
Abstract
Introduction
Self-compassion has demonstrated substantial advantages in regulating anxiety and depression across diverse population groups. Nevertheless, conventional methods for augmenting self-compassion are dependent on an individual’s imaginative faculties. Virtual reality presents a novel avenue for self-compassion intervention. But these interventions vary considerably in their types, session duration and frequency, and outcome assessment measures. This scoping review integrates evidence regarding the application of virtual reality (VR) in self-compassion interventions, with the aim of providing information and guidance for future clinical implementation.
Methods
We conducted a systematic search of ten databases, including PubMed, Web of Science, Embase, PsycINFO, Scopus, the Cochrane Library, CINAHL, CNKI, Wanfang, and VIP. The search period extended from the inception of the databases to November 4, 2025. All the included studies met the eligibility criteria.
Results
Sixteen studies were included. Interventions were classified as non-interactive virtual reality (VR) self-compassion interventions and interactive interventions involving virtual scenes or characters. Non-interactive VR has a low usage threshold, making it suitable for most individuals. Scene-based interactive interventions are brief and allow simple interactions, suiting those with short attention spans. Character-based interactive interventions promote deeper emotional engagement but require more complex operations, fitting individuals with marked self-conflict and high cooperation. Although effects varied by intervention type, an overall positive trend was observed. Participants demonstrated good adherence and favorable user experiences; several studies also adopted strategies to enhance adherence.
Conclusion
VR-based self-compassion interventions fall into non-interactive and interactive types, each differing in technical features and target populations. Overall, these interventions effectively enhance self-compassion, and participants generally show high acceptance. However, most studies have methodological limitations. Therefore, the conclusions require further validation through high-quality, large-sample randomized controlled trials that also monitor long-term intervention effects.
1. Background
In recent years, the prevalence of emotional disorders such as anxiety and depression has risen markedly. 1 As a crucial psychological resource for emotion regulation, self-compassion is being gradually recognized. 2 Self-compassion is generally defined as a self-acceptance attitude while facing failure or personal distress. It encourages people to acknowledge and accept negative experiences, offering kindness and support to oneself, but not to avoid them or engage in self-criticism. 3 Research demonstrates that higher levels of self-compassion significantly mitigate anxiety and depression in diverse groups, including students, adults, 4 patients with mental disorders, 5 cancer, 6 or chronic diseases. 7 Neuroscience research further suggests that greater self-compassion is correlated with decreased functional connectivity between the prefrontal cortex and the amygdala, 8 as well as enhanced psychological resilience under stress. 9 Consequently, self-compassion is regarded as a key protective factor that may buffer against the onset of anxiety and depression, potentially reducing the latent risk of more extensive psychopathology. 10
However, empirical evidence suggests that self-compassion generally remains suboptimal across diverse populations and is persistently correlated with unfavorable psychological and clinical consequences. In non-clinical populations, students 11 and adults 12 often confront academic or occupational stressors and may lack effective strategies for emotion regulation, which can lead to an increase in self-criticism. Among clinical populations, individuals suffering from mental disorders typically report low levels of self-compassion, 13 which is significantly associated with suicidal and non-suicidal self-injury. 14 For patients diagnosed with cancers such as breast cancer 15 and lung cancer, 16 the prolonged disease course and prognostic ambiguity result in a chronic exhaustion of psychological resources. This chronic depletion undermines the capacity for self-compassion, thereby notably reducing treatment adherence. 17 Similarly, for patients with chronic diseases, inadequate symptom management can initiate debilitating cycles of self-criticism, which subsequently impair medication adherence and self-management capabilities. 18 Therefore, it is of urgent necessity to implement effective measures to enhance self-compassion ability.
Traditional methodologies, encompassing mindfulness-based compassion meditation, 19 two-chair dialogue therapy, 20 and compassion-focused therapy (CFT), 21 have obtained empirical validation for their effectiveness in augmenting self-compassion. Nevertheless, during the implementation phase, traditional methodologies predominantly depend on an individual’s imaginative faculty, rendering it arduous to ensure the stability of the intervention outcomes. Virtual reality (VR) technology is capable of generating immersive three-dimensional environments through the integration of multi-sensory simulations, such as visual, auditory, and tactile stimuli, 21 thereby constructing highly realistic simulated situations. This enables participants to immerse themselves in virtual settings or embody specific roles without relying on their own imaginative capabilities. 22 Consequently, an increasing volume of research has investigated VR as a novel medium for self-compassion interventions, yielding preliminary evidence of its efficacy. 10 The systematic review by Žilínský et al 23 examined the positive effects of virtual reality (VR) on enhancing self-compassion. However, a systematic synthesis of implementation types, target population characteristics, type-specific intervention effects, and participant acceptability is lacking, which limits clinical translation.
This scoping review aims to delineate the technical types, target populations, and effects of existing interventions, assess acceptability, and summarize strategies used to improve adherence. It may also inform the design of more rigorous and effective interventions, ultimately fostering greater self-compassion and sustainable mental health.
2. Methods
This scoping review followed the PRISMA-ScR (Preferred Reporting Items for Systematic Reviews and Meta - Analyses extension for Scoping Reviews) 24 checklist framework to direct its implementation and reporting. The checklist for this review can be found in Appendix A. Moreover, the review protocol was registered with the Open Science Framework (DOI: 10.17605/OSF.IO/3NQVU).
2.1. Research Questions
The review addressed the following questions: (1) Based on interactivity, what types of VR interventions can be distinguished, and in which populations have they been applied? What are the typical intervention duration and frequency? (2) What outcome measures and assessment tools have been used, and what effects have been observed? (3) How acceptable is VR technology to participants, and what strategies can enhance adherence?
2.2. Eligibility Criteria
The inclusion criteria for this scoping review were formulated using the PCC (Population, Concept, Context) framework. The specific criteria are as follows:
P (Population): The study population was unrestricted, including individuals from any demographic or clinical background.
