
Abstract
Introduction
Thailand has implemented community-based long-term care (CBLTC) under the Universal Coverage Scheme (UCS) to support family caregiving and enhance the quality of life of dependent older adults. This study aimed to examine the CBLTC purchasing arrangements at the subdistrict level and the challenges that arise under these arrangements.
Methods
The qualitative case study method based on a health financing framework was adopted. Semi-structured interviews were conducted with 40 key informants from selected subdistricts in Nakhon Pathom Province, along with representatives from central and regional levels in Thailand. A thematic analysis was conducted using both inductive and deductive approaches.
Results
Findings revealed major challenges under the CBLTC purchasing arrangements, including budget constraints, misalignment between the payment and workload of volunteer caregivers, misalignment of service provisions outlined benefit package, and lack of monitoring system.
Conclusion
The findings highlight the need to improve CBLTC purchasing arrangements under the UCS to enhance the efficiency of provider payment mechanisms and address the needs of dependent older adults and support family caregiving.
Introduction
Globally, demographic transition has resulted in a shift in the age structure toward population aging. 1 Population aging is projected to substantially increase by 2050, with the majority residing in middle-income countries,2,3 thus raising needs and demands for long-term care (LTC). This situation gets intensified through a rise in the prevalence of chronic diseases, leading to disability and loss of intrinsic capacity among the older population. 4 Therefore, it is imperative for middle-income countries to proactively develop LTC systems before these issues escalate to significant challenges, require substantial resources to deal with. 5 However, raising public financing for LTC services alone is insufficient to ensure access to quality care or protect dependent older people and their families from financial impoverishment in the absence of effective purchasing arrangements.6,7
Purchasing is a core LTC financing function that refers to the allocation of pooled funds to providers for delivering LTC services on behalf of the population. 8 Purchasing is the mechanism through which LTC services are financed and paid for, and thus, it is linked to the design of payment methods, benefit packages, and performance monitoring. 6 Purchasing can be considered strategic when budget allocation is linked to information on provider performance and the LTC needs of the population, 9 and thus, it can be used as a tool to improve the quality and efficiency of LTC system. 10
Thailand is an upper-middle income country in Southeast Asia that is facing challenges from a rapid increase in population aging and LTC needs. 11 In response to these challenges, the country has started the implementation of community-based long-term care (CBLTC) under the Universal Coverage Scheme (UCS) for all Thai dependents who score 11 or lower on the Barthel Index of Activity of Daily Living (ADL) since 2016.12,13 However, the majority of CBLTC beneficiaries are dependent older people. It is important to note that, with the implementation of CBLTC services, families continue to be primary caregivers of the dependent older people as the objective of CBLTC is to support family caregiving, not to replace it. 14
Despite existing studies on CBLTC under the UCS in Thailand,15-17 little has been known about its implementation and challenges related to purchasing arrangements at the subdistrict level. This study examines the purchasing arrangements for CBLTC under the UCS at the subdistrict level in Nakhon Pathom Province, Thailand and emerging challenges under these arrangements.
This study extends the central inquiry into the following three sub-research questions:
CBLTC Purchasing Arrangements in Thailand
In Thailand, CBLTC is provided as a health benefit package under the UCS, a tax-based financing scheme administered by the National Health Security Office (NHSO). Purchasing CBLTC services under the UCS involves three key government institutions: the National Health Security Office (NHSO), Local Administrative Organizations (LAOs), and the Ministry of Public Health (MOPH). The NHSO designs the eligibility criteria and the benefit package in collaboration with the MOPH and annually allocates the budget to provide CBLTC services for all Thai dependent citizens. LAOs are designed as a primary mechanism for managing the CBLTC Fund at the subdistrict level. CBLTC service providers include primary care facilities, mostly health centers of the MOPH and Centers for the Development of Older Persons’ Quality of Life of LAOs. 13
The NHSO transfers funds to Local Health Funds earmarked for the CBLTC Fund, which is a subdistrict-level financing mechanism, to support CBLTC services under the benefit package based on a per capita basis. 18 In 2023, the per capita budget was US$ 188. 19 Despite being voluntary, 15 LAO enrollment in CBLTC provision reached 7,179 out of 7,759 (92%) in 2023. 19 At the subdistrict level, LAOs may designate either a primary care facility at the subdistrict level or a Center for the Development of Older Persons’ Quality of Life to provide CBLTC services. In most cases, the Memorandum of Understanding for CBLTC provision between LAOs and health centers is established. 13 Thus, LAOs perform as local purchasers at the subdistrict level. Primary care facilities, predominantly health centers, are the main providers of CBLTC services. Care managers in health centers coordinate service delivery and collaborate with volunteer caregivers at the subdistrict level within their areas of responsibility.
