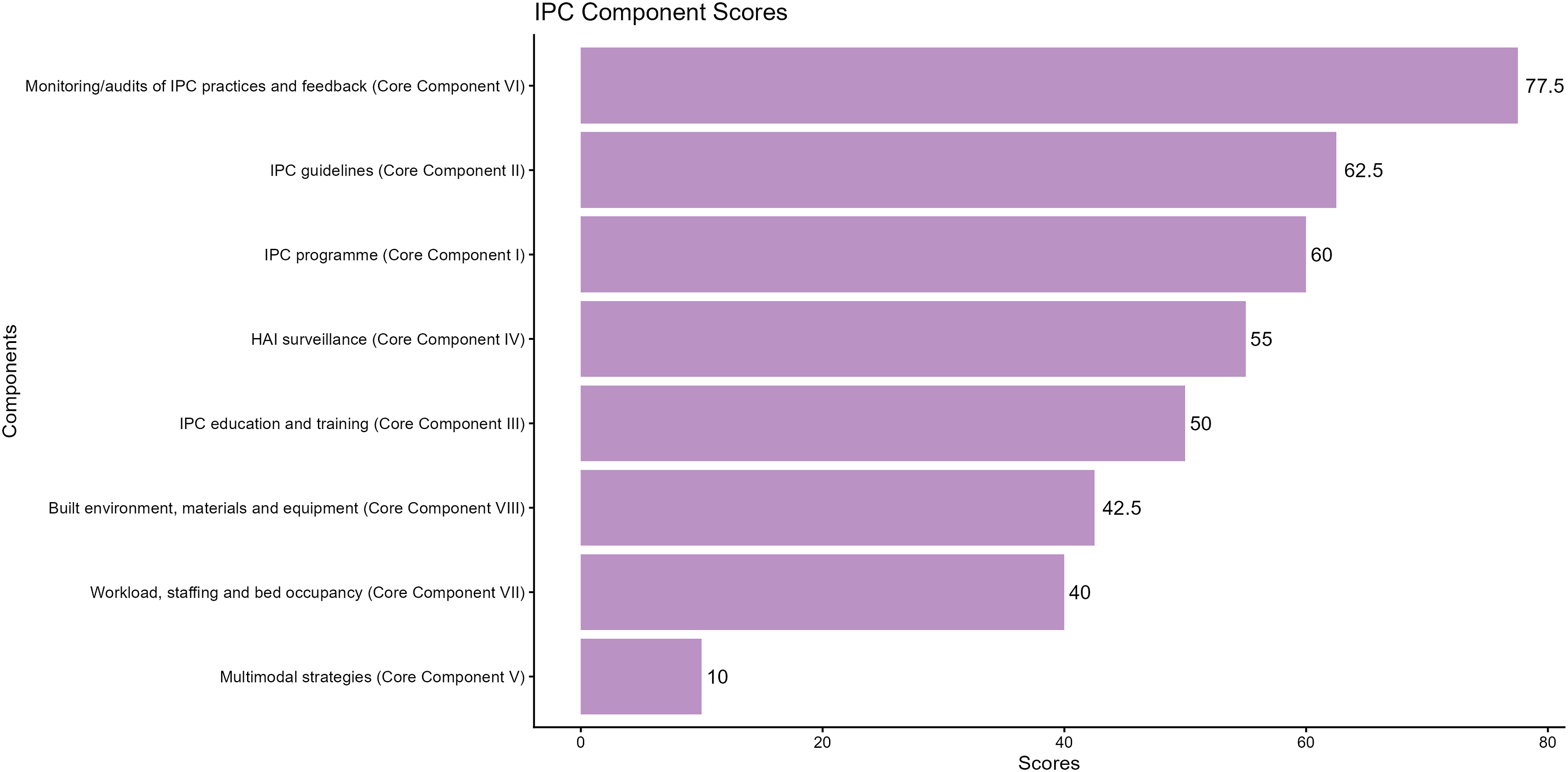
Although the WHO IPCAF tool is not divided into organizational and structural components, it is a mix of both. Within IPC-related research, they are commonly grouped as organizational, where the six core components (I to VI) provide information on governance, leadership, policies, and overall institutional practices, whereas the structural components (VII to VIII) address infrastructure, manpower, facility capacities, and the environment. An analysis of both the organizational and structural components showed that the organizational components had a higher mean score (52.5), with substantial variability across component scores. The interquartile range, as shown in the box plot (Figure 3), indicates moderate