C (Concept): The core concept was the utilization of VR technology in self-compassion interventions. This incorporated both interactive and non-interactive immersive VR technologies.
C (Context): The context encompassed any setting where VR technology could be realistically applied, such as hospitals, community health centers, or other health-related environments.
S (Source Type): randomized controlled trials, non-randomized controlled trials, mixed methods studies, and qualitative studies.
Excluded criteria are as follows: ①The research was presented in the form of a review, conference abstracts, and study protocols; ②Publications were in languages other than Chinese or English; ③The full text could not be retrieved; ④Duplicate publications.
2.3. Search Strategy
Systematic searches were carried out across ten databases, including PubMed, Cochrane Library, Web of Science, CINAHL, Embase, Scopus, PsycINFO, CNKI, VIP, and Wanfang Data. The search strategy combined subject headings and free-text keywords to enhance sensitivity, covering the period from the inception of each database to November 4, 2025. Additionally, the reference lists of all included studies were manually screened, and backward citation tracking was conducted to identify additional relevant publications. The complete search strategies for all databases are available in Appendix B.
2.4. Selection of Sources of Evidence
After duplicate removal in End Note 21, two reviewers trained in systematic review methodologies independently conducted an initial screening of titles and abstracts. Subsequently, the full-text articles of potentially eligible studies were retrieved and independently evaluated by the two reviewers for final eligibility. Any discrepancies that emerged during the screening process were resolved through discussion and reaching a consensus with a third reviewer. Similarly, data extraction from the included studies was independently carried out by the two reviewers, and any disagreements were resolved through consultation with the third reviewer.