Payment for volunteer caregivers varies by provider agency. According to the Ministry of Health’s circular on lump sum payment for volunteer caregivers on October 1, 2017, volunteer caregivers providing CBLTC in collaboration with health centers shall receive no more than US$47 of lump sum payment per month, which is determined by the number of care recipients under responsibility: US$19 per month for those caring for 1–4 individuals and US$47 per month for those caring for five or more individuals. 13 Concurrently, Centers for the Development of Older Persons’ Quality of Life are authorized to establish their own regulations, including the determination of payment rates for volunteer caregivers (e.g., hourly rates).20,21
CBLTC Benefit Package Based on Care-needs Level
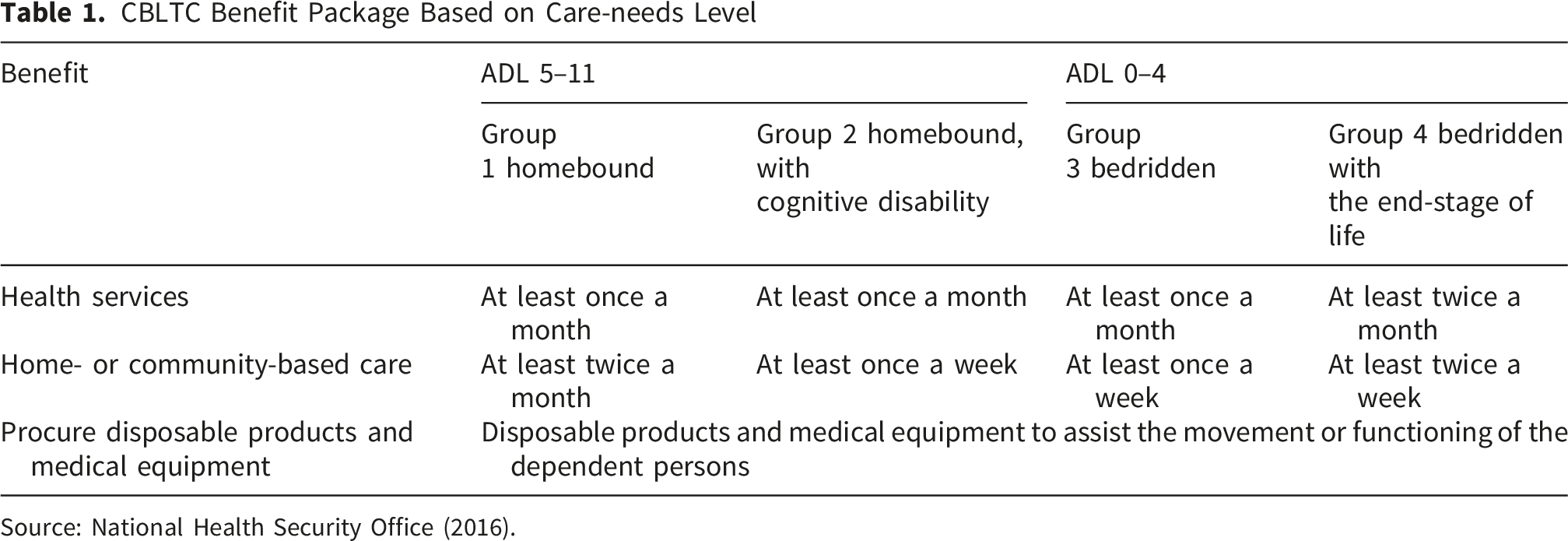
Source: National Health Security Office (2016).
Method
Study Setting
The study was conducted in Nakhon Pathom Province located within Bangkok Metropolitan Area in central Thailand, comprising a mixture of rural and urban areas. It had a population of 924,521 people in 2023 and is transitioning into an aged society, with older people aged 60 years or over accounting for 20.5% of the total population. 22 This province has early adopted the CBLTC since 2016. In 2022, 52 LAOs enrolled in provision of CBLTC with 1,713 beneficiaries.
Study Design
This study adopted a qualitative case study design, using the health financing framework based on the World Health Organization, 23 which lays out a structured way to analyze purchasing arrangement for CBLTC services.
