
Abstract
Introduction
Chronic disease management depends on sustained interaction with primary care services, yet these interactions may be shaped by digital inequalities in urban middle-income settings. This study examines whether household digital access is associated with differences in primary care utilization and hospitalization outcomes among adults with chronic diseases in three Caribbean cities of Colombia: Barranquilla, Cartagena, and Santa Marta.
Methods
This study used a quantitative, observational, cross-sectional, and exploratory design based on secondary anonymized data from national household surveys, SISPRO administrative health records, and national ICT indicators. The analytical sample included adults aged 18 years and older living in urban households in Barranquilla, Cartagena, and Santa Marta who had at least one chronic disease identified through survey or administrative records and had complete information for the dependent variable and all covariates included in the multivariable models. Individuals younger than 18 years, residents of rural areas, persons without evidence of chronic disease, and observations with missing data in key analytical variables were excluded. Descriptive comparisons were combined with binary logistic regression models including household internet access, age, gender, education, income quintile, insurance regime, and city fixed effects, and a probit model was estimated as a robustness check.
Results
Descriptive findings show that individuals living in households with internet access reported more primary care visits than those without access. Across the pooled sample, predicted probabilities of hospitalization were lower among individuals with household internet access, with the largest difference observed in Santa Marta. The robustness analysis using a probit specification confirmed the same negative association between household internet access and hospitalization probability.
Conclusion
The findings provide preliminary evidence that household digital access is associated with greater primary care utilization and lower hospitalization risk among adults with chronic diseases in the three cities studied. Although the cross-sectional design does not allow causal inference, the results suggest that digital inclusion may be a relevant complementary component of primary care-centered strategies for chronic disease management in urban middle-income contexts.
Introduction
Chronic diseases have become the main causes of illness and system load for health care systems in high- and middle-income countries. Diabetes, hypertension, and other chronic conditions require regular monitoring and management, frequently involving visits to health care providers and successful transitions between different levels and sites of care. Primary health care has a key role to play in both preventing chronic diseases and detecting and managing those that do occur on an ongoing basis. There is growing attention to patient-centred approaches to chronic illness management and to more integrated models of care to improve both treatment and continuity of care for patients with chronic diseases.
There is a rapid increase in the use and integration of digital technologies for primary health care delivery. Digital access to primary health care for urban populations with socioeconomic inequalities could potentially reduce access barriers and affect health system visit rates and follow-up adherence for patients. It also could affect patient management for those with chronic diseases. Studies based on chronic care models and community-based interventions showed that accessibility and integration of health services are critical to obtaining optimal health outcomes for patients with chronic diseases. 1
In rapidly changing middle-income countries, serious digital and health inequities persist. In unequal cities, differences in digital access translate into different health outcomes through unequal access to primary health care services. Integrated chronic care services are delivered from a single primary care practice; therefore, in addition to having sufficient institutional capacity, patients and health professionals must be able to interact with the system through different technological channels. 2 This study investigates the relationship between digital access and primary care utilisation.
This study assessed the relationship between household digital access and chronic disease management in three cities in the Caribbean region of Colombia: Barranquilla, Cartagena, and Santa Marta. The three cities are of similar size and have similar sociodemographic profiles, but they have different levels of digital infrastructure as well as socioeconomic and health system characteristics. The objective was to identify initial patterns that can orient the development of primary care-centered digital health strategies in urban settings similar to those studied. Although this study focuses on the Colombian Caribbean, the research questions have wider applicability in middle-income cities throughout the world where different dynamics of digital inequality intersect with varying levels of chronic disease prevalence and unequal access to health infrastructure.
Literature Review
Theoretical Foundations of Primary Care–Centered Chronic Disease Management
Chronic disease care models, such as the Chronic Care Model, include elements of structured follow-up and patient involvement at all levels of the health care system. All services are organized around a primary care “hub” to monitor and prevent complications.
This report focuses on how patient-centred health care delivery is organised around the needs, experiences and abilities of individual patients with chronic conditions and health care practices. In turn, patient-centred health systems are organised around patients with chronic conditions and health systems. There is a growing body of research evidence on the effects of patient-centred approaches to health care practice, such as treatment adherence, provider-patient communication, and patient health outcomes. 3 The organisation and structuring of patient-centred health systems will likely have an impact on the behaviour and health of patients.
New digital technology is being introduced in many contemporary health care systems to support and enhance the delivery of care within primary care-centered models of care. Teleconsultation, remote monitoring of vital signs and digital appointment scheduling are examples of new ways to enhance communication, care continuity and access to care for patients and health professionals. Although the technology is still in its early phases, it is mainly used to support and extend primary care in order to help health care systems control costs and deliver integrated patient care to address the health needs within a population health approach. The patients who have a chronic health condition are of particular interest.
Primary Care and Chronic Disease Management as a Population Strategy
Primary care has long been recognized as the cornerstone of effective health systems, particularly in the management of chronic diseases. Chronic conditions such as diabetes, hypertension, and cardiovascular illnesses require continuous, coordinated, and preventive care rather than episodic treatment. Theoretical frameworks such as the Chronic Care Model emphasize the role of proactive, patient-centered primary care systems in improving long-term outcomes. Studies in health systems research show that coordinated primary care reduces hospitalizations, improves adherence to treatment, and enhances patient satisfaction.2,4
From a theoretical perspective, chronic disease management depends on the integration of services across different levels of care. Integrated care models argue that fragmented systems lead to higher costs and worse outcomes, especially for patients with multiple chronic conditions. Patient-centered care, in this context, becomes both an ethical and operational principle, as it ensures that treatment decisions, monitoring, and follow-up are tailored to individual needs. 3 The effectiveness of these models depends on the strength of primary care as the coordinating hub of the system. Community-oriented approaches also reinforce the importance of primary care as a population-level strategy. Rather than focusing exclusively on clinical treatment, such approaches integrate prevention, early detection, and social support mechanisms. Research on palliative and chronic care has shown that community-based models can address the needs of patients more effectively, especially in contexts with resource constraints. 1 This perspective shifts the focus from isolated clinical encounters to broader health system organization.
Integrated chronic care systems also rely on patient engagement and continuity of care. Evidence from long-term care settings indicates that patients’ perceptions of integrated services are associated with better experiences and improved adherence to treatment plans. 2 These findings support theoretical models that emphasize coordination, continuity, and communication as key determinants of chronic disease outcomes. Overall, the literature suggests that effective chronic disease management requires a primary care-centered system that integrates services, emphasizes patient-centered practices, and promotes continuity of care. However, the success of such systems increasingly depends on digital tools that facilitate communication, monitoring, and access to services.
Digital Health Technologies and Chronic Disease Self-Management
Digital health technologies have the potential to transform the way patients with chronic diseases are managed and cared for. They can enable health care professionals to be more proactive in their support of patients between face-to-face consultations through the use of technologies such as telemedicine, remote health monitoring technologies, mobile apps, and electronic health records. From a theoretical perspective, digital health technologies have the potential to support patient self-management of chronic diseases by enabling patients to take an active role in managing their health condition on an ongoing day-to-day basis. Monitoring their health through various digital sources and making healthy choices, together with those close to them, in response to changing circumstances, is fundamental to this process.