2.5. Quality Assessment
The methodological quality of the included studies was evaluated using the Mixed Methods Appraisal Tool (MMAT). 25 The MMAT is a validated instrument designed for assessing diverse study designs. For each study category, the MMAT consists of five specific criteria that address key methodological domains; each criterion is rated as “Yes,” “No,” or “Unclear”. 25 Two independent reviewers conducted the assessments. Their results were compared, and discrepancies were resolved through discussion and consensus with a third reviewer.
2.6. Data Extraction
Following the literature selection procedure, two reviewers independently developed a standardized data extraction. The entries were then cross verified for accuracy, resolving any discrepancies through discussion and reaching a consensus with a third reviewer. The data extracted to address the review questions included: first author, publication year, country, study design, population characteristics and sample size, technology type, intervention details (duration, frequency), and outcome measures.
3. Results
3.1. Literature Screening Results
A total of 344 records were retrieved from the database searches. After the removal of duplicates and the screening of titles and abstracts, 45 articles were subjected to full-text review. Among these, 16 studies satisfied all the eligibility criteria for inclusion. No additional studies were discovered through the manual searches of reference lists or citation tracking. A systematic search of three Chinese databases yielded no eligible studies, likely because VR-based self-compassion research remains in its early stages in China. The selection process is presented in detail in Figure 1. Flowchart of the study selection process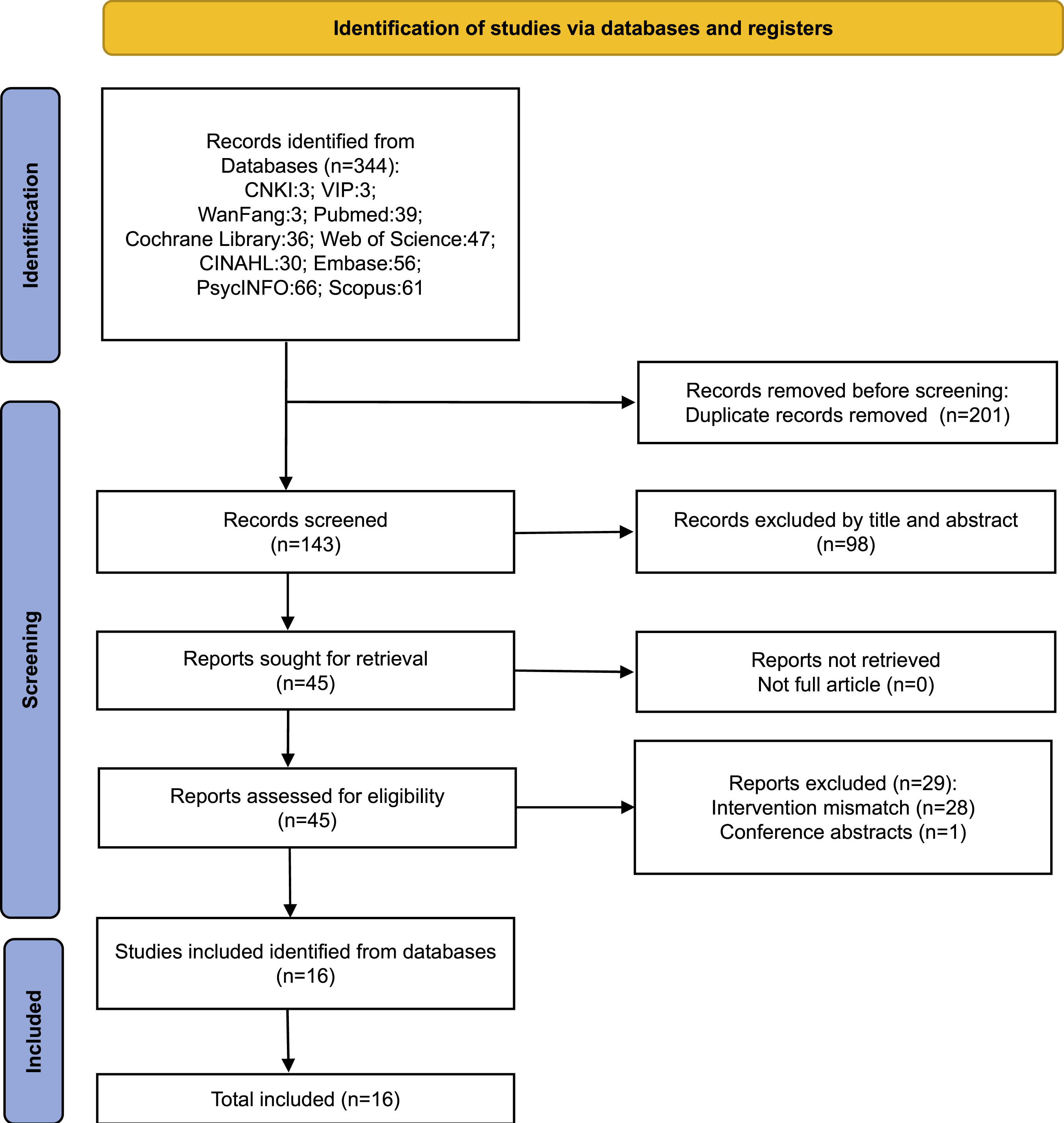
3.2. Quality Assessment of Included Studies
The Results of Methodological Quality Assessment
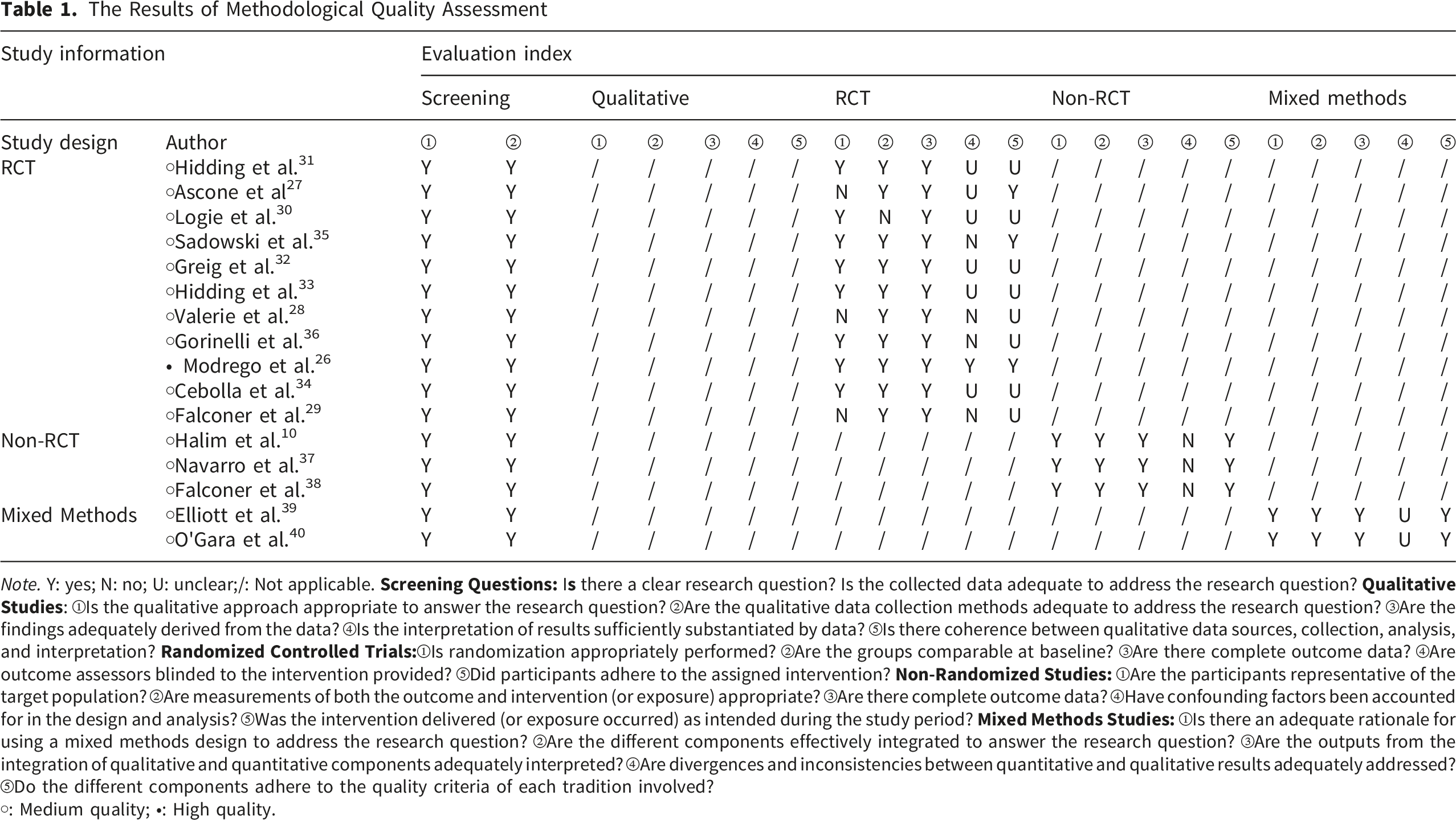
Note. Y: yes; N: no; U: unclear;/: Not applicable.
○: Medium quality; ●: High quality.