dispersion, suggesting inconsistency across organizational components. In contrast, the structural components further revealed a lower average score (41.2), as both component scores were similar, the spreading was minimal, with a narrow distribution showing infrastructural and resource gaps in IPC implementation. Boxplot comparison of organization and structural infection prevention and control scores [Abbreviation: IPCAF: Infection Prevention and Control Assessment Framework]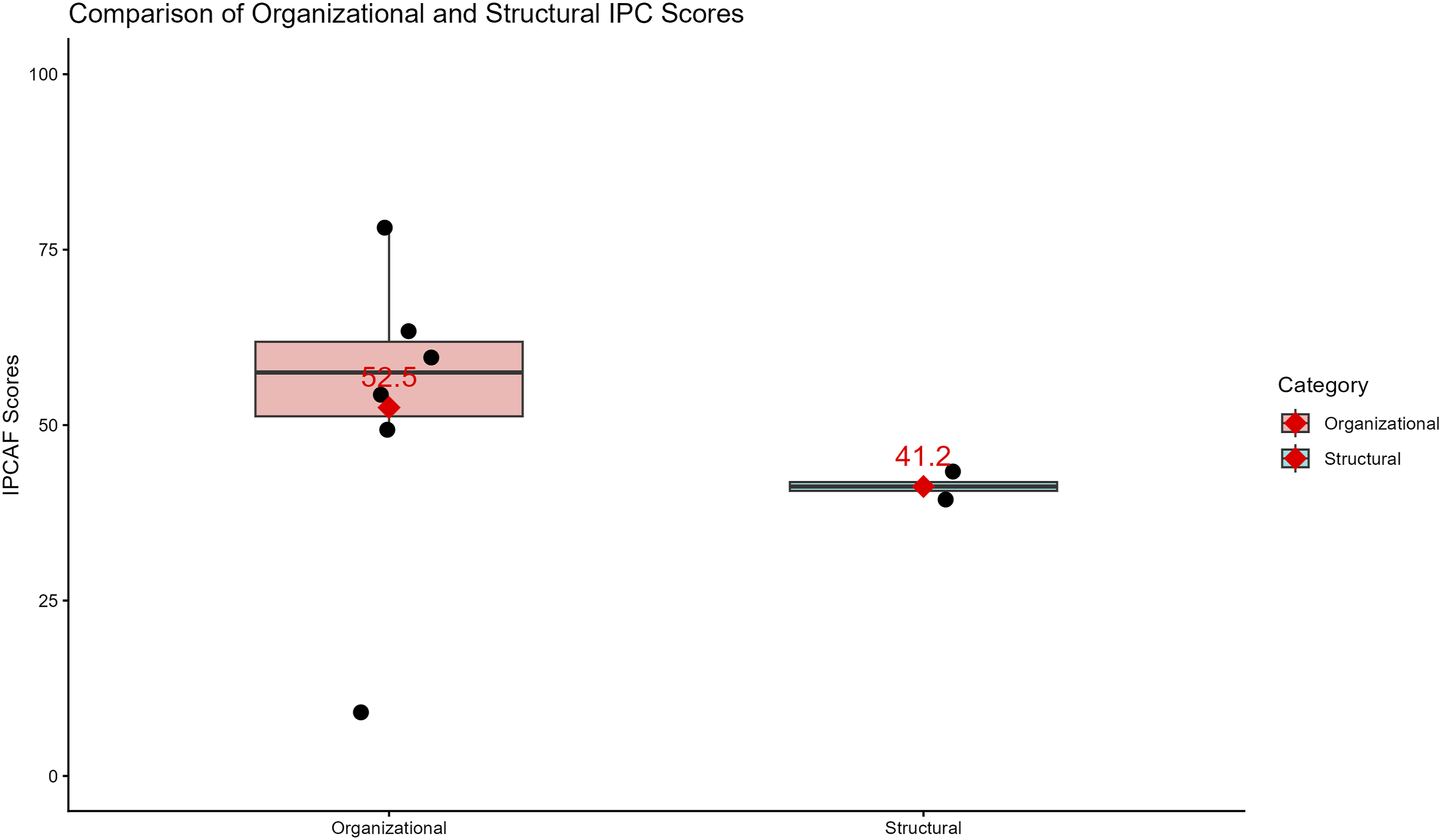
The lack of adherence to structural components may directly affect surveillance and multimodal strategies; hence, an action plan that focuses on each component is imperative to facilitate IPC-related activities within the hospital.