Empirical research has increasingly demonstrated the effectiveness of digital health interventions in improving adherence to treatment and health outcomes for a number of different chronic diseases.5,6
Digital self-management can also be understood through behaviour change and health communication theories and models. Digital technologies can offer people reminders, the ability to track health-related data, and ways of communicating with health professionals. This can reinforce healthy behaviour and support adherence to medication. This paper draws on research carried out with older adults living with multiple health conditions to explore how people use ICTs to support self-management and whether this helps them to take the most beneficial routes to health and outcomes. The paper also illustrates how digital technologies are being used in clinical decision-making and timely intervention in physical and mental health care. Monitoring patients remotely using the latest technologies enables providers to identify complications early so that appropriate action can be taken and patients receive the best possible quality of care. A new systematic review of the evidence examines the impact of digital technologies on quality of care and clinical outcomes for people with chronic kidney disease and common comorbidities. The review highlights the growing use of technologies that rely on a continuous feedback model.
However, the impact of digital health interventions depends on many different contextual factors, including the digital skills of health professionals and users, the quality of the health information infrastructures available to support health care, and the integration of health information systems. The implementation of digital health has been found to be constrained by a variety of barriers related to access to technology, organisational issues, and user issues. Digital health technologies have the potential to extend the functions of primary health care but, in practice, are largely used as additional tools to support routine clinical work, optimise follow-up and monitoring, and facilitate continuity of care and communication between patients and health professionals at different points in the health and care organisations that deliver primary health care. Digital health technologies can support self-management and additionally can be used to monitor patients with complex care needs and their relatives to help ensure adherence to medication regimens for chronic diseases.
Barriers, Inequalities, and Adoption of Digital Health
While the potential benefits of digital health technologies are considerable, they are currently being diffused unevenly across different populations and health systems. Their spread depends both on the availability of technology and on the social acceptance of new technology. Several models explain technology adoption. The Technology Acceptance Model considers the intention and behaviour of health care professionals and patients to adopt health information technologies. Their intentions and behaviour in using health information technologies are influenced by perceived usefulness, ease of use, and institutional and organizational support. 7
The concept of acceptance of health care service technologies in health care settings also requires differentiation between general acceptance of health care service modalities and acceptance of particular functions of digital therapeutics. General acceptance of health care technologies refers to acceptance of health care services delivered through technologies such as artificial intelligence, telehealth, and digital therapeutics, whereas acceptance of a particular digital therapeutic function refers to users’ perceptions of specific applications, features, or health-related uses within digitally delivered care. Therefore, the first construct covers a broad array of health care technologies and related attitudes, whereas the second refers to attitudes toward specific functions that guide behavioural intentions.
In research on digital health acceptance, a distinction must also be made between acceptance of the modality of digital health and acceptance of specific outcome-related functions. A person may have a very positive attitude toward digital health technologies in general but show only moderate acceptance of specific functions. This higher-order acceptance of the modality is a distinct phenomenon and may be influenced by different factors than acceptance of a specific use case, such as data tracking, access to relevant health information, responsiveness to health needs, ease of use, perceived risk, clinical relevance, and trustworthiness. Although there may be some overlap between general attitudes toward digital health technologies and specific functions, both constructs are distinct and should not be conflated in research or practical application.
When building a model of acceptance of a particular digital therapeutic capability, researchers should define the theoretical construct of the independent variable carefully. In this case, the strong structural path to acceptance of embedding data-driven, predictive, or real-time capabilities into mental health treatments indicates that a distinction must be maintained between broad acceptance of digital and AI-enabled care for general health care delivery and acceptance of one specific digital therapeutic function. Accordingly, very large coefficients for such structural paths should be interpreted cautiously because they may reflect insufficient conceptual separation between constructs.
Digital divides can also occur at the patient level across socioeconomic status, age, education, or geography. These social differences can prevent patients from effectively using technology for telehealth, seeking online health information, and communicating with health care providers. Prior research on telehealth has highlighted both the benefits and the challenges of incorporating digital health technologies into clinical practice, showing how technology can increase access to care for some populations while denying access to others. 8 It is also important to note that having household internet access does not necessarily mean that all individuals within the household have the skills, routines, devices, or service quality needed to use those resources effectively for health-related purposes. Household-level data therefore require cautious interpretation when used as evidence of digital divides, as there may be considerable variation within households with internet access.9-11
Digital systems, including contact tracing apps, telemedicine platforms, and health applications, were rapidly scaled up during the COVID-19 pandemic. The effectiveness of these systems largely depends on the existence of sufficient digital infrastructure as well as adequate digital literacy among affected populations. Experiences during the pandemic suggest that health policymakers should address digital inequalities more directly.
The adoption of digital health into health care is influenced by economic, institutional, and social factors. A growing body of theory seeks to explain the complex sociotechnical process of digital health innovation by moving beyond a neutral technology-then-innovation perspective and focusing instead on interactions between technology, users, and organisational context.
Empirical Evidence on Digital Inequality and Health Access in Latin American and Middle-Income Contexts
This study explores the potential of telehealth to improve access to healthcare in developing countries. It contests prevailing, availability versus access oriented approaches to understanding digital inequality and suggests that inequality is a “structural problem” that goes beyond simple availability of technology. Views on digital access in Latin America have been increasing in recent years. In Brazil, for instance, despite the growth in internet availability, significant inequities in access persist. This study aims to explore the structurally socially stratified field of access to digital health technologies in a middle-income country, and to investigate the findings in the context of health access. Access to care delivered and facilitated by digital technologies can condition who can benefit from such innovations.
In Brazil, access to and treatment by health services can be enhanced by digital health, provided there are sufficient institutional and technological conditions for effective implementation and use of health technology. The aim of this multicenter, prospective study was to evaluate the effects of digital health technologies for integrated management of patients with suspected or confirmed dengue, chikungunya and Zika viruses. A total of 15 primary health units in Brazil participated in the study, including seven in the North-east, four in the South and four in the South-east of the country. The results indicated that digital health increased access to health services in underserved areas, solved cases rapidly and received positive evaluations from all participants. However, the findings revealed that the success of telehealth depended on the health information and communication technology infrastructure, training of health professionals and the organisational readiness of the institutions. Therefore, the health outcomes in middle-income countries are not only dependent on the existence of digital solutions, but also unequal capacity of local systems to absorb the technology.
Evidence from Latin American and other middle-income contexts shows that digital health can improve access to care when it is supported by adequate infrastructure, institutional readiness, digital literacy, and user trust. However, the same literature also warns that digital health may reproduce existing inequalities when connectivity, education, income, and service availability are unevenly distributed across populations. For the present study, this evidence is relevant because Barranquilla, Cartagena, and Santa Marta combine urban health needs with unequal access to household internet and primary care resources. Therefore, the literature is used not to examine gender inequality or Peru as separate analytical cases, but to frame digital access as a socially stratified condition that may shape chronic disease management in middle-income urban settings.