3.3. Basic Characteristics of Included Studies
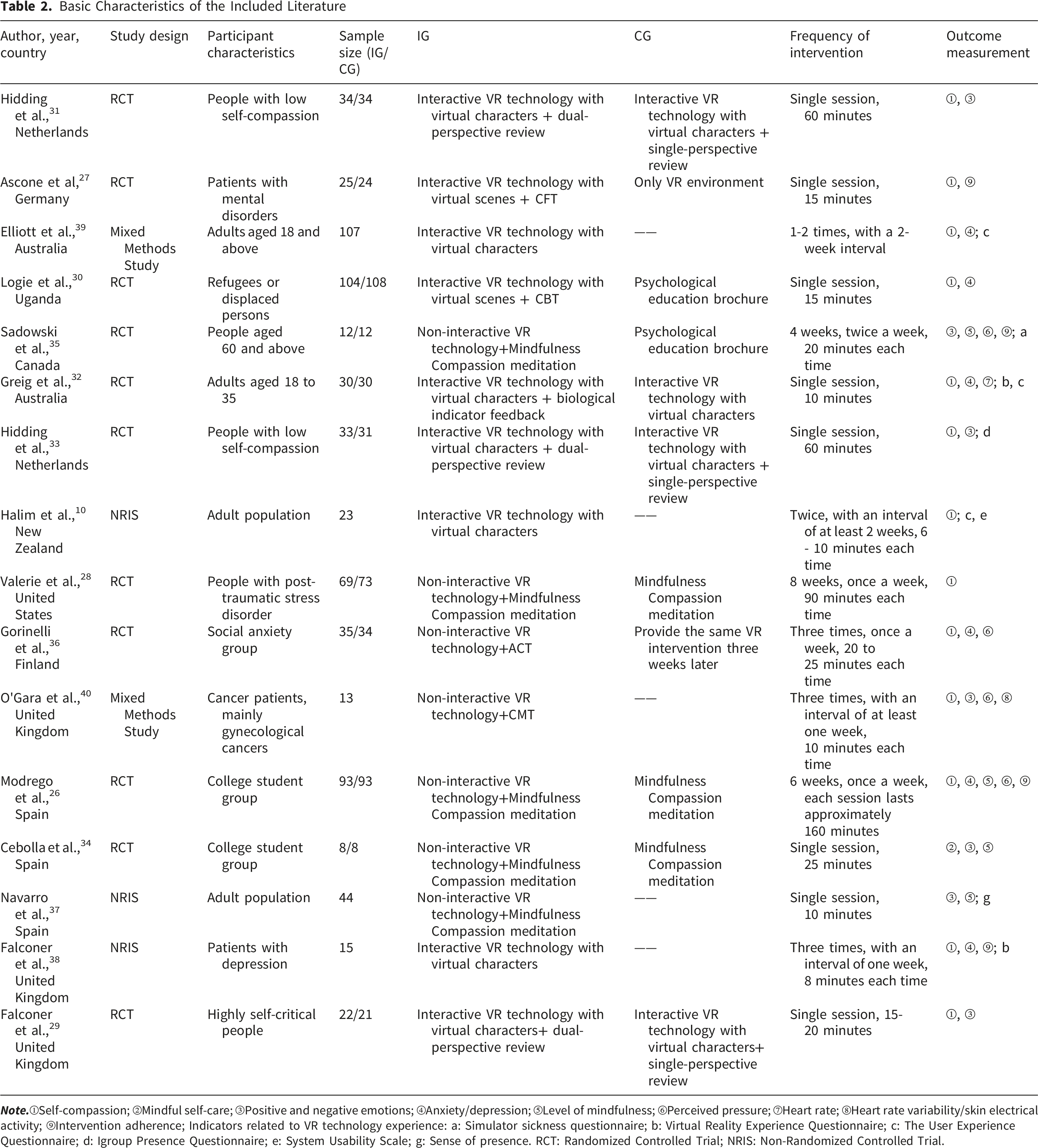
Basic Characteristics of the Included Literature
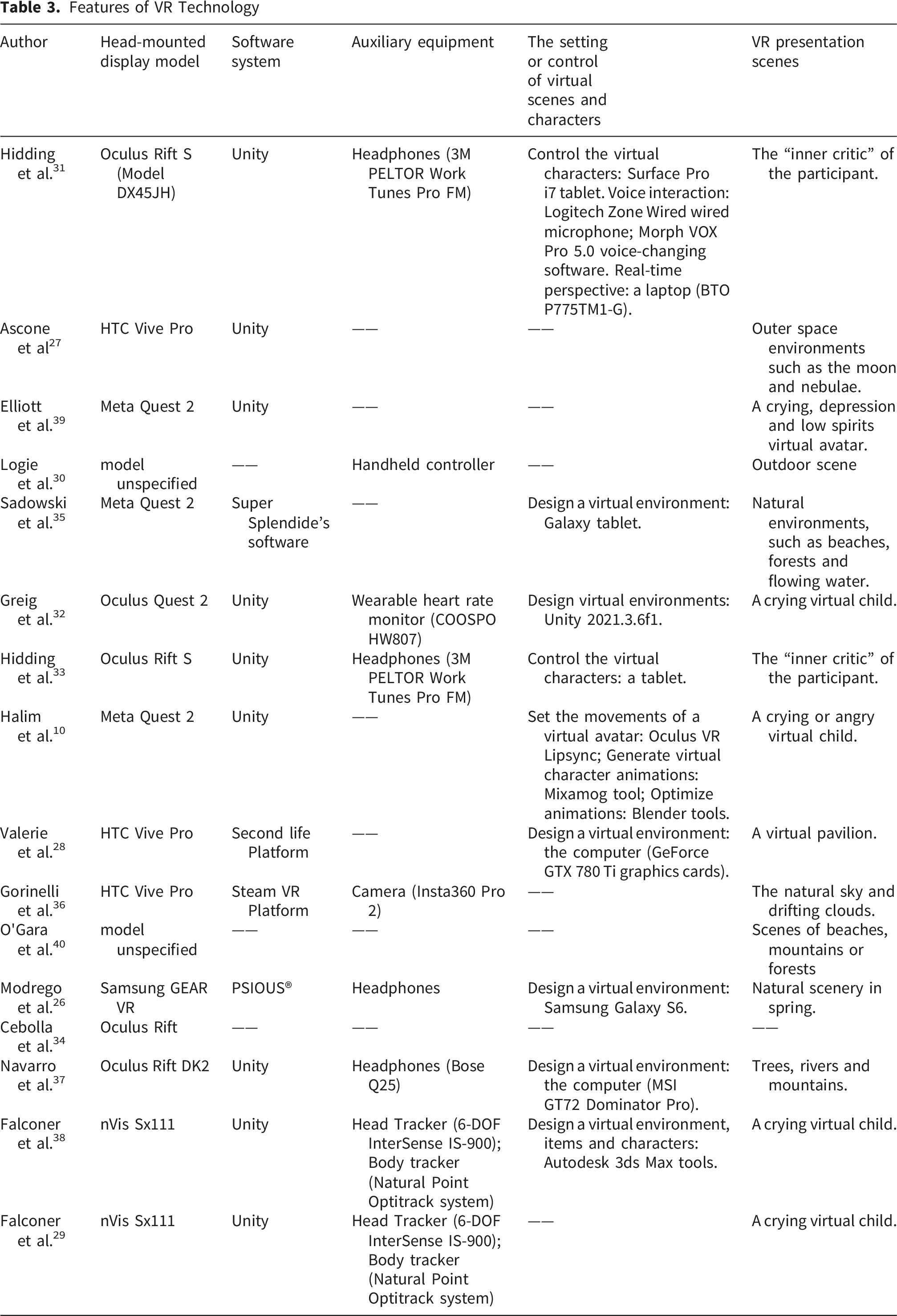
Features of VR Technology
3.4. Intervention Types and Target Populations
3.4.1. Non-Interactive VR in Self-Compassion Interventions
Non-interactive VR typically immerses participants in soothing virtual environments where they passively receive psychological therapy. Seven studies combined VR with mindful self-compassion meditation,26,28,34,35,37 Acceptance and Commitment Therapy (ACT), 36 or Compassionate Mind Training (CMT) 40 respectively. Virtual environments included pavilions, 28 beaches,35,40 trees, rivers, or forests, 37 often accompanied by individually preferred audio or 3D spatial sounds such as ocean waves, birdsong, or rainfall. 35 Interventions were delivered by psychologists or counselors in psychotherapy or community activity rooms. Target populations included older adults 35 (n=1), individuals with post-traumatic stress disorder 28 (n=1), patients with social anxiety disorder 36 (n=1), cancer patients 40 (n=1), college students and general adults26,34,37 (n=3). Regarding intervention frequency and duration, two studies34,37 delivered a single session lasting 10-60 minutes; two studies36,40 delivered three sessions with intervals of at least one week, each session lasting 10-25 minutes; three studies26,28,35 delivered interventions lasting 4-8 weeks, with a frequency of 1-2 sessions per week and session durations ranging from 20 to 160 minutes.
3.4.2. Interactive VR in Self-Compassion Interventions
3.4.2.1. Virtual Scene-Based Interactive Interventions
Only two studies used this approach, enabling simple interactions such as pointing and touching. Ascone et al 27 designed an outer-space VR scene based on compassion-focused therapy; participants used hand trackers to touch glowing orbs in a nebula, making them emit light to symbolically reinforce self-compassion. Logie et al 30 used three virtual teaching scenarios rooted in cognitive behavioral therapy, where participants navigated and touched speech bubbles for psychoeducational content using handheld controllers. Interventions were delivered by psychologists and counselors. These approaches were applied to patients with psychiatric disorders 27 (n=1) and refugee youth at high risk of emotional disorders 30 (n=1), with a single session duration of 15 minutes in both studies.