Participants
In the first stage of participant selection, the chosen subdistricts were identified:11 out of 34 subdistricts in Nakhon Pathom with at least 20 CBLTC beneficiaries registered in the NHSO database were randomly selected. Subsequently, the health centers serving each of these selected subdistricts were contacted via telephone and verbally informed about the study. Care managers of health centers and executives of the LAOs in the selected subdistrict were invited for participation. In addition, care managers were requested to recruit volunteer caregivers for participation. To gain perspectives and insights from policy makers engaging in CBLTC, experts of NHSO and NHSO Region 5 along with executives of the Department of Health, Ministry of Public Health, were also invited to partake in the study.
From October 2023 to March 2024, stakeholders engaging in CBLTC financing and services in Nakhon Pathom Province and at the central and regional levels were selected as the research participants through purposive- and snowball-sampling. The inclusion criteria were being over 18 years of age; experienced in providing or financing of CBLTC for more than 1 year; being a care manager, a volunteer caregiver, or an executive of the LAOs from the 11 selected subdistricts of Nakhon Pathom Province, or an executive or a specialist at the central or regional level; and voluntarily participating and signing the informed consent. Participants who were not willing to participate in the interview were excluded.
Interview Guide
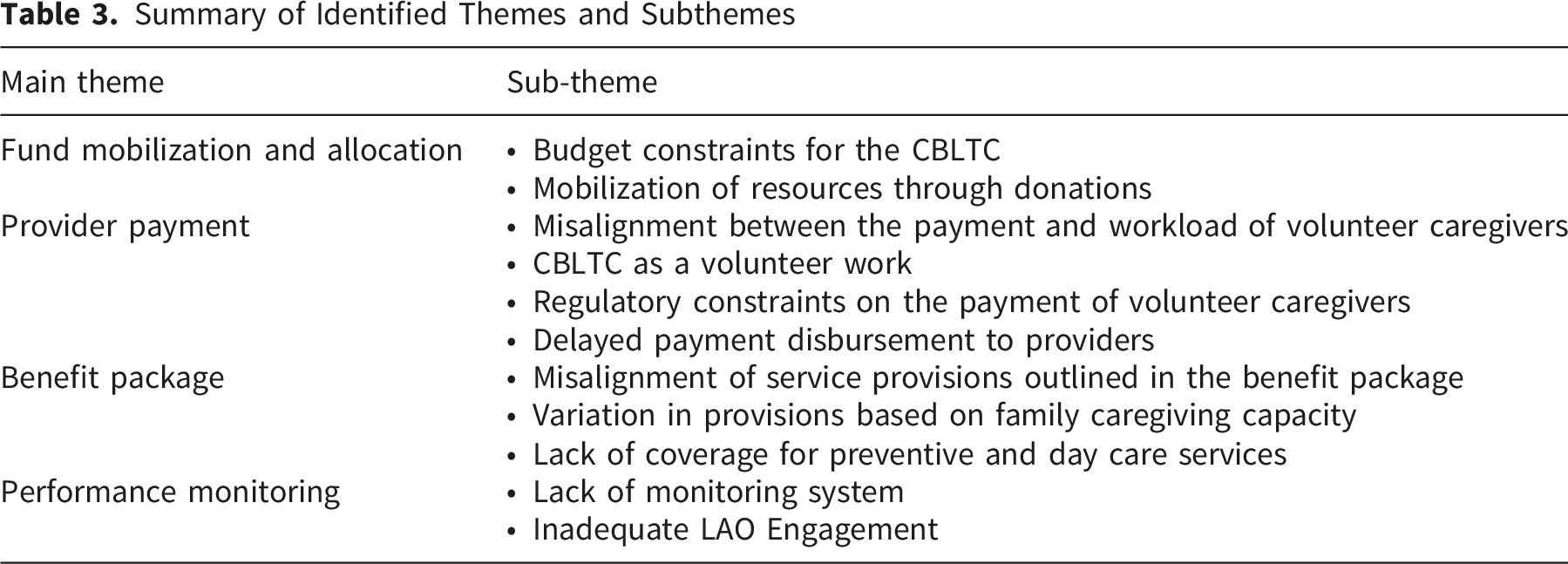
The health financing framework was used to direct the development of the interview guide comprising three themes: fund mobilization and allocation, provider payment, and benefit package. The perceptions of issues in budget allocation and provider payment were highlighted as core questions. Two researchers conducted pilot interviews with three eligible participants to assess the applicability of the interview guidelines. See Supplementary for the full interview guide.