Step 2. Determine the Assigned “IPC Level” in Your Facility Using the Total Score From Step 1: IPC Level Facility
IPC Level Status
While the interpretation of IPC category status is divided into 4 categories, we can also adapt these WHO thresholds for an individual’s component proportionally. As such, for each component score out of 100, the interpretation would be as follows: Inadequate (0 – 25), Basic (25.1 – 50), Intermediate (50.1 -75), and Advanced (75.1-100). The radar chart prepared (Figure 4) to visualize the facility’s core component scores in response to WHO thresholds shows an irregular shape with an inward collapse in the multimodal strategies, moderate structural constraints, and uneven implementation, highlighting heterogeneous IPC capacity across the facility. Within Figure 4, the farther the blue polygon extends towards the outer edge, the better the score is for the individual component; as such, it highlights the multimodal strategies requiring the greatest priority. Radar chart providing a visual summary of the facility’s performance across the 8 WHO IPCAF core components [Note: In this figure, each spoke (axis) represents one WHO IPCAF core component. The concentric rings represent score levels: 0: Very poor, 25: inadequate, 50: basic, 75: intermediate, 100: advanced; The blue shaded area represents the facility’s performance profile.]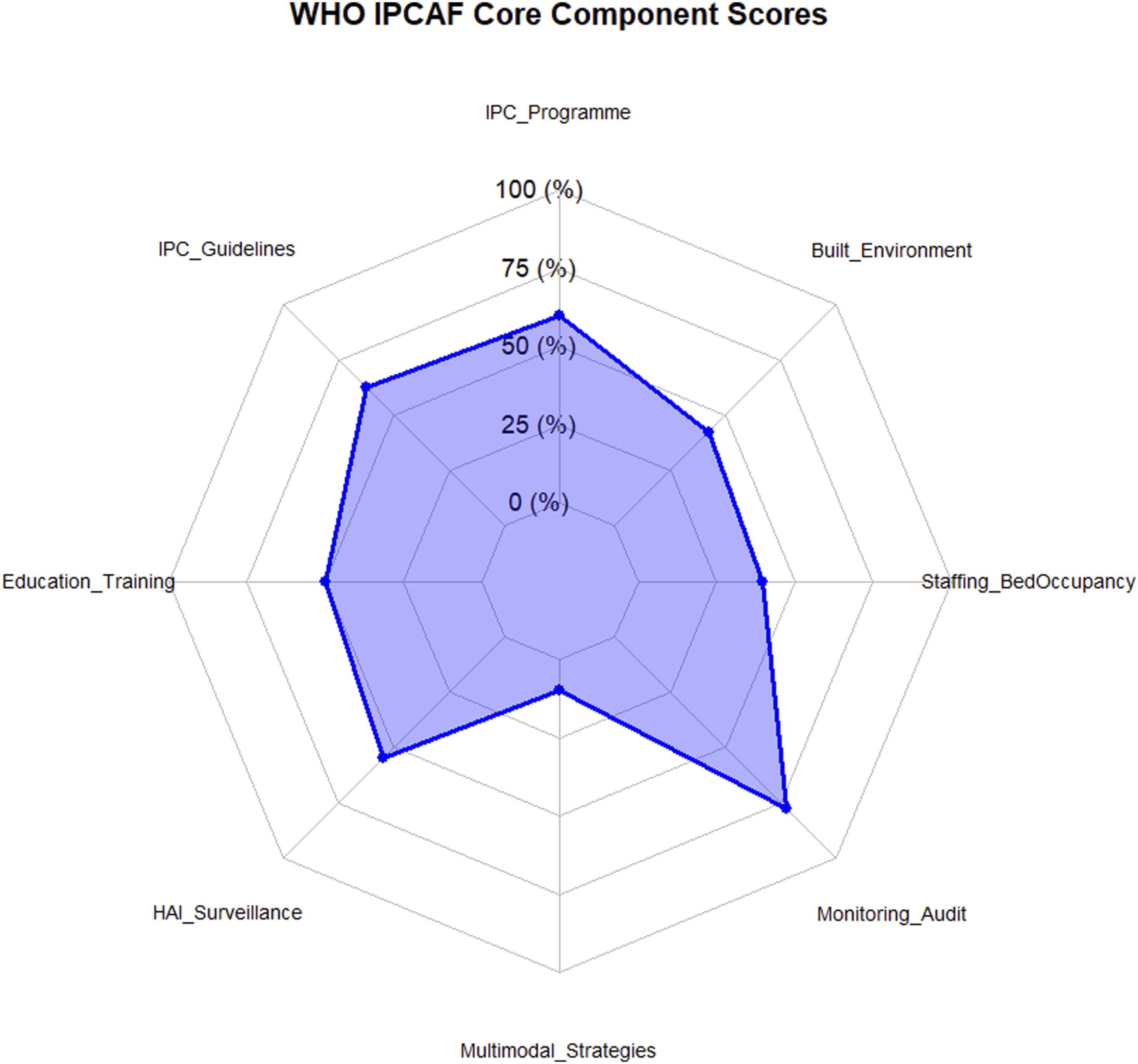
Step 3. Review the Framework Results and Develop an Action Plan: Proposition of Action Plan