3.4.2.2. Virtual Character-Based Interactive Interventions
Seven studies involved virtual characters in two primary forms. The first embodied the participant’ s inner self-criticism,31,33 a method derived from two-chair dialogue therapy.
41
The interventionist built the virtual character based on the participant’ s self-critical statements31,33 and adjusted personalized attributes such as size, facial expression, and voice.31,33 During the intervention, participants were guided to respond to the criticism with firm, self-compassionate language. The second form presented a vulnerable, self-critical character, such as a crying child.29,38 Prior to the intervention, the interventionist taught compassion skills, including emotion identification, attention shifting, and evocation of positive memories.
10
Participants then played the role of “comforter,” practicing these skills in VR.10,29,32,38,39 Afterwards, they could review a video recording of their interaction from a third-person perspective.
31
Interventions were delivered by psychiatrists trained in professional psychotherapeutic techniques and were applied to individuals with low self-compassion31,33 (n=2), depression
38
(n=1), highly self-critical populations
29
(n=1), and general adults10,32,39 (n=3). Most studies involved two or more sessions, with session durations of 8-60 min; a few delivered a single 60-minute session. As shown in Figure 2. Self-compassion intervention types based on VR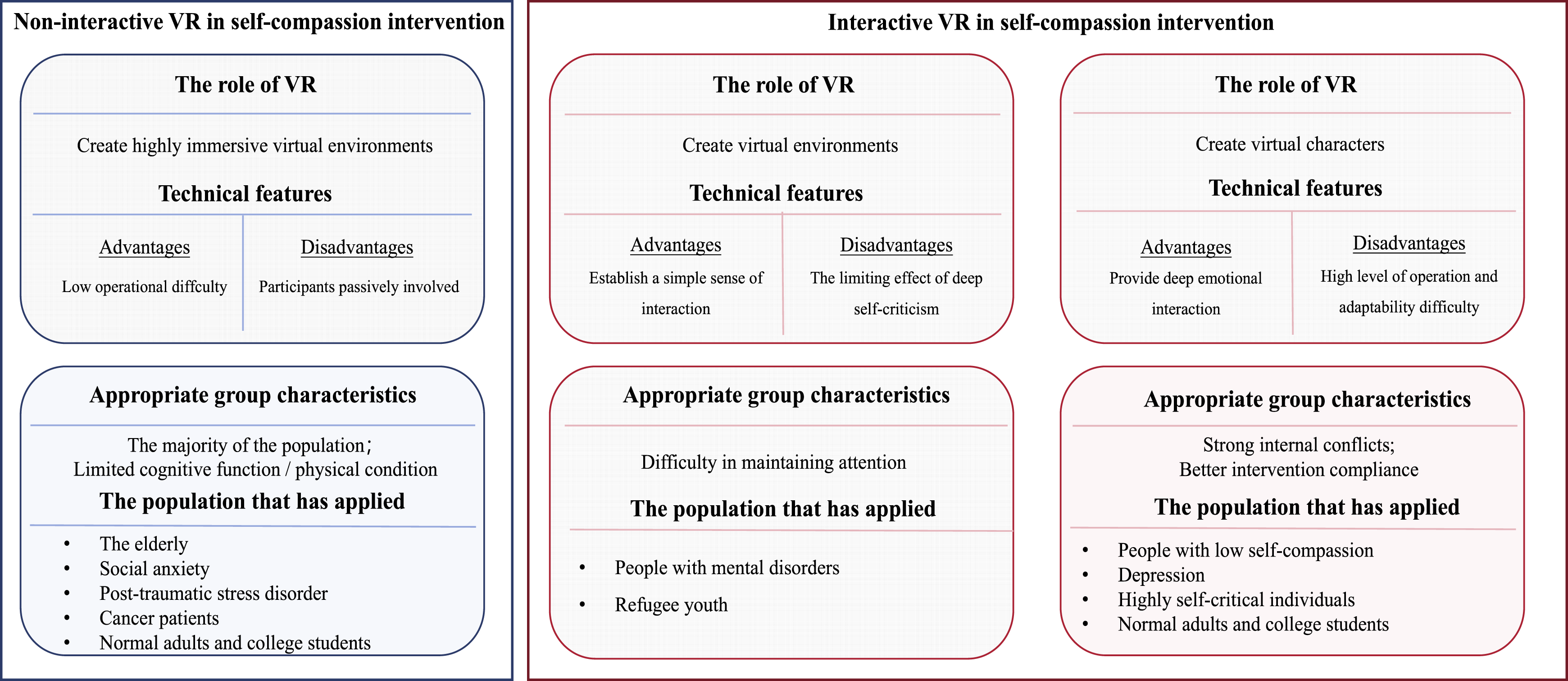
3.5. Primary Outcomes Assessment and Effectiveness of Intervention