Data Collection
Semi-structured interviews, lasting approximately 45–60 minutes, were conducted and voice-recorded in private rooms at health centers or LAOs in Nakhon Pathom. The central and regional level participants were interviewed via Zoom with audio recording. Two university lecturers with over 15 years of experience in health systems and policy research, specializing in health financing, conducted the interviews: one was female with PhD, and the other was male with MD and PhD. Additionally, field notes were taken during the interviews.
Information sheets containing details about the researchers, study purpose, research benefits, research methods, participant selection, voluntary participation and possibility of withdrawal, along with informed consent forms were distributed to all participants prior to the semi-structured interview.
Data Analysis
The interviews were audio recorded, transcribed verbatim, and anonymized by assigning a code to each participant. The interview transcripts were analyzed using thematic content analysis, an approach appropriate when the study has pre-defined objectives and frameworks. 24 Coding was done manually with an MS Excel template. An extraction matrix was developed for this purpose, mostly based on pre-identified themes but also with addition of emergent themes (deductive and inductive approach). Themes and codes reflected the purchasing arrangements of CBLTC of the study, focusing on fund mobilization and allocation, provider payment, benefit package, and performance monitoring. Data saturation was reached after the coding and analysis of the 40th participant’s transcript. This study employed data triangulation from various sources through different groups of participants to verify the information and ensure the credibility of the data analysis. The analysis was shared with a small group of participants for feedback, thereby enhancing the rigor of the analytical process. This study was conducted and reported in accordance with the Comprehensive Criteria for Reporting Qualitative Research (COREQ). 25
Results
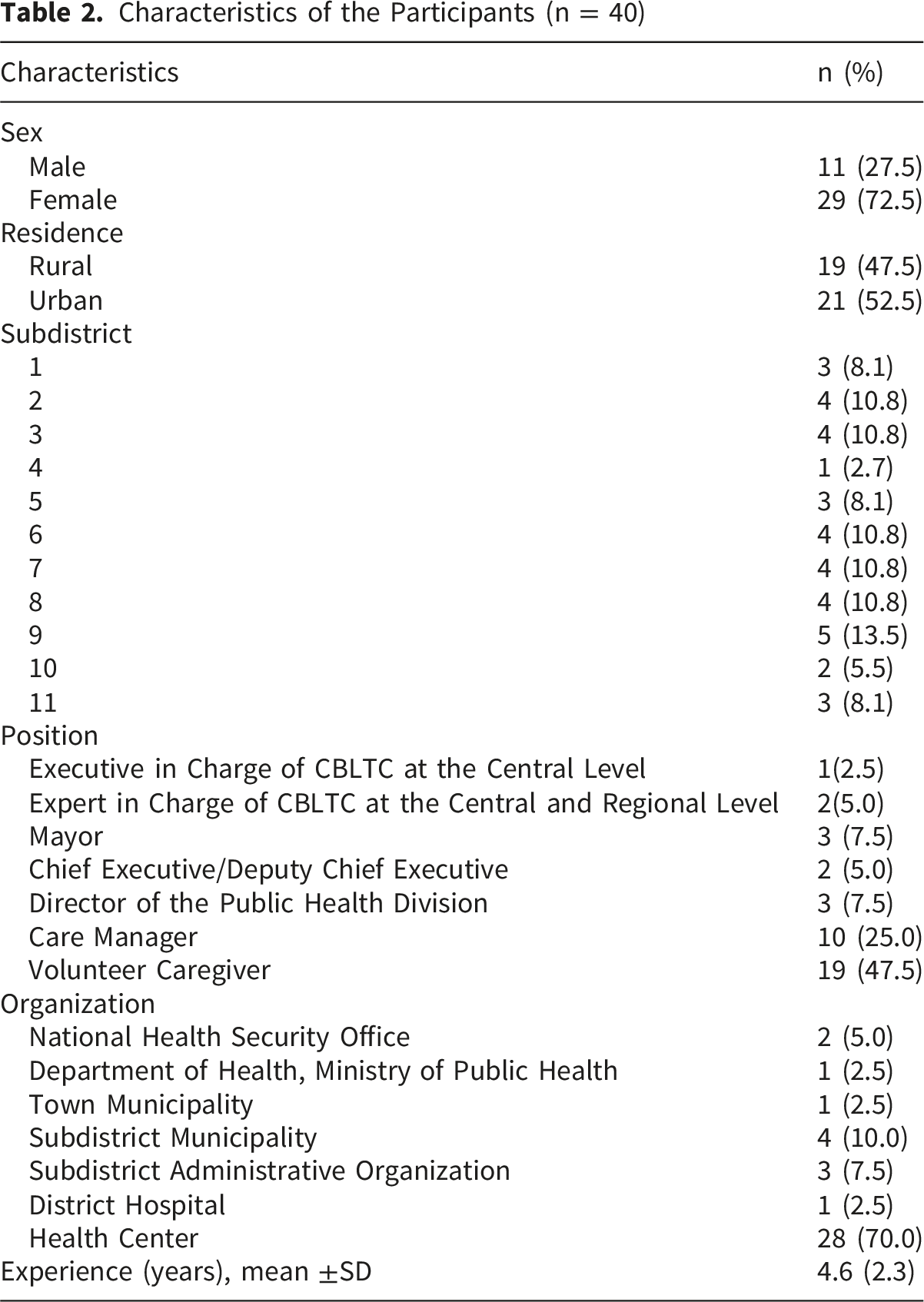
Characteristics of the Participants (n = 40)
Summary of Identified Themes and Subthemes
Theme 1: Fund Mobilization and Allocation
Budget Constraints for the CBLTC
Inadequate CBLTC budget was commonly highlighted among participants. They pointed out that the per capita budget at the time of the study was insufficient to cover both hiring more volunteer caregivers and procuring the disposable products and medical equipment to meet the needs of dependent older adults. Thus, many suggested that the per capita budget be increased to enhance the quality of life of dependent older people. ‘The number of bedridden older people is continuously increasing. This increases the workload of the staff, and they cannot handle it. The budget is insufficient to hire more volunteer caregivers.’ (Deputy Chief Executive, Subdistrict Administrative Organization, Subdistrict 6) ‘I would like to see increased budget support for CBLTC as this is a major issue. We are now entering an aging society with a growing number of older adults. Greater emphasis should be placed on elderly care to reduce level of dependency.’ (Care Manager, Health Center, Subdistrict 2)
Mobilization of Resources through Donations
‘We used to have only two patient beds, but now we have nearly 20 beds, mainly from Rotary donations.’ (Care Manager, Health Center, Subdistrict 5) ‘Some people need beds or wheelchairs. We usually check with the hospital to see if they have any available to lend or if there are any donation. Sometimes we ask community leaders for help, and if nothing is available, we coordinate with the municipality—but most of the time, the hospital provides them.’ (Volunteer Caregiver 1, Subdistrict 4)
Theme 2: Provider Payment
Misalignment between the Payment and Workload of Volunteer Caregivers