Poor performance in core components “Built environment, materials and equipment for IPC at the facility level”, “Workload, staffing and bed occupancy,” and “Multimodal strategies” discloses significant areas for improvement. These results highlight the importance of targeted interventions to enhance IPC capacity and progress toward a higher IPC level. Following the scores, we have proposed an action plan (Figure 5). Proposed Infection Prevention and Control (IPC) Action Plan following the Interpretation: A three-step process of IPCAF [(Abbreviation: CC: Core component; IPC – Infection Prevention and Control; WHO: World Health Organization; IPCAF: Infection Prevention and Control Assessment Framework; HAI: Hospital Acquired Infections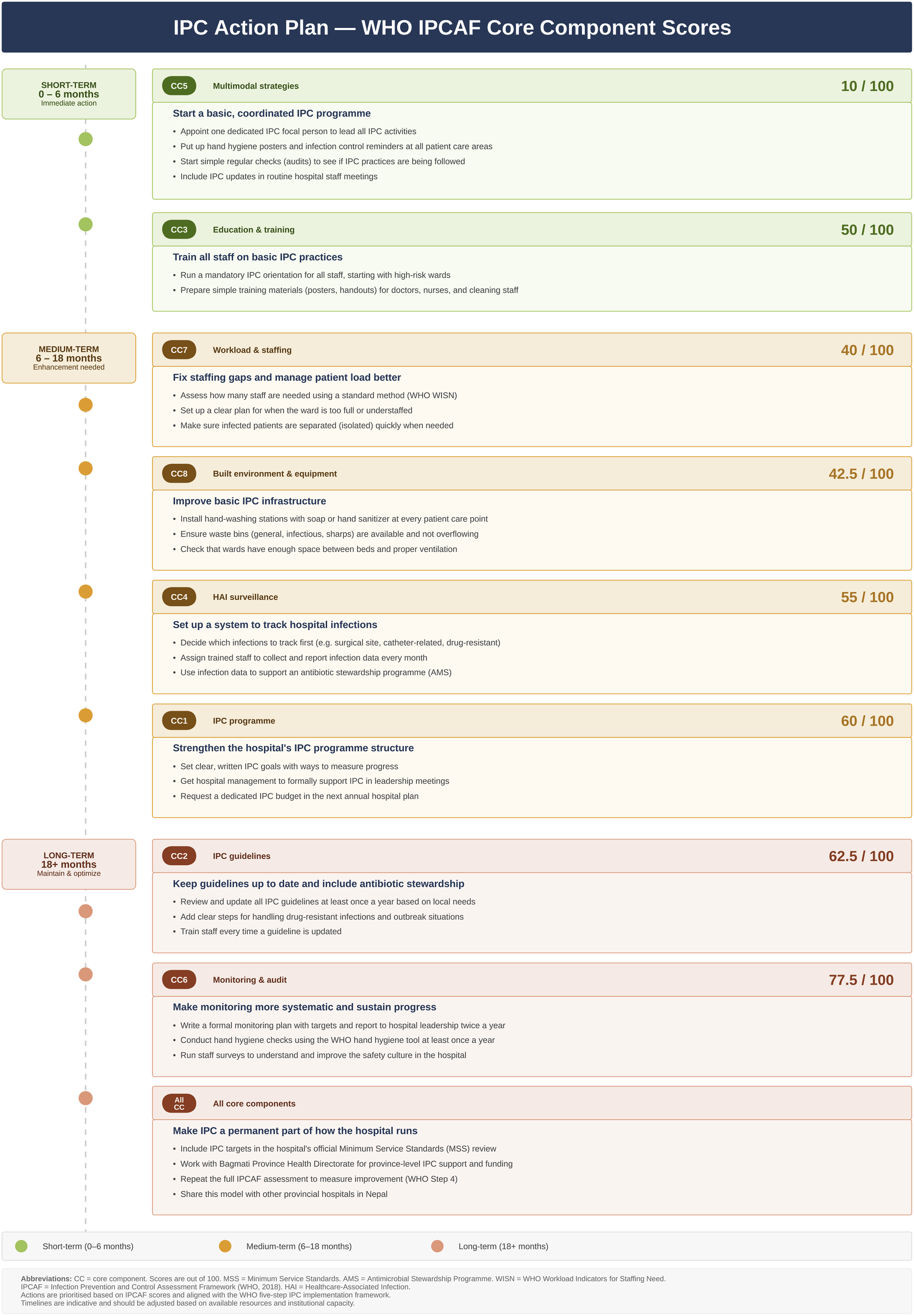
We have divided the action into three categories i.e., core components requiring immediate action (short term 0-6 months), components requiring enhancement (medium term 6-18 months) and components that needs to be maintained and optimized (long term 18+ months), where core components 5 (multimodal strategies) and 3 (education and training) are within our immediate action plan as these were poorly adherent to IPCAF.
Discussion
This study is uniqueas it marks the first IPC-related assessment study conducted at a provincial hospital in Bagmati Province, Nepal. This study acts as a quality improvement project, helping in assessing the IPC status, and will assist in building the action plan (Figure 5) for the hospital to increase the IPC-related impact in the coming days.
The gaps in IPC activities within a country represent its true ability to meet the International Health Regulations, respond to infectious disease outbreaks, and combat AMR, thus reflecting the hindrance in achieving United Nations SDGs. 4 Review studies conducted to analyze the status of IPC within LMICs revealed varying degrees of IPC program implementation, also with several gaps acting as a barrier for its proper implementation. 18
Core Components 1: Infection Prevention and Control (IPC) Programme
Effective IPC programmes are crucial in order to ascertain patient safety and encourage public health. 19 It is imperative to develop multidisciplinary team coordination within the IPC program and the committee to improve the quality of care and mitigate infection risks.19,20 In addition, the IPC programs must be tailored with clearly defined objectives, functions, and responsibilities based on local epidemiology and priorities, and risk assessments for the prevention of HAI and the spread of AMR. 21 The Guideline Development Group (GDG) recommends a minimum ratio of one full-time or equivalent infection preventionist per 250 beds in every acute care facility. 21 However, a full-time, dedicated team-based approach is lacking in this IPC setting. In addition, no specific budget has been allocated for this program, and demonstrable support for IPC indicators has not been properly conducted within the facility. This underscores the need for a dedicated full-time IPC professional with a separate budget or remuneration that could link the IPC-related issues to the team members.