The outcome measures of self-compassion intervention based on VR mainly cover five domains: self-compassion, emotional state, physiological indicators, intervention adherence, and user experience. Regarding self-compassion assessment, using the Self-Compassion and Self-Criticism Scale (SCCS) in five studies,29,31-33,38 8 studies10,26-28,30,36,39,40 utilized the Self-Compassion Scale (SCS), and one study 34 applied the Mindful Self-Compassion Scale (MSCS). Emotional state was measured through indicators such as positive and negative affect,29,31,33-35,37,40 anxiety and depression levels,26,30,32,36,38,39 mindfulness levels,26,34,35,37 and perceived stress.26,35,36,40 Moreover, two studies monitored physiological indicators via wearable sensors, including heart rate, 32 heart rate variability, and electrodermal activity. 40
Among non-interactive VR interventions, five reported significant improvements in self-compassion,26,28,34-36 whereas one 40 found no significant change. Three studies showed reductions in negative emotions.26,36,40 Two studies showed decreased perceived stress.35,36 One study 36 further demonstrated a decline in electrodermal activity during and after the intervention. In virtual scene-based interactive interventions, one study 30 found significant self-compassion improvement, while another 27 did not. All seven virtual character-based interactive studies reported increased self-compassion,10,29,31-33,38,39 and five additionally observed decreased self-criticism.29,31-33,38
3.6. Acceptability and Strategies to Enhance Adherence
Acceptability was reflected in adherence and user experience. Four studies26,27,35,38 evaluated adherence by calculating attendance and completion rates, reporting 95.7%, 26 92.50%, 27 85.71%, 35 and 86.7%, 38 respectively. User experience was assessed through usability,10,32,38,39 sense of presence,33,37 and adverse events. 35 In the interactive VR study, 27 77% of participants rated the experience highly enjoyable and 23% were neutral, though issues such as insufficient interactivity, system lag, and monotonous scenes were also reported. 10 Among non-interactive VR users, 91.67% enjoyed the experience and 90.9% expressed willingness to continue. 35 A small number of participants experienced mild symptoms such as nausea, 35 dizziness, 40 oculomotor discomfort, and disorientation 35 ; however, most symptoms diminished over time. Additionally, the excessive weight of the head-mounted display also caused discomfort.