Data Systems, Digital Access, and Health Outcomes in Urban Contexts
The ability to use digital technologies has important health implications. Researchers using data systems to study this issue are able to examine connections between health service utilization including treatment of chronic disease and health outcomes. In Colombia, systems such as the SISPRO platform managed by the Ministry of Health and Social Protection contain data on health service utilization by geographic location, including hospitalizations and diagnoses. In addition, household surveys are conducted to collect data on living conditions, measures of socioeconomic status, and access to technology such as cell phones and the internet. The National Quality of Life Survey (NSQL) conducted by Departamento Administrativo Nacional de Estadística (DANE) collects data on prevalence of chronic disease, health and well-being, health behaviors, health service utilization and other characteristics of households. The data can also be used to study the social determinants of health outcomes.
Digital access indicators provide supplementary information on digital access including digital connectivity, electronic or computer device ownership and internet use, including national ICT surveys that provide information on the digital infrastructure within a country and provide insights into levels of digital inequality across different geographic regions or urban and rural cities and neighborhoods (Departamento Administrativo Nacional de Estadística, 2024b). In this paper we utilise a simplified binary household internet access indicator that assumes connectivity exists irrespective of quality, intensity or relevance to potential health service use.
Integrating digital and health data provides valuable insights to support the goals of population health models that attempt to link the social determinants of health with health outcomes within the context of access to services. This paper describes an urban health research project which utilises a variety of data sets including surveys, administrative data and digital data to understand the complex interactions between a variety of socioeconomic and structural determinants on health outcomes in a context of high socioeconomic inequality. Digital access to health information and care can be considered an intermediate determinant of health outcomes and health interaction with primary care services. In highly unequal cities this interaction is organised mainly through digital channels. This can influence consultation rates, monitoring of patients with chronic conditions and hospital admissions. Combining data from administrative sources and surveys allows for a wide range of questions related to land tenure, taxation, regulatory enforcement, and value to be addressed in urban middle-income countries.
Research Methods
Research Design and Analytical Approach
This research is carried out under a quantitative methodology, with an observational and comparative design. The study is applied in three major metropolitan centers in the Colombian Caribbean: Barranquilla, Cartagena and Santa Marta. With an exploratory purpose, the goal is to establish preliminary evidence of relationships between variables, rather than demonstrating cause and effect. An integrated approach is proposed to analyze the information obtained from household surveys and health registries regarding the prevalence of chronic diseases, in addition to indicators related to the household’s socioeconomic status and access to digital technologies. Analysing data from several sources provides new opportunities to study the relationship between digital access and use of health services.
We employ cross-sectional data and statistics from national sources and administrative datasets to examine the association between digital access and three indicators of chronic disease management in three cities worldwide. Different data sources were used at the country level and harmonized at the city level along with relevant demographic variables. While the data do not allow us to draw conclusions about causality, we can determine which associations are statistically significant. Our aim is to generate preliminary findings that can inform future research intending to establish empirical evidence of causality.
This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guideline for cross-sectional studies, and the completed STROBE checklist has been provided as a supplementary file.
Study Area and Population
The adoption of telemedicine is a promising development in the health sector in Colombia’s Caribbean region. To examine its challenges and opportunities, this study focuses on three medium-sized cities: Barranquilla, Cartagena and Santa Marta. The selected cities present different economic and social contexts, and different degrees of preparedness of the health system. While Barranquilla is the most economically active of the three cities, with the best digital connectivity, Cartagena faces important challenges linked to high socioeconomic inequality, and Santa Marta is a small city lacking robust health infrastructure and great vulnerability. The study focuses on the three cities, which makes it a useful case study in a middle-income country, yet the city-based design of the study has limitations in generalizing the findings. The study population will comprise of adults 18 years and older, with at least one chronic disease identified through household surveys or records of health data. For the purpose of the analysis, only urban households residing in the three cities under study will be included. As a result, findings will only be applicable to the urban subpopulation of the Colombian Caribbean and will not be generalizable to other sectors of the healthcare system, other age groups, rural population or other regions of the country.
Data Sources and Variable Construction
The study is based on secondary data from three official Colombian sources of information. The first source is the National Quality of Life Survey, conducted by the Departamento Administrativo Nacional de Estadística, DANE, which includes closed-response household questionnaire items on self-reported health status, chronic disease, demographic characteristics, education, income, and household access to basic services and technologies. The second source is SISPRO, managed by the Colombian Ministry of Health and Social Protection, which provides administrative health information on consultations, diagnoses, and hospitalizations. The third source consists of national ICT access and household connectivity indicators, also used to characterize digital access across the three cities. Because the study relies on secondary data rather than on a questionnaire administered directly by the researchers, the measurement approach is described through the official survey and administrative indicators used to construct the analytical variables.
Since the study only uses secondary anonymized data, there are no ways to carry out participant recruitment or studies’ surveys. In contrast, the secondary data employed here were collected by official institutions by conducting their own fieldwork. The data were from The National Quality of Life Survey (QNLS), SISPRO’s administrative records and other national ICT indicators and associated studies. In this work, methodological transparency is reflected in the clear exposition of the inclusion criteria and of the data sources, as well as of the data harmonization and the construction of the analytical sample made up of the merged datasets used in the study.