Core Components 2: Infection Prevention and Control (IPC) Guidelines
The inclusion of IPC content within the MSS plays a key role in hospital safety, quality, and the prevention of HAIs.13-15 This justifies the question core component 2, where the IPCAF tool adheres to the national guidelines, i.e., the MSS criteria. The MSS checklist also acts as a potent tool for outlining the IPC-related criteria. Since the tools used here are IPCAF, we have discussed them in relation to the IPCAF core components only. Although an overall score above the mid-value has been achieved, areas for improvement include outbreak management, prevention of transmission of multidrug-resistant pathogens, implementation of guidelines according to local needs and resources, and regular monitoring of IPC guideline implementation. The hospital also lacks an AMS program. Literature also shows how the inclusion of AMS programs within the hospitals is crucial in mitigating the burgeoning issues of AMR and increasing patient safety. 22 However, several challenges might exist for the initiation of the program due to a lack of acceptability from physicians, resources, poor knowledge, attitude, and practice regarding antibiotic use, thus underscoring a coordinated need from the Ministry of Health and Health Directorate, Bagmati province, Nepal. 23 Judicious use of antimicrobials through the AMS activities is also an integral part of the global AMR response with HAI surveillance, proper sanitation, IPC measures, training, and educational skills. 24 Since IPC and AMS are complementary to each other in mitigating AMR, combined efforts of both can lead to increased results in comparison when they are working in silos. 24
Core Components 3: Infection Prevention and Control (IPC) Education and Training
Knowledge of IPC procedures among HCWs is crucial for effective IPC. Adopting a comprehensive approach to enhancing IPC intervention strategies is strongly recommended, with a key focus on improving HCWs’ compliance with IPC measures.25,26 The training mandates task-based strategies that are participatory and must include bedside simulation training as well. 27 Literature shows that IPC education and training, effective implementation of multimodal strategies, and strengthening IPC are essential to combat HAIs and AMR and to prevent and respond to outbreaks.4,28-30 A mid-value score of 50/100 highlights the need and significance of a dedicated educational training with a fixed time period within the hospital through a tailored approach, including electronic medium, timely reminders, and through information, education, and communication (IEC) materials. Training must be targeted towards three categories of human resources: IPC specialists, all care workers in patient care, and support staff for health service delivery on a routine basis. 27 Involvement of well-trained and dedicated professionals directly affects the implementation of other core components as well. Participants or individuals working in the IPC within healthcare settings must undergo rigorous continuous professional development and training sessions so as to maintain vigilance, along with being familiar with the updated rules and guidelines regarding decontamination, sanitation, hygiene, disposal, and occurrence of new infectious diseases. 31 Adil et al 2025 review also reveals lack of knowledge and training as one of the key barriers to compliance with IPC. Lack of training and knowledge also hinders the AMS programmes ultimately affecting the IPC level with increasing risk of infection.
Core Components 4: Health Care-associated Infection (HAI) Surveillance
According to the International Nosocomial Infection Control Consortium report on HAIs, the combined rates of HAIs were 7.28% and 10.07 Device-associated (DA) HAIs per 1000 patient days. 32 Similarly, a study conducted within a tertiary care hospital also showed a high incidence of HAIs (43%) in Intensive Care Units (ICU) and a high burden of multidrug-resistant microorganisms (74%), highlighting the importance of IPC programs and antibiotic stewardship. 33 Literature also recommends that around 70% of HAIs can be prevented by the effective implementation of an IPC-based program.5,33 The IPC team is responsible for the proper planning, conducting surveillance and analysis with a proper system, and reports to be submitted in a timely manner. 27 There seems to be a lack of surveillance within the hospital despite the IPC team working on the basis of the MSS criteria. This shows poor actions, a lack of dedicated, full-time workers, and a lack of well-trained professionals.
Core Components 5: Multimodal Strategies for Implementation of Infection Prevention and Control (IPC) Interventions
The lowest score observed in core component 5 (10/100) indicates a poor understanding and execution of multimodal strategies within the hospital. A successful implementation of a multimodal intervention reflects quality care and enhanced patient safety. 27 Despite the formation of a team and application of guidelines, the execution is poor for educational, communication, and several other indicators. This area can be seen as the most overlooked one among all the components. In addition to handling a large number of patients every day, a special focus should also be kept on mitigating the risk of infections that might spread among the hospital premises. Poor adherence to the elemental strategies, such as system change, monitoring feedback, communications and reminders, safety climate, and cultural change, increases the risk for HAIs. This underscores the need for interventions integrated into AMS programs that strengthen such elemental strategies to mitigate the risk of HAIs.