Several participants stated that the current lump sum payment was not commensurate with the volunteer caregivers’ workload. First, the addition of one care recipient shifted the payment from US$19 per month (1–4 individuals) to US$47 per month (5 or more individuals). Second, some volunteer caregivers were responsible for more care recipients without a corresponding increase in payment, especially in areas with a volunteer caregiver shortage or higher number of dependent older people. Third, the care need level of each dependent older person varied. Thus, some dependent older adults required more care visits than others. Furthermore, some raised that this lump payment was insufficient to cover fuel fees for visiting dependent older people at home. ‘Each volunteer caregiver takes care of 10 dependent older people. This is because our villages have many dependent older people… I think the compensation is not proportional. It should be raised.’ (Volunteer Caregiver 2, Subdistrict 7) ‘Right now, it’s like a flat-rate payment. Everyone gets paid the same regardless of workload, which I do not think is fair.’ (Care Manager, Health Center, Subdistrict 11)
CBLTC as a Volunteer Work
Many volunteer caregivers perceived the provision of CBLTC services as volunteer work, and, thus, the compensation did not matter to them. They had long been engaged in volunteer work and served the dependent older people in their communities since no compensation was provided. ‘I think the compensation is appropriate. Even if I do not get it, it’s totally fine. I have never expected any compensation. I do this work from my heart.’ (Volunteer Caregiver 1, Subdistrict 2) ‘Even if no payment is provided, I continue to work without complaint. In the past, there was no compensation, and it was not an issue. I have long been engaged in caregiving and accustomed to caring for patients and those in need of assistance. Financial compensation is not my primary concern.’ (Volunteer Caregiver 2, Subdistrict 3)
Regulatory Constraints on the Payment of Volunteer Caregivers
Although the NHSO did not establish a standardized payment rate for volunteer caregivers, its utilization became subject to the financial regulations and payment mechanisms of the receiving agencies once the per capita budget was transferred to CBLTC providers. All CBLTC providers in this study were health centers of the MOPH. Thus, they had to follow the MOPH’s circular on lump sum payment for volunteer caregivers, resulting in similar payment rate applying for volunteer caregivers across selected districts. ‘NHSO provides only general guidance for the CBLTC. Payment for volunteer caregivers follows the regulation of the responsible agency. The MOPH has its own payment guidelines. In the case of local governments, hourly payment is possible.’ (Expert 2, National Health Security Office)
Delayed Payment Disbursement to Providers
Delayed disbursement of payment to volunteer caregivers was also an issue mentioned by participants. Some said that hierarchical approval in the bureaucracy system caused this delay. In normal practice, after the LAOs approve of individual care plans, care mangers need additional approval processes from the higher public health authority, either the District Health Office, the Provincial Public Health Office, or both, to use the funds. ‘First, the Subdistrict Municipality must approve individual care plans. Subsequently, care manager must develop a CBLTC project proposal to utilize CBLTC funds, with further approval required from the District Health Office and the Provincial Public Health Office.’ (Care Manager, Health Center, Subdistrict 9)
Theme 3: Benefit Package
Misalignment of Service Provisions Outlined in the Benefit Package
Some volunteer caregivers reported that their visits were less frequent than the level stipulated in the care plan and guidelines in the benefit package, especially for bedridden older people who required greater frequency of visits. The participants reported two main challenges affecting their service provision and frequency of visits. First, they had other responsibilities, such as taking care of their families, routine work, and other volunteer work. Notably, most of them were both volunteer caregivers and volunteer health workers. Thus, they needed to balance volunteer care work and other tasks. ‘I am often able to follow the guidelines, but there are times when I cannot, as I also need to care for my children and my brother.’ (Volunteer Caregiver 1, Subdistrict 8) ‘Sometimes I visit dependent older people as required by the care plan. But sometimes, I don’t. It depends on my availability.’ (Volunteer Caregiver 2, Subdistrict 9)