Main Variables Used in the Analysis
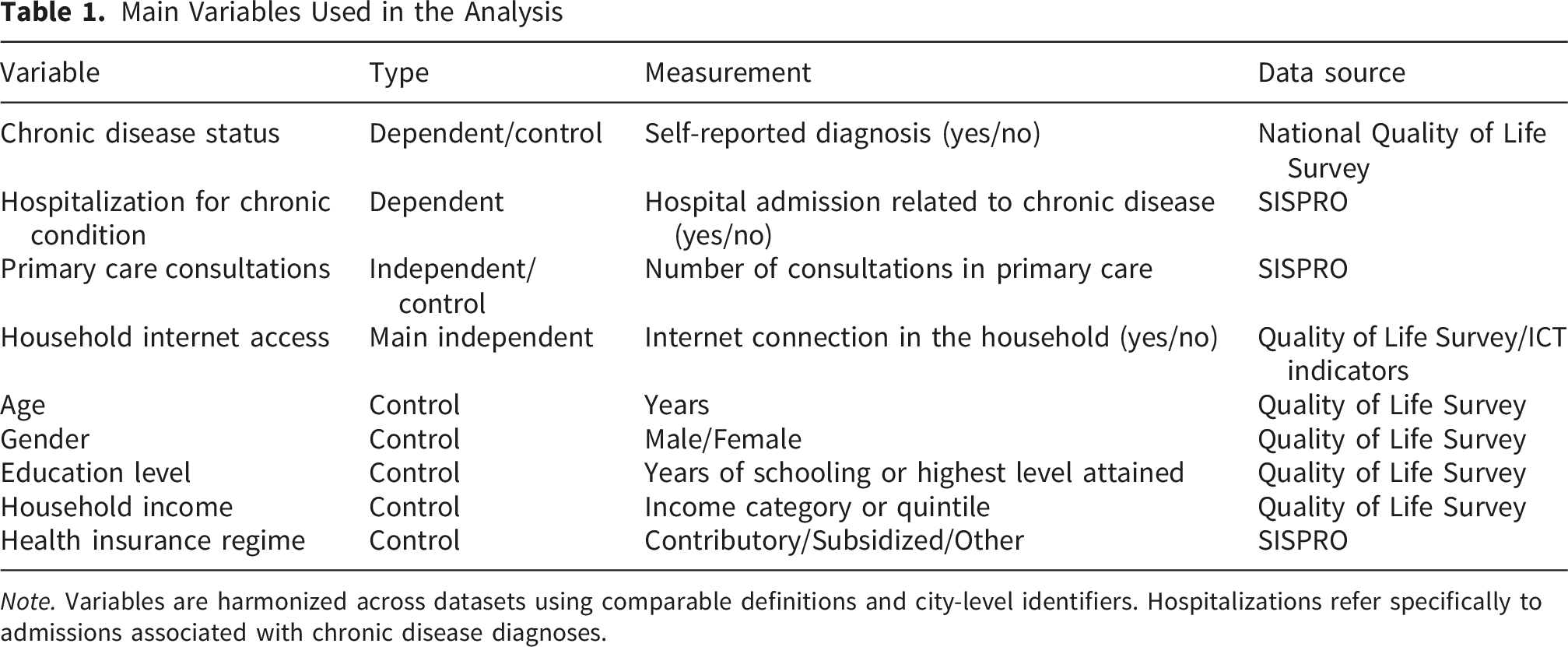
Note. Variables are harmonized across datasets using comparable definitions and city-level identifiers. Hospitalizations refer specifically to admissions associated with chronic disease diagnoses.
Table 1 presents the variables used in the empirical analytical model. The dependent variable measures the probability of hospitalization due to chronic conditions for those with Internet access in the household. The control variables are demographic, socioeconomic and institutional characteristics that may affect both the availability of information technologies and health status.
In this study the studied variables are treated as observed variables. They are based on direct indicators from survey and register data. This means that a reflective measurement model is not suitable here. In consequence, typical reliability and accuracy indicators like composite reliability and average variance extracted cannot be calculated. The goal of the study is to examine the relationships between socioeconomic status and digital media use and several health variables. In contrast to studies employing structural equation modelling (SEM) where multiple indicators measure latent variables, these observed variables are single indicators. This is a common methodological practice. The interpretation of such observed variables differs from the interpretation of latent variables. Issues concerning internal consistency are not relevant for observed variables and, therefore, cannot be evaluated. The typical error of measurement is not relevant for observed variables, too.
Statistical Analysis
Descriptive and inferential statistical techniques were applied to examine the relationship between household digital access and chronic disease management outcomes in the three cities under study. First, descriptive statistics were used to summarize the analytical sample and to compare key variables across Barranquilla, Cartagena, and Santa Marta. Frequencies, percentages, means, and standard deviations were calculated for the principal variables, including household internet access, primary care consultations, hospitalization related to chronic conditions, education, income, and other sociodemographic characteristics. These descriptive results were used to identify preliminary differences across cities and between digitally connected and non-connected households.
Bivariate comparisons were then used to explore differences in primary care utilization according to household internet access status. Average annual primary care visits were compared between individuals living in households with and without internet access, and these comparisons were examined both for the pooled sample and across the three cities. Because the study has an exploratory observational design, these descriptive and bivariate results were interpreted as preliminary patterns of association rather than as evidence of causal effects.
To evaluate the association between digital access and hospitalization related to chronic disease, the main multivariable analysis used a binary logistic regression model. The dependent variable was coded as 1 when the individual experienced hospitalization related to chronic disease and 0 otherwise. The main independent variable was household internet access, measured as a dichotomous indicator. The model included age, gender, education, income quintile, health insurance regime, and city fixed effects as control variables in order to account for observable demographic, socioeconomic, and contextual differences across individuals and cities. Regression coefficients from the logistic model were interpreted through odds ratios, and predicted probabilities were also estimated to facilitate substantive interpretation of the results.
As a robustness check, an additional probit regression model was estimated using the same dependent variable and the same set of covariates. This alternative specification allowed assessment of whether the direction and statistical significance of the main association remained stable under a different link function. The estimation sample was restricted to complete cases with non-missing values for the dependent variable and all covariates included in the multivariable models. Statistical results were reported using coefficients or odds ratios, standard errors, p-values, marginal effects where appropriate, model fit indicators, and the number of observations. To improve transparency and reproducibility, all regression results were reported with 95% confidence intervals in addition to coefficients or odds ratios, standard errors, p-values, model fit indicators, and the number of observations. For the logistic model, confidence intervals were calculated around the odds ratios, while the probit specification reported confidence intervals for both coefficients and marginal effects where appropriate. This consistent reporting allows readers to assess not only statistical significance but also the precision and plausible range of the estimated associations.
Econometric Model
We employ a logistic regression model to estimate the probability of hospitalization of chronic diseases. The dependent variable equals one if a person is hospitalized because of chronic diseases in the year of observation and zero if not. We predict the following probability: The probability of hospitalization of individual i in the year of observation P(Hi=1) = 1/(1+e^(β0+β1* Digital_i + β2* X_i + β3* City_i)), where Digital_i equals one if household i has access to the internet and zero otherwise, X_i are control variables including different demographic and socioeconomic measures, and City_i capture city fixed effects.
The logistic regression can also be expressed in log-odds form. Equation 2 presents the linear relationship between household digital access, control variables, city fixed effects, and the log-odds of hospitalization related to chronic disease:
Equation 2. Logistic regression in log-odds form

In this equation,
Digital connectivity is treated as a structural condition that may be associated with more frequent contact with primary health care providers. However, the present model does not formally test whether primary care utilization mediates the relationship between household internet access and hospitalization. For that reason, the proposed pathway linking digital access, primary care engagement, and lower hospitalization risk is interpreted as a theoretically plausible mechanism rather than as an empirically demonstrated causal pathway. Prior evidence on teleconsultation, remote monitoring, and digital health communication supports the idea that digital tools may facilitate early detection, adherence, and follow-up among patients with chronic conditions, but the present cross-sectional design only estimates conditional associations. A logistic functional form is therefore appropriate for modelling the association between household internet access and the probability of hospitalization, while avoiding causal claims about the mechanism.
The model includes city fixed effects to control for unobserved city-specific structural differences. Potential differences in physical infrastructure, availability and quality of health care services, demographic composition, socioeconomic conditions, and digital connectivity across Barranquilla, Cartagena, and Santa Marta may affect both household internet access and the risk of hospitalization related to chronic conditions. By controlling for these city fixed effects, the estimated association between digital access and hospitalization risk is interpreted within the urban Colombian Caribbean context rather than as a generalized effect across unrelated settings.