Core Components 6: Monitoring/Audit of IPC Practices and Feedback
This section observed the highest score, reflecting proper adherence. However, the lack of a proper monitoring plan with clear goals and a lack of focus on safety cultural factors leaves room for improvement. This component also focused on multidisciplinary team monitoring and audit of IPC practices, with the report evaluated by the hospital and senior administration. Monitoring and feedback can also be aimed at engaging stakeholders, creating partnerships, and developing working groups and networks. 27
Core Component 7: Workload, Staffing, and Bed Occupancy
The score of 40/100 indicates moderate adherence; however, it underscores significant gaps in optimal staffing and workload management. The high bed occupancy rate is associated with increased infection rates, likely due to insufficient time for thorough cleaning and disinfection between patients. 30 Additionally, an inadequate nurse-to-patient ratio may compromise effective hand hygiene practices and delay the timely isolation of infected patients. 4 The major issue can be found in workload management, as the WHO Workload Indicators for Staffing Need method has not been properly implemented. 27
Core Component 8: Built Environment, Materials, and Equipment for IPC at the Facility Level
The built environment and availability of IPC-related infrastructure, such as hand hygiene stations, isolation rooms, ventilation, and PPE, are essential for effective infection control. The score of 42.5/100 reflects major gaps in these areas. Poorly designed healthcare settings, including inadequate bed spacing, inaccessible safe drinking water stations, and inadequate waste disposal, are known to increase infection risks, particularly in LMICs. 29
Hospitals across countries had variable IPC scores when analyzed using the IPCAF tool. IPC assessment using the IPCAF tool across 33 Malawian hospitals revealed that the majority of hospitals (66.7%) were at an intermediate level, with only 26.4% at the basic level. Among the core components, the lowest median scores were observed in the monitoring/audit and feedback domain; accordingly, the overall assessment underscored the need for significant intervention in areas such as monitoring/audit and feedback, HAI surveillance, staffing, and bed occupancy. 34 Similarly, 65 healthcare facilities in Cameroon showed an inadequate (29%) and basic (57%) level of IPC. The majority of the hospitals lacked HAI surveillance. 35 Analysis of 15 healthcare facilities across the Pacific island countries and territories revealed significant strengths with the presence of IPC programs, updated guidelines, a monitoring feedback mechanism, with gaps in the training and education, and HAI surveillance. 36 Despite these studies dealing with multiple hospitals and healthcare facilities, our study focuses on a quality improvement project. Regardless of the setting, the theme is common, with shared gaps requiring interventions in areas such as education, training, HAI surveillance, and the development of monitoring/feedback mechanisms.
Recommendation
With a well-protected and dedicated budget for IPC, a strong program can be implemented through robust political commitments and proper adherence to guidelines. A well-dedicated team is required for successful implementation. The findings from this study could help in recommending a definitive proposal in encouraging the action plan via budget allocation and implementation in the hospital setting. With our action plan proposition in three terms, the study findings encourage immediate action (0-6 months term) for core components 5 (multimodal strategies) and 3 (education and training), as these scores are very poor. This could focus on properly appointing a dedicated IPC focal person with essential responsibilities for sanitation and hygiene, and on the identified gaps in the multimodal strategies. Similarly, to strengthen education and training, a mandatory IPC orientation must be introduced, starting with high-risk wards. Additionally, information, education, and communication materials could be developed with enhanced visualizations for doctors, nurses, and cleaning staff. A medium-term (6-18 months) focus could be conducted on core components 7 (workload and staffing), 8 (built environment and equipment), 4 (HAI surveillance), and 1 (IPC programs) for further enhancement. Lastly, long-term (18+ months) focus should be on core components 2 (IPC guidelines) for overall sustainability, maintenance, and optimization, as these scores are higher (Figure 5). This finding could also provide information on the IPC level status in accordance with the MSS standards and what is needed to enhance. It also creates room for discussion with the provincial health directorate to help provide IPC-level support and funding. A final recommendation is to implement the action plan with the help of all stakeholders and reassess overall improvement to once again determine the IPC status using the WHO fourth step for the implementation of IPC facility programs (Figure 1).