Second, family caregivers’ preference or acceptance of volunteer caregivers influenced the implementation of care plan. Resistance or limited trust to volunteer caregivers limited the provision of planned CBLTC services. Some care managers and volunteer caregivers reported that family caregivers, particularly those living in towns or subdistrict municipalities, which are considered urban areas, did not want volunteer caregivers to pay frequent visits to dependent care recipients at home. ‘I admitted that sometimes volunteer caregivers don’t visit dependent older people according to the care plan… In some cases, their relatives don’t want volunteer caregivers to visit their home very often because they want to preserve their privacy. In homes with valuable items, their relatives refuse to allow volunteer caregivers to enter.’ (Care Manager, Health Center, Subdistrict 1) ‘At the beginning, it was difficult to reach dependent older people because their families did not accept us, so we had to bring the care manager along when visiting them. But as time goes by, they want us to visit even more often.’ (Volunteer Caregiver 1, Subdistrict 5)
Variation in Provisions Based on Family Caregiving Capacity
Some participants reported that variations in family caregiving capacity shaped the scope and intensity of service provision, which can be diverse from an individual care plan. In households where dependent older persons received adequate support from family caregivers, volunteer caregivers tended to focus primarily on health education rather than direct personal care. ‘For those who have no severe needs and are well-taken care of by their families, we do not need to help them perform tasks. Usually, I guide them on how to take the medicine or perform stretch exercises and remind them about their appointments.’ (Volunteer Caregiver 2, Subdistrict 11)
In contrast, volunteer caregivers frequently expanded their responsibilities beyond the prescribed care plans and scheduled visits when family caregiving capacity was limited or insufficient, particularly during periods of heightened care needs, such as the development of bedsores. ‘Cases with bedsores are particularly demanding. We have to help with wound care, and if family members cannot do it, we need to visit them every day.’ (Volunteer Caregiver 2, Subdistrict 1)
Lack of Coverage for Preventive and Day Care Services
Although many think that services included under the CBLTC benefit package are appropriate for dependent older people, some participants maintained that it is necessary to expand the service coverage to include day care and preventive services to better address the diverse needs of older people. They highlighted that both services offer a range of activities that can help maintain and potentially improve the function ability of older adults. ‘There should be greater emphasis on the care of older persons to reduce dependency risk. This could begin early in older age by providing support that helps them maintain a good quality of life.’ (Care Manager, Health Center, Subdistrict 2) ‘A day care center for dependent older people living alone should be established…I have discussed this with the mayor, and the municipality needs to find a place for it.’ (Caregiver 1, Subdistrict 2)
Theme 4: Performance Monitoring
Lack of Monitoring System
Participants pointed to a gap in the governance in purchasing, with the absence of a formal service monitoring system for CBLTC providers and unclear oversight between the NHSO and LAOs. This ambiguity in roles appeared to have led LAO participants to defer responsibility to care managers within health centers of the MOPH, indicating a lack of clearly defined accountability mechanisms. Such unclear responsibility for performance monitoring contributed to inconsistencies in service delivery and deviations from both the benefit package guidelines and individual care plans, ultimately undermining the quality and standardization of care provided. ‘NHSO cannot audit CBLTC services and individual care plans. The CBLTC Fund Committee will review them.’ (Expert 1, National Health Security Office) ‘Health center takes care of it (CBLTC)… LAO mostly approves all the individual care plans that the health center has proposed.’ (Mayor, Subdistrict Administrative Organization, Subdistrict 3)
Inadequate LAO Engagement