Model Specification, Missing Data Handling, and Statistical Reporting
To improve reproducibility, the statistical specification of the baseline model should be stated more explicitly. The main analysis estimates a binary logistic regression in which hospitalization related to chronic disease is modeled as a function of household internet access, age, gender, years of education, income quintile, insurance regime, and city fixed effects. The dependent variable is coded as a dichotomous outcome, and the principal coefficient of interest corresponds to the odds ratio associated with household internet access, conditional on the full set of covariates. The complementary probit model reported later in the manuscript uses the same dependent variable and the same covariate structure, so that differences across specifications reflect the estimation link function rather than changes in model composition. This clarification makes clear that the core specification is stable across models and that the robustness exercise is directly comparable to the baseline analysis.
Additional clarification is also needed regarding the treatment of missing data. Because the study integrates survey-based and administrative sources, some observations may be affected by incomplete reporting across demographic, socioeconomic, or digital access variables. In the present analysis, the estimation sample should therefore be described as based on complete cases with non-missing values for the dependent variable and all covariates included in the multivariable model. This choice improves internal consistency across the regression estimates, but it may also reduce sample size and introduce selection concerns if missingness is not random. For that reason, the manuscript should explicitly state the final analytical sample used in each model and acknowledge that the findings are conditional on available complete information rather than on imputed values or partially observed records.
Finally, the reporting of regression results should be expanded to include confidence intervals in addition to standard errors and p-values. For the logistic model, reporting 95% confidence intervals around odds ratios would allow readers to assess both statistical precision and the plausible range of the estimated association. The same principle applies to the probit specification and to the reported marginal effects, where confidence intervals would improve comparability across models and strengthen interpretive transparency. Presenting these intervals alongside coefficients, standard errors, p-values, model fit indicators, and the number of observations would make the empirical strategy easier to replicate and would align the results section more closely with standard reporting expectations for observational health research.
Ethical Considerations and Data Limitations
The study only uses secondary data from a variety of national surveys and administrative health data sources. The secondary data used in this study is anonymized and de-identified, such that no personally identifiable information is present. The study does not involve any interaction with individuals or clinical interventions; therefore, there is no issue regarding informed consent or patient safety.
The analysis is based on anonymised secondary data and follows standard ethics in health systems research such as maintenance of confidentiality, proper handling of data and transparent communication of methods and findings. The secondary data used here is a national dataset of anonymised data that was originally collected by official bodies as part of their role, within ethical protocols at the time of data collection. The study utilises national administrative and survey data; as such it has good external validity and reflects real patterns of service use. Administrative data from systems such as SISPRO that record all actual consultations, diagnoses and hospitalisations can be used to analyse the disease management and care of people with chronic health conditions. There is a growing body of research on integrated chronic care systems that has shown the potential of using such data to assess aspects of patient-centred care, and systems’ performance. This study uses such data sources to explore issues in primary care management of people with diabetes.
This analysis contains several limitations. First, the data used are cross-sectional and therefore cannot be used to establish causality. Second, the logistic model used here estimates only the association between digital access and the probability of hospitalization, conditional on the control variables included in the model, such as income, health status, older age, and urban residence. There may also be unobserved variables correlated with both digital access and health outcomes, such as health literacy or the quality of local health services. Common indicators of chronic disease prevalence based on survey data often rely on self-reported information about physician-diagnosed conditions, which introduces the risk of recall bias or underreporting. Administrative data, by contrast, provide information on individuals who come into contact with the health system but do not capture undiagnosed cases. Early studies on telemedicine adoption and digital barriers in health care further suggest that both technological and social factors must be considered when interpreting the available datasets.9,11
Endogeneity, Reverse Causality, and the Limits of Cross-Sectional Inference
The model specifies only conditional associations between household internet access and hospitalization for chronic diseases. Because the data have a cross-sectional design, no inference can be made regarding the temporal sequence between household internet access and lower rates of hospitalization for chronic diseases. Therefore, these coefficients should not be interpreted as indicating that access to digital technologies has a positive, unidirectional effect on chronic disease management. Instead, residents of healthier households with more stable socioeconomic conditions may be more likely to have internet access at home. Accordingly, the findings should be interpreted as conditional on household internet access.
Individuals or households with a greater chronic disease burden, more complications, or more prior health care experience may also be more likely to obtain internet access or use health-related digital tools and communication technologies because of their health care needs. In turn, prior health status could explain the observed associations between connectivity and hospitalization. In other words, prior health status may act as an unobserved predictor of both connectivity and health-related digital use, thereby distorting the estimated relationship between digital connectivity and health outcomes. This concern has been raised in prior studies on digital health adoption.7,8
Variables not included in the SHCA data, such as health literacy, household organization, severity of chronic conditions, physical distance from providers, quality of primary care, and availability of informal caregivers, are also shaped by socioeconomic and institutional advantages that do not necessarily depend on digital access. Although the findings of this model are intended as illustrative evidence, full disclosure of these limitations is essential. Future research would benefit from longitudinal data, panel data, and quasi-experimental designs, including instrumental variable approaches, to address endogeneity more directly.2,4,10
Despite the challenges involved in merging administrative and survey data, using such sources allows an exploratory analysis of the relationship between digital access and the difficulties faced by people with chronic diseases in managing their health, as well as the relationship between digital connectivity and hospitalization risk. The model specified below represents a probabilistic relationship between digital connectivity and hospitalization risk, and the estimates should be interpreted as exploratory evidence. A major limitation is that household internet access is measured as a simple binary variable, that is, whether connectivity exists in the household, rather than through more nuanced indicators such as digital literacy, frequency of internet use, device quality, connection stability, or actual telehealth use. Therefore, the estimates capture some, but not all, dimensions of digital access relevant to chronic disease management. Despite the challenges involved in merging administrative and survey data, using such sources allows an exploratory analysis of the relationship between digital access and the difficulties faced by people with chronic diseases in managing their health, as well as the relationship between digital connectivity and hospitalization risk. The model specified in this study represents a probabilistic association between digital connectivity and hospitalization risk, and the estimates should be interpreted as exploratory evidence. A major limitation is that household internet access is measured as a simple binary variable, that is, whether connectivity exists in the household, rather than through more nuanced indicators such as digital literacy, frequency of internet use, device quality, connection stability, or actual telehealth use. Therefore, the estimates capture some, but not all, dimensions of digital access relevant to chronic disease management. Future research using longitudinal data and richer measures of digital use could clarify the mechanisms driving these associations. In particular, formal mediation analysis should be treated as a priority for follow-up research to determine whether primary care utilization explains part of the association between household digital access and hospitalization outcomes. Future studies could also incorporate direct self-reported telehealth use in addition to administrative claims data to better explain the relationship between health information technology use and health outcomes.