Strengths and Limitations
The study is the first quality improvement project on IPC assessment within the hospital, providing useful information across several IPC domains. However, the study also has limitations. Including healthcare professionals in a meeting, based on their IPC team experience, might introduce response biases. Similarly, the single-center design, the cross-sectional nature of the assessment, and the potential lack of objective verification of reported practices may affect the generalizability of the study. Additionally, since a box plot is used for the organizational and structural components, as the structural components are only two, the box distribution is naturally compressed; hence, interpretation regarding the variability should be made cautiously. While the figure was used for descriptive analysis, inferential statistics is limited by the small number of component scores. Lastly, the input and context regarding the ToT training narrative, including the lead author's involvement, might introduce observer and social desirability biases.
Conclusion
The IPC assessment identifies significant gaps across multiple core IPC components, and the hospital’s IPC status is classified as “Basic.” This assessment highlighted relative strengths; however, critical deficiencies were identified in key areas, including multimodal strategies, staffing, infrastructure, HAI surveillance, and IPC training. These findings underscore the urgent need for a comprehensive, team-based IPC approach, supported by effective implementation and continuous monitoring of the recommended IPC action plan with dedicated budget and resource allocation. Similarly, this pilot assessment could serve as a scalable model for other provincial hospitals in Nepal or in similar LMIC contexts.
Supplemental Material
Supplemental Material - Focusing on the III Strategic Priority of National Action Plan on Antimicrobial Resistance through the Baseline Assessment of Indicators of Infection Prevention and Control in a Provincial Hospital in Nepal: A Quality Improvement Project
Supplemental Material for Focusing on the III Strategic Priority of National Action Plan on Antimicrobial Resistance through the Baseline Assessment of Indicators of Infection Prevention and Control in a Provincial Hospital in Nepal: A Quality Improvement Project by Nabin Pathak, Prerana Shrestha, Shreya Dhungana, Sachita Barma, Sujil Manandhar, Prabhat Kumar Jha, Subash Karki, Surendra Dev Badu, Prashant Bidari, and Sunil Shrestha in INQUIRY: The Journal of Health Care Organization, Provision, and Financing.
Supplemental Material
Supplemental Material - Focusing on the III Strategic Priority of National Action Plan on Antimicrobial Resistance through the Baseline Assessment of Indicators of Infection Prevention and Control in a Provincial Hospital in Nepal: A Quality Improvement Project
Supplemental Material for Focusing on the III Strategic Priority of National Action Plan on Antimicrobial Resistance through the Baseline Assessment of Indicators of Infection Prevention and Control in a Provincial Hospital in Nepal: A Quality Improvement Project by Nabin Pathak, Prerana Shrestha, Shreya Dhungana, Sachita Barma, Sujil Manandhar, Prabhat Kumar Jha, Subash Karki, Surendra Dev Badu, Prashant Bidari, and Sunil Shrestha in INQUIRY: The Journal of Health Care Organization, Provision, and Financing.
Footnotes
Acknowledgments
The authors would like to thank all members of IPC who were involved in the data collection process. Similarly, the authors would also like to thank draw.io (https://app.diagrams.net/) and Lucidchart (https://www.lucid.co) to help us create with Figures 1 and ![]() respectively.
respectively.
Ethical Considerations
The permission letter to conduct this quality improvement project was taken from the hospital’s director to ensure validity (Reference number 1583). The permission was also obtained from the Drug and Therapeutic Committee (DTC) meeting held on July 1st, 2025 (Decision number 4), which was validated by the medical director and several members of the committee. Similarly, ethical approval was also taken from the Institutional Review Committee, Madan Bhandari Academy of Health Sciences (Approval number IRC-091-082-83) prior to the data collection process.
Consent to Participate
Since the study did not include clinical patients, informed consent form was not taken. However, for the participants from the IPC team, they were formally described about the data collection process and verbal consent was taken. They were informed that their participation in the research was entirely voluntary, as they were given the right to withdraw from the study if they wanted.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All the data are available within the study and as supplementary files.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.