Strategies were implemented in the included studies to enhance intervention compliance (see in Figure 3). Regarding reminders and incentives, two studies26,30 utilized text messages or application notifications, whereas three studies10,29,31 employed incentives such as lotteries, earning points, or monetary rewards. For social support, two studies10,30 established peer support via weekly group discussions on platforms, and four studies31,33,35,39 provided continuous professional guidance. Additionally, two studies26,29 supplied supportive materials such as audio recordings and written instructions to facilitate the intervention process or daily home practice. To optimize the intervention design, one study
10
incorporated a VR system equipped with clear tutorials and a friendly interface to mitigate usability barriers. Another study
36
involved participants in co-design of the intervention, enabling personalized customization of elements such as the gender, tone, and speed of the guidance audio. Four studies10,28,32,33 permitted participants to select personalized avatars or virtual environments according to their preferences. Two studies36,40 administered assessments immediately after the intervention and provided feedback by visualizing outcome trends, thereby helping participants recognize their progress. Adherence strategies of virtual reality in self-compassion intervention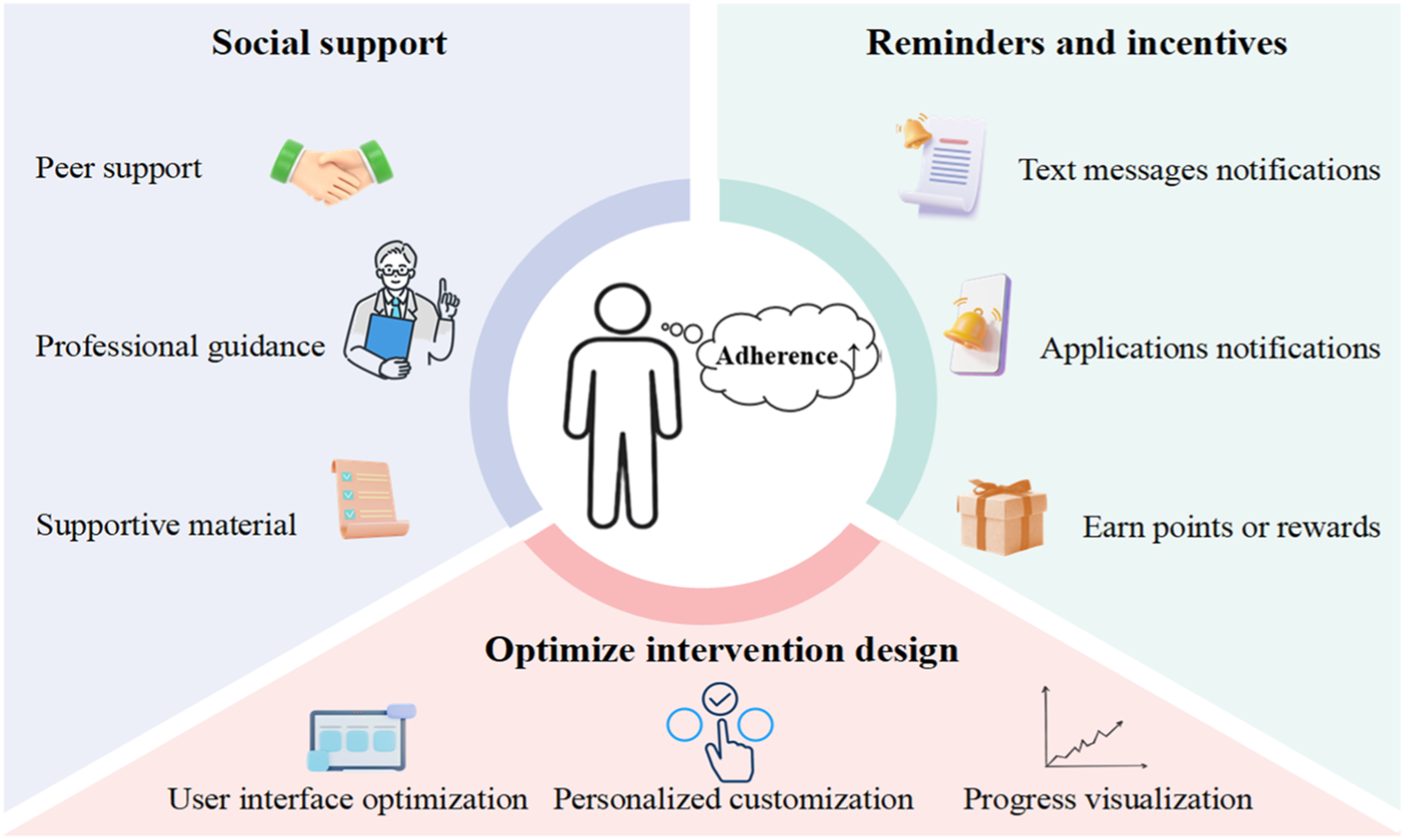
4. Discussion
4.1. Overview of the Included Literature
This scoping review comprehensively summarizes the current applications and efficacy of virtual reality technology in self-compassion interventions. A total of 16 studies encompassing 1,135 participants were incorporated. The included articles were rated as high or moderate in quality, indicating reliable findings and providing solid evidence to support the conclusions of this review.
The publication dates are predominantly clustered between 2014 and 2025, indicating that VR self-compassion intervention has been in a stage of rapid development over the past decade. The majority of the included studies were randomized controlled trials (RCTs) (11/16, 68.75%) or non-randomized controlled trials (3/16, 18.75%). The majority of the studies (10/16, 62.5%) were conducted in European nations, specifically the United Kingdom, Spain, Finland, Germany, and the Netherlands, whereas studies from other regions were comparatively scarce. All studies employed immersive VR technology, with interactive VR (9/16, 56.25%) being marginally more prevalent than non-interactive VR (7/16, 43.75%). Future research ought to verify the efficacy of virtual reality in self-compassion interventions within more extensive cultural contexts.
4.2. Intervention Types and Adaptability Across Populations
Based on interactivity, interventions were classified as non-interactive or interactive, with the latter further divided into virtual scene-based and virtual character-based interactions.
Non-interactive VR delivers highly immersive scenes, 37 in which participants receive visual and audio guidance without active manipulation. 42 Its low usage threshold 35 makes it suitable for most populations, particularly those with cognitive or physical limitations that hinder device operation. It has been applied to improve mental health in older adults 35 and cancer patients, 40 and serves as an adjunctive technology for treating social anxiety, 36 post-traumatic stress disorder, 28 college students and general adults. However, participants remain passive recipients, and effects depend heavily on how well scene design matches individual preferences; thus, assessing these preferences is advised to improve acceptance. Because intervention duration varies widely across studies,26,28,35 future research should determine the optimal duration.
In scene-based interaction, participants autonomously engage with environmental elements via handheld controllers or hand trackers. 27 This approach involves moderate complexity, basic engagement, and typically short single sessions. 30 It suits populations with attention difficulties, such as those with psychiatric or emotional disorders.27,30 Given limited interaction forms, its effect on alleviating deep self-criticism is relatively constrained. Future research should optimize interactive task design and explore integration with other psychological interventions.
In character-based interaction, emotionally expressive virtual characters are constructed to embody the participant’ s inner “self-critic”31,33 or to represent a vulnerable figure seeking comfort.29,32 Participants interact from a first-person perspective. This technique directly targets self-critical cognitive patterns and provides deep emotional engagement, making it suitable for populations with significant self-conflict, such as those with low self-compassion,31,33 depression, 38 and high self-criticism. 29 Nevertheless, this technology imposes high demands on both operational skills and user adaptability, and also requires participants to have good intervention compliance and verbal expression skills. Future studies could simplify interaction procedures, reduce adaptation difficulty, and adopt progressive models incorporating simple interactive exercises to gradually build participants’ competence.