Results
Descriptive Profile of the Study Population
Analytical Sample by City and Household Digital Access Status
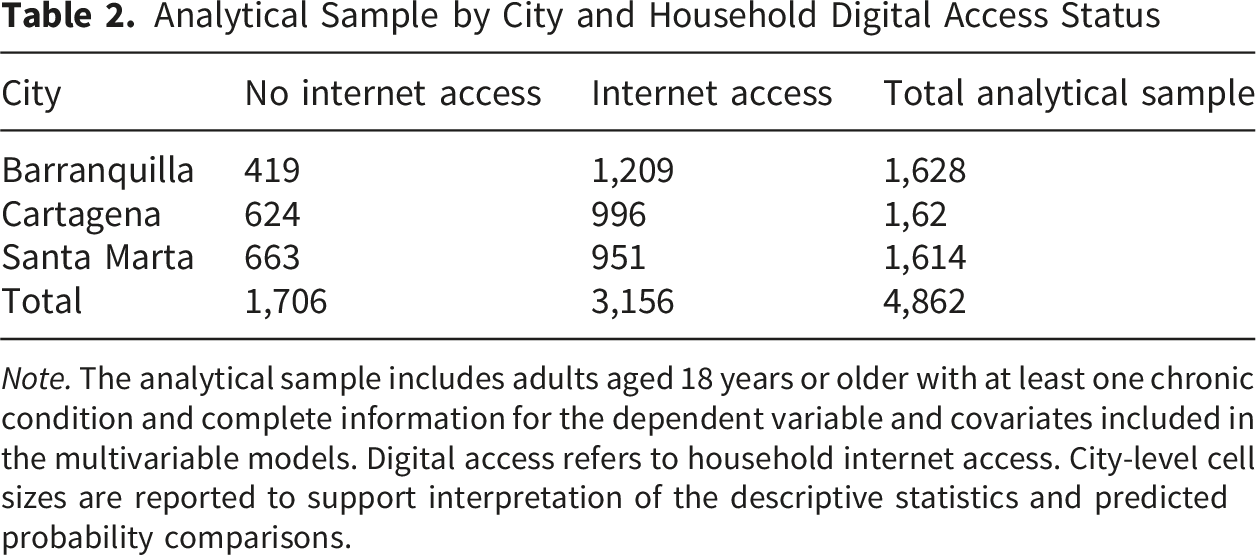
Note. The analytical sample includes adults aged 18 years or older with at least one chronic condition and complete information for the dependent variable and covariates included in the multivariable models. Digital access refers to household internet access. City-level cell sizes are reported to support interpretation of the descriptive statistics and predicted probability comparisons.
As shown in Table 2, the final analytical sample is relatively balanced across the three cities, with 1,628 observations from Barranquilla, 1,620 from Cartagena, and 1,614 from Santa Marta. The distribution by household digital access status also shows sufficient cell sizes for city-level descriptive comparisons and predicted probability estimates. Barranquilla has the largest digitally connected subsample, while Santa Marta has the largest non-connected subsample, reflecting the city-level differences in household internet access described in the descriptive results.
Barranquilla has the highest prevalence of household internet access and highest average income, followed by Cartagena and then Santa Marta where the majority of households are in the lowest income quintile. Large between-city differences exist in terms of self-reported internet access for the individuals in the sample. On average, approximately two-thirds of the individuals in the analytical sample reported having internet access at home. The data reflect considerable variation in the digital environment in the Caribbean region of Colombia. This initial analysis allows for some preliminary commentary regarding the extent to which digital resources may be unequally distributed to populations with chronic health needs.
Descriptive Statistics by City

Note. Percentages and averages are calculated for individuals with at least one chronic condition. Values are harmonized across survey and administrative datasets.
The figures in Table 3 illustrate a consistent pattern: cities with higher digital access also show higher primary care consultation rates and lower hospitalization rates. Although these differences are descriptive, they provide an initial empirical context for the regression analysis that follows.
Digital Access and Primary Care Utilization
We also present findings on the association between internet access at the household level and the use of primary health care services. On average, those who have internet access in the households where they reside have more primary care consultations than those who do not have access. On average, respondents with internet access report 0.95 more primary care visits over the past year than those without internet access. These differences are observed in all three cities. The difference is largest in Barranquilla and smallest in Santa Marta.
Primary Care Visits by Digital Access Status

Note. Values represent average annual primary care visits among individuals with chronic conditions.
The results in Table 4 indicate a clear difference in primary care utilization between digitally connected and non-connected households. While these results are descriptive, they support the hypothesis that digital access may be associated with greater engagement with primary care services.
Logistic Regression Results: Digital Access and Hospitalization
Using harmonized household, administrative health, and ICT-related data from Barranquilla, Cartagena, and Santa Marta in the Colombian Caribbean, the study employs logistic regression to examine the association between household digital access and hospitalization related to chronic disease. In addition to household internet access, the model controls for demographic, socioeconomic, insurance-related, and city-level factors. The results indicate that individuals living in households with internet access have lower odds of hospitalization than those without access, with the odds ratio for digital access below one. This finding is consistent with the study hypothesis, but it should be interpreted as a conditional association rather than as evidence of a causal effect.
Logistic Regression Results for Hospitalization
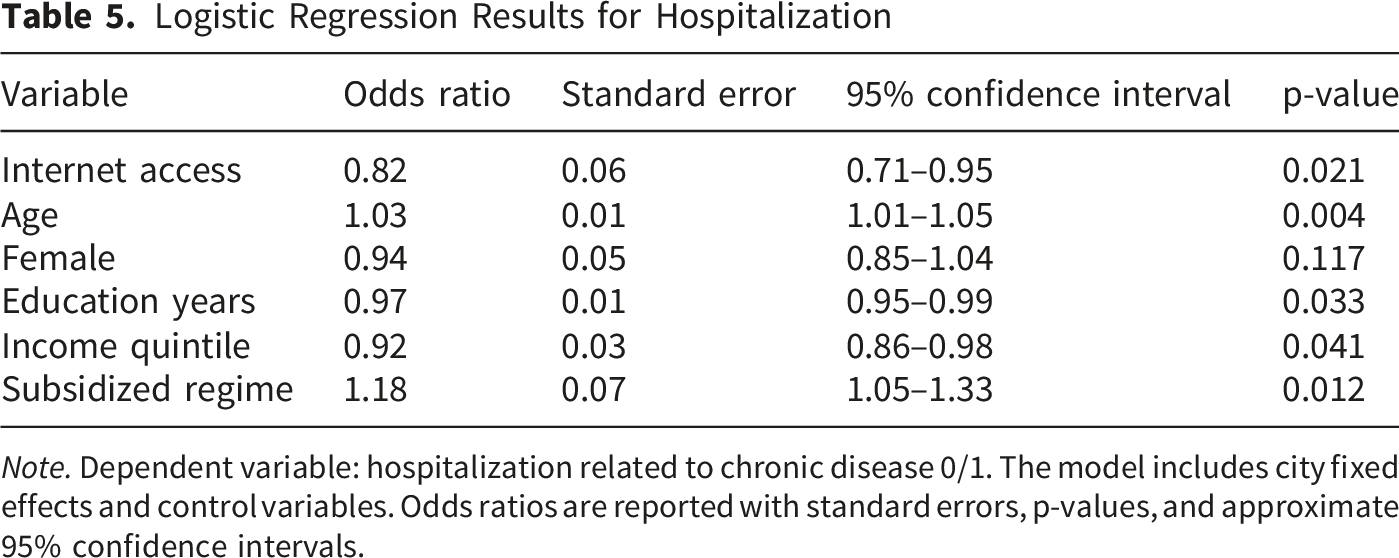
Note. Dependent variable: hospitalization related to chronic disease 0/1. The model includes city fixed effects and control variables. Odds ratios are reported with standard errors, p-values, and approximate 95% confidence intervals.