Participants highlighted a gap between the intended and actual roles of LAOs in the CBLTC system. Although LAOs are formally expected to function as purchasers at the subdistrict level, in practice they were perceived to adopt a largely passive role, operating mainly as financial intermediaries. This may constrain the responsiveness and effectiveness of CBLTC services. Consequently, participants expressed expectations for LAOs to perform a more proactive and engaged role to better align service provision with the needs of dependent older adults and system objectives. ‘LAOs are expected to take a leading role and become a center in managing the CBLTC.’ (Expert 1, National Health Security Office) ‘They [LAOs] don’t get involved in CBLTC. They need to pay more attention. They need to review the budget for each care recipient in the community and what care recipients need and what is missing. They need to know who is getting involved, who does what? They need to visit dependent older persons, but they don’t…Hope that cooperation will happen in the future.’ (Volunteer Caregiver 1, Subdistrict 1)
Discussion
Based on the health financing framework, this study analyzed the purchasing arrangement of CBLTC services under the UCS at the subdistrict level in Nakhon Pathom Province. Findings highlight the implementation challenges of purchasing arrangements, including fund mobilization and allocation, provider payment, benefit package, and performance monitoring. The findings suggested that the purchasing arrangement should be adjusted and refined to enhance the efficiency and quality of service delivery to increase the quality of life of dependent older population and support family caregiving, which are the objectives of the CBLTC system.
Expanding Fiscal Space through Budgetary Integration
Participants consistently identified the limited per capita budget for CBLTC as a key challenge, while seeking medical equipment donation is a strategy to mobilize additional resources. However, it is a complementary source. The findings underscore the need to expand fiscal space for CBLTC by increasing not only the per capita budget but also by mobilizing additional funding sources from existing budgets. Integration of health and social service budgets for dependent older persons at the subdistrict level, including the CBLTC budget from the NHSO, social service budgets for older persons from the Ministry of Social Development and Human Security, and financial contributions from the LAOs, is a potential approach. To enable LAOs to co-finance the CBLTC provision, the government should increase fiscal transfers to LAOs to at least meet the ceilings stipulated in the Decentralization Act. Additionally, attention is needed to how these additional resources are distributed. Ensuring that increased funding reaches volunteer caregivers, alongside more equitable allocation of medical equipment targeting higher-need households, may help mitigate the family’s financial burden associated with LTC.26,27
Refining the Provider Payment Mechanism
The subdistrict CBLTC payment mechanism used a similar approach, in which volunteer caregivers were compensated through a lump sum payment. Participants mentioned that the payment was inadequate and disproportional to the workload of volunteer caregivers. The findings suggested that the lump sum payment reduced the service provision, contributing to inconsistencies in meeting the CBLTC benefit package guidelines in terms of frequency and duration of services. This finding is consistent with previous research demonstrating that full-time paid caregiving models achieved better quality of services than the part-time volunteer-based models,27,28 in which expectations regarding volunteers’ time commitment or caregiving capacity were often unrealistic. 29 A shift from volunteer-based caregivers to full-time paid caregivers may enhance the continuity and quality of CBLTC services. However, the existing public financial management regulations within the MOPH limited the adaptability of provider payment mechanisms and prolonged the budget approval process, resulting in delayed fund disbursements to volunteer caregivers. This suggests that LAOs should designate a Center for the Development of Older Persons’ Quality of Life as a CBLTC provider instead of a health center of the MOPH to enhance flexibility and timely resource allocation at the provider level. This is because each center can set up its own financial management regulation for CBLTC, including compensation for volunteer caregivers. This adjustment allows a more precise reflection of compensation in relation to the workload of volunteer caregivers.
Adjusting the Benefit Package and Care Plan to Meet the Needs of Older Adults
The participants mentioned that the benefit package should be expanded to meet the needs of older people by including early preventive services to prevent functional decline and delay the onset of long-term care dependency among at-risk older populations, particularly frail or prefrail older adults.30,31 Day care services should also be included to support dependent older people living alone and family caregivers in need of respite care. 32 In addition, it is evidence that day care center attendance helped maintain the quality of life of dependent older adults.33,34 Meanwhile, some family caregivers preferred to take care of dependent older people themselves and requested less frequent visits from volunteer caregivers, especially those in urban subdistrict areas, due to the issue of the acceptability of volunteer caregivers. 35 This suggests that an individual care plan under the benefit package should consider the care needs of dependent older adults, living arrangements, and family support capacity in resource-limited contexts. CBLTC may target support to those with greatest needs, 36 such as dependent older adults living alone or from low-income households. Meanwhile, families with the willingness and capacity to provide care themselves should be supported to do so. Nevertheless, the CBLTC system can still play a facilitative role by supplying disposable products and medical equipment and offering training to family caregivers.
Enhancing the Performance Monitoring
The findings revealed that the performance monitoring system for CBLTC was absent. This suggests that the management information system for CBLTC should be put in place to collect data for monitoring the quality of service and inform the design of payment mechanism.37,38 In addition, with the decentralized CBLTC system, the role of LAOs in purchasing CBLTC services was not aligned. The LAOs limited exercise of strategic purchasing functions such as provider oversight and performance monitoring. 38 The findings suggest that the NHSO should strengthen LAO engagement and management capacity or reassess the designation of local purchasers for CBLTC. Given the small size and limited capacity of LAOs at the subdistrict level, assigning the purchasing role to District Health Boards may be a more viable policy option, as they possess greater administrative scale and institutional capacity.
To our knowledge, this is the first study that explores the purchasing arrangement of CBLTC services under the UCS in Thailand. This study also contributes to the knowledge gap on CBLTC purchasing arrangements in the Asian context. Although the findings provide useful insights, this study has some limitations. First, the generalization of this study is limited. The study only includes 11 subdistricts in Nakhon Pathom Province in central Thailand. Further studies in other parts of Thailand are needed. Second, this study’s findings of this study are drawn from the provider’s perspective. Thus, future studies should explore the user’s perspective. Finally, the CBLTC system in Thailand is constantly changing: technically, this study is assumed to capture only the situation as of March 2024.
Conclusion
Based on the health financing framework, our study provided insights into the challenges emerging under the purchasing arrangements of CBLTC services under the UCS. Major challenges include budget constraints, misalignment between the payment and workload of volunteer caregivers, misalignment of service provisions outlined benefit package, and lack of monitoring system. Insights from this study can contribute to the policy discussion on how to improve the purchasing arrangements for CBLTC to meet the LTC needs of dependent older people and support family caregiving in Thailand, as well as in other countries that are planning to implement CBLTC system in response to population aging challenges.
Supplemental Material
Supplemental material - Purchasing Community-Based Long-Term Care Services Under Thailand’s Universal Coverage Scheme: A Provider’s Perspective
Supplemental material for Purchasing Community-Based Long-Term Care Services Under Thailand’s Universal Coverage Scheme: A Provider’s Perspective by Aungsumalee Pholpark, Samrit Srithamrongsawat in INQUIRY: The Journal of Health Care Organization, Provision, and Financing
Footnotes
We would like to thank all participants who provided valuable information for this study.
Ethical Considerations
This study was approved by the Mahidol University Social Sciences Institutional Review Board (MUSSIRB) (Certificate of Approval No. 2023/107.2206).
Consent to Participate
Written informed consent was obtained from study participants.
Author Contributions
AP and SS conceptualized the study. AP and SS collected the data. AP and SS conducted the data analysis. AP and SS wrote the first draft and the revision of the manuscript. All authors approve of the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is funded by National Research Council of Thailand (NRCT): Contract number N42A660932.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated during and/or analyzed during the current study are not publicly available due to privacy concerns but are available from the corresponding author on reasonable request.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.