The results indicate that individuals with household internet access had 18% lower odds of hospitalization for chronic conditions, after adjusting for age, gender, education, income quintile, insurance regime, and city fixed effects. This association should be interpreted cautiously because the study does not identify the specific mechanism explaining the difference. Household internet access was measured as a simple binary indicator, and the analysis cannot distinguish whether the association reflects basic connectivity, digital literacy, quality of devices, stability of internet service, telehealth use, or other unobserved socioeconomic advantages. Accordingly, the result should be presented as evidence of a modest conditional association rather than as proof of improved chronic disease management caused by digital access.
Predicted Probabilities and City-Level Comparisons
To further interpret the results of the regression analyses, predicted probabilities of hospitalization among individuals with household internet access and those without household internet access were calculated using the logistic regression coefficients from the models.
The predicted probability of hospitalization for those without internet access is higher for the 2000 poor individuals surveyed in three cities in Colombia. The difference between the predicted probability of the individuals with internet access and those without access is not large, but it is positive and robust across the three locations. The largest difference between those with and without access is found in Santa Marta, a location with the lowest level of digital access in the sample. City-level results suggest that the relationship between digital access and likelihood of hospitalization may be affected by a variety of factors including the quality of primary health care and the quality of the digital infrastructure within each city.
Predicted Probability of Hospitalization by Digital Access
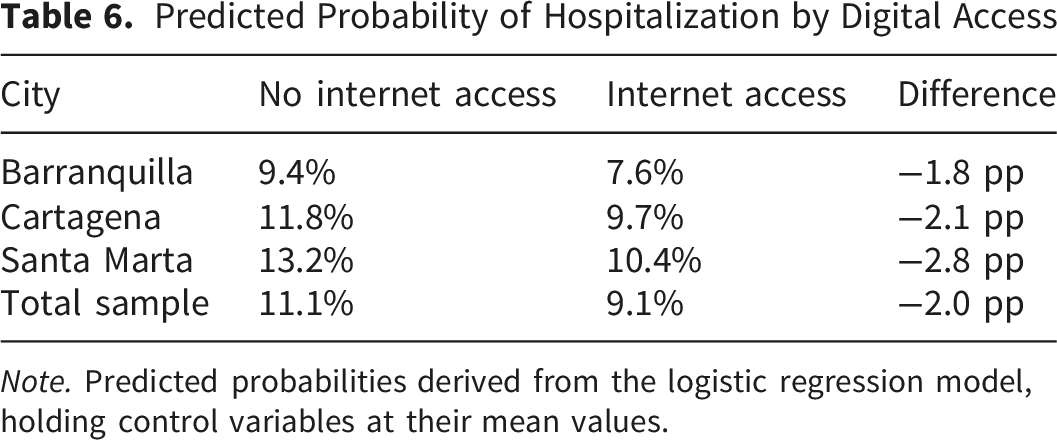
Note. Predicted probabilities derived from the logistic regression model, holding control variables at their mean values.
Table 6 shows that individuals with household internet access consistently exhibit lower predicted probabilities of hospitalization across all three cities. While the differences are not large, the direction of the association is consistent with the study’s hypothesis. These results provide preliminary evidence that digital connectivity is associated with chronic disease management outcomes across the three cities. Although descriptive differences in primary care utilization are consistent with a possible pathway linking digital access to more frequent engagement with primary care services, this mechanism was not formally tested within the regression framework. Accordingly, the role of primary care utilization should be interpreted as a theoretically plausible explanation rather than an empirically identified mediating pathway in the present study.
Robustness Check: Alternative Model Specification
In order to test the robustness of the findings from the logistic regression, an alternative econometric specification was also estimated using a probit model. The probit model is similar to the logistic regression model employed in the paper but makes the alternative assumption that the error terms are normally distributed rather than logistically distributed. Therefore, an alternative test of the direction and significance of the relationship between digital access and hospitalization can be obtained under an alternative functional form.
In developing the robustness test, we employ a probit specification. The probit model includes the same independent variables as the logistic regression - whether a household has Internet access, age, gender, education, income, insurance regime and city fixed effects - but switches to a probit specification with the same dependent variable - whether a household hospitalizes due to a chronic condition - as was used in the logistic regression estimates. The use of this test allows us to investigate whether the method of estimation affects the results while keeping everything else constant.
Probit Regression Results for Hospitalization (Robustness Check)

Note. Dependent variable: hospitalization related to chronic disease 0/1. The probit specification includes the same control variables and city fixed effects as the baseline logistic model. Marginal effects are evaluated at sample means. Coefficients are reported with standard errors, p-values, and approximate 95% confidence intervals.
The probit results are in the expected direction and remain statistically significant, confirming the stability of the main association under an alternative binary-response specification. The marginal effect indicates that, holding the included covariates constant, individuals living in households with internet access have an estimated 2.1 percentage point lower probability of hospitalization. This result is consistent with the logistic model and the predicted probability analysis. However, it should still be interpreted as robustness evidence for the association, not as confirmation of a causal effect or a formally tested mediation pathway.
Discussion
Digital Access as a Structural Determinant of Chronic Disease Management
The results of this study suggest a consistent preliminary association between household digital access and lower probabilities of hospitalization among individuals with chronic conditions. Although the analysis is exploratory and does not establish causality, the direction of the findings aligns with theoretical models that conceptualize digital connectivity as an enabling factor for continuous and coordinated care. In primary care-centered systems, the ability to communicate with providers, receive reminders, and access health information plays a critical role in treatment adherence and early intervention. Digital access, in this sense, can be understood as a structural determinant that shapes how individuals interact with the health system.
These findings are consistent with research showing that information and communication technologies support self-management processes among patients with chronic diseases. For example, studies on older adults with comorbidities demonstrate that ICT use is associated with improved disease monitoring and more effective self-care behaviors, suggesting that digital access may influence health outcomes through behavioral pathways. 12 Such mechanisms are particularly relevant in urban environments where digital infrastructure varies across neighborhoods and social groups. 13
The observed association between digital access and primary care utilization is consistent with theoretical perspectives that emphasize continuous interaction between patients and providers in chronic disease management. Routine consultations, monitoring, and timely treatment adjustments remain central to patient-centered and integrated chronic care models, and digital tools may help reduce logistical barriers or improve communication channels.2,3,5 Nevertheless, this interpretation must remain cautious. Primary care utilization was not formally modeled as a mediator or intervening variable, and the cross-sectional design does not allow the study to determine whether digital access leads to lower hospitalization through greater primary care engagement. The pathway should therefore be described as theoretically plausible and consistent with prior research on chronic care, digital health interventions, and ICT-supported self-management, but not empirically tested in the present analysis.5,12
At the same time, the findings highlight the importance of considering digital access not only as a technological variable but also as a social determinant of health. Differences in connectivity may reflect broader socioeconomic inequalities that influence access to health services. Studies on digital health adoption emphasize that technology alone does not produce better outcomes; rather, its impact depends on how it interacts with existing social and institutional structures. 11
In this sense, the results contribute to the growing body of literature that frames digital connectivity as part of the broader infrastructure surrounding primary care systems. Rather than being an isolated innovation, digital access may function as a complementary component of patient-centered care models that support communication, follow-up, and self-management.3,11 At the same time, the present findings do not allow us to verify whether more consistent engagement with primary care services is the mechanism linking digital access to lower hospitalization probabilities. For that reason, any indirect health benefit associated with digital inclusion should be presented as a theoretical interpretation supported by previous literature, not as an empirically identified mediating pathway within this study.5,12
Urban Inequalities, Digital Divides, and Health System Performance
One of the most relevant findings of the study is the variation observed across cities with different levels of digital connectivity and socioeconomic conditions. The descriptive and regression results suggest that cities with higher levels of digital access also tend to show lower hospitalization probabilities among patients with chronic conditions. Although these differences are modest, they point to the possibility that digital infrastructure may influence health system performance at the urban level.
Urban health research has long emphasized the role of structural inequalities in shaping access to services and health outcomes. In many middle-income contexts, cities exhibit sharp internal disparities in income, education, and infrastructure. Digital connectivity often follows these same patterns, with higher-income neighborhoods enjoying better access to internet services and digital tools. As a result, digital health innovations may reinforce existing inequalities if access remains uneven across populations.
Research on telemedicine adoption highlights how socioeconomic factors influence the uptake and effectiveness of digital health services. Systematic reviews have identified barriers such as limited infrastructure, lack of digital literacy, and institutional resistance as key obstacles to widespread adoption. 9 These barriers are particularly relevant in urban areas with high levels of inequality, where some groups may benefit more from digital health innovations than others.
Similarly, studies on eHealth adoption among providers emphasize the importance of organizational readiness, training, and institutional support. The successful integration of digital tools into primary care depends not only on technological availability but also on provider acceptance and workflow integration. 7 These factors may vary across cities and may influence the effectiveness of digital health strategies. For that reason, the findings of this study should be interpreted cautiously. In Barranquilla, Cartagena, and Santa Marta, higher levels of digital connectivity are associated with modestly lower probabilities of hospitalization among individuals with chronic conditions. This pattern suggests that digital inclusion may complement broader primary care and inequality-reduction strategies, but it does not support broad claims about large system-wide effects. At the same time, the results may still be relevant for other middle-income urban settings that face similar problems of fragmented access, uneven infrastructure, and internal social inequality. Any such comparison, however, should be made cautiously and with attention to local institutional differences.
Policy Implications for Primary Care–centered Digital Strategies
The preliminary associations identified in this study carry cautious implications for health policy in the three cities under analysis. The results indicate a modest association between household internet access and lower hospitalization risk, suggesting that digital connectivity may complement, but not substitute for, broader primary care strengthening efforts. For that reason, the policy relevance of the findings should be framed proportionately: the observed effect size is meaningful enough to justify attention to digital inclusion as one supporting dimension of chronic disease management, but not strong enough to support claims that connectivity expansion alone would substantially reduce hospitalizations. Any policy interpretation should therefore emphasize incremental and context-specific gains rather than large-scale expected effects.
Patient-centered care frameworks also provide a useful lens for interpreting these findings. Research on chronic illness care indicates that patient perceptions of coordinated, accessible services are linked to better outcomes and higher levels of treatment adherence. 2 Digital tools may enhance these perceptions by making services more accessible and responsive to patient needs. In this way, digital connectivity can contribute to the operationalization of patient-centered care principles. Moreover, studies on the challenges faced by primary care practitioners highlight the importance of organizational support and resource allocation in chronic disease management. Primary care providers often operate under resource constraints, which can limit their ability to offer continuous and coordinated care. 4 Digital tools may alleviate some of these pressures by streamlining communication, facilitating remote monitoring, and improving information flow between patients and providers.
The broader health system context also matters. Evidence from pandemic-related digital health interventions shows that digital platforms can expand access to care and support public health responses, but their effectiveness depends on infrastructure, governance, and user readiness. 10 These lessons suggest that digital strategies should be integrated into broader health system reforms rather than implemented as isolated technological solutions. In this sense, the present findings support modest and context-sensitive policy considerations: expanding internet access, improving digital literacy, and integrating telehealth services into primary care networks may contribute to chronic disease management, but such measures should be understood as complementary rather than decisive interventions. Moreover, because the evidence is limited to three Caribbean Colombian cities, the external validity of these implications is necessarily bounded. Additional research in other urban and non-urban settings would be needed before extending these conclusions to Colombia as a whole or to middle-income contexts more broadly.
Conclusion
Improved communication, access to health information, appointment management, and patient-provider interaction may help explain why household internet access is associated with greater primary care use and lower hospitalization probabilities.2,3,5,12 However, these mechanisms were not formally tested in the present study. In particular, the possible mediating role of primary care utilization in the relationship between digital access and hospitalization remains theoretical. Future studies using longitudinal data, direct measures of telehealth use, and formal mediation models are needed to determine whether digital access improves chronic disease outcomes through stronger engagement with primary care services. 12
Supplemental Material
Supplemental Material - Digital Access and Primary Care Use in Chronic Disease Management: Preliminary Evidence From Three Caribbean Cities in Colombia
Supplemental material for Digital Access and Primary Care Use in Chronic Disease Management: Preliminary Evidence From Three Caribbean Cities in Colombia by Mario de la Puente, Hernán Guzmán, Denis Adriana González Sánchez, Anderson Domínguez, Juan Lamby in INQUIRY: The Journal of Health Care Organization, Provision, and Financing.
Footnotes
Acknowledgement
The authors thank their respective institutions for providing academic support and access to research resources. The authors also acknowledge the national statistical and administrative agencies of Colombia for making the datasets used in this study publicly available.
Ethical Considerations
This study uses anonymized secondary data from national surveys and administrative records. No direct human participation or identifiable personal data were involved. Therefore, formal ethical approval was not required according to institutional and national guidelines for secondary data research.
Consent to Participate
The study is based on anonymized secondary datasets.
Author Contributions
M.D.L.P. contributed to the conceptualization of the study, research design, methodology, formal analysis, interpretation of results, supervision, and writing of the original draft. H.G. contributed to conceptual support, interpretation of results, and writing–review and editing. D.A.G.S. contributed to data collection and contextual interpretation. A.D. contributed to data collection, data curation, and writing–review and editing. J.L. contributed to investigation, data validation, and writing–review and editing. All authors reviewed and approved the final version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data used in this study are derived from publicly available national surveys and administrative records. Data are available upon reasonable request to the corresponding author, Mario de la Puente.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.