4.3. Intervention Effectiveness
In non-interactive VR, most studies26,28,34-36 found significant improvements in self-compassion, consistent with Han et al 43 This may be because highly realistic, personalized environments 37 reduce demands on imaginative resources and cognitive load, 42 enabling deeper emotional focus. However, O’Gara et al 40 found no significant change in cancer patients, possibly due to physical burden during treatment or rehabilitation and low perceived relevance of self-compassion content. 40 Future research should test the applicability of non-interactive VR in clinical populations with larger sample sizes 36 and tailor content to patients’ physical and psychological characteristics.
The effectiveness of scene-based interaction requires further confirmation. Ascone et al. 27 found no significant effect in patients with psychiatric disorders, perhaps because a single brief intervention was insufficient. In contrast, Logie et al. 30 found that their intervention significantly improved self-compassion levels among refugee youth, possibly due to a high match between the intervention content and the needs of the target population, including identification of depressive symptoms, role-playing experiences of mental health stigma, and exercises on self-compassion and emotion regulation. Future research should systematically compare the effects of different intervention duration on self-compassion and conduct content adaptation studies for different populations.
In interaction with virtual characters, all included studies reported that this approach effectively improved participants’ self-compassion levels.10,29,31-33,38,39 This may be because VR can externalize the participant’ s inner critical voice into a visible virtual character, 31 enabling direct first-person dialogue that transcends imaginative limits and resolves internal conflicts. 33 Additionally, participants help the virtual character cope with negative emotions in the VR scenario and practice self-compassion skills, 32 gradually internalizing the compassion they express outwardly into self-compassion abilities. 39 Participants can also review the interaction process with the virtual character from a third-person perspective, which further promotes the internalization of compassion. 29
VR technology offers a novel and effective approach to self-compassion interventions. Clinicians can adapt it to specific disease characteristics and cultural contexts, delivering more immersive, targeted psychological support. Administrators may consider integrating VR-based self-compassion protocols into clinical training systems to enhance healthcare professionals’ familiarity with the technology.
4.4. Acceptability of VR in Providing Self-Compassion Interventions
Both non-interactive and interactive VR demonstrated good acceptability, as evidenced by high adherence rates and favorable user experiences. In terms of adherence, four studies26,27,35,38 reported that the adherence rates to VR interventions ranged from 85.71% to 95.70%. This high adherence can be ascribed to the inherent novelty of VR technology, which can enhance participants’ interest and intrinsic motivation. 44 Moreover, the integration of strategies such as motivational feedback, peer support, or personalized environment design in some interventions probably contributed to the improvement of engagement. Regarding user experience, participants generally reported that the VR system interfaces were user-friendly with intuitive guidance,10,37,38 effectively lowering the usability threshold. The majority of participants reported a strong sense of presence and immersion in the virtual environments and appreciated the personalized avatar and scene designs. The utilization of interactive VR technology in several studies,27,29,31,38 which enables interaction through controllers or hand gestures, was found to enhance the engaging nature of the intervention. Nevertheless, some challenges were reported, including limited interaction modalities with virtual avatars, intermittent system latency or lag, a dearth of scene variety, 10 blurred visuals, and the heaviness of the head-mounted displays. 35 Additionally, the study 40 reported that some participants experienced mild physiological reactions such as dizziness and nausea.
Future research should pay greater attention to adherence metrics, optimize the usability design of VR hardware, continuously improve technical performance, and closely monitor users’ adverse effects. These endeavors are crucial for further enhancing the feasibility and safety in clinical practice.
4.4. Problems of Current Literature and Future Directions
The present application of this method has manifested promising outcomes. However, certain issues persist regarding intervention strategies, duration, and measurement indicators. Firstly, the majority of the included studies involve short term interventions, rendering it arduous to evaluate the persistence and stability of the intervention effects. 31 The determination of intervention duration lacks relevant empirical evidence. 45 On the premise of considering economic effects, long-term randomized controlled trials could be attempted, and follow-up mechanisms could be established 33 to further examine the application effects and systematically compare the influence of different intervention durations and frequencies on the outcomes. Secondly, outcome measures predominantly rely on subjective self-reports, which are subject to certain recall biases. Future investigations can measure objective physiological indicators such as heart rate, heart rate variability, skin electrical activity, or electroencephalogram. 23 Finally, although some studies have proposed adherence strategies, few have systematically evaluated their actual effects. Future research can selectively incorporate adherence strategies into intervention programs and evaluate their impact on intervention adherence and effects.
4.5. Limitation
Firstly, the absence of grey literature may introduce publication bias. Secondly, the geographic distribution of the included studies is highly concentrated in Europe. Cross-cultural differences in the understanding of self-compassion and acceptance of VR technology thus limit the generalizability of the findings. Thirdly, restricting the search to Chinese and English sources may have led to language bias. Finally, most of the included studies have methodological limitations, and the overall quality of evidence is moderate. Therefore, the conclusions need to be further validated by high-quality, large-sample studies.
5. Conclusion
This review synthesized VR-based self-compassion interventions and classified them into two main types: non-interactive and interactive. Each type has distinct technical features and target populations. Overall, these interventions effectively enhance self-compassion, and participants generally showed high acceptance. Several studies also implemented strategies to improve adherence. However, intervention duration varies markedly, and practical applications face limitations. Future research should explore intervention effects across diverse populations and establish optimal duration, thereby providing more targeted empirical evidence for improving mental health in various groups.
Supplemental Material
Supplemental Material - Virtual Reality Technology in Individual Self-Compassion Interventions: A Scoping Review
Supplemental Material for Virtual Reality Technology in Individual Self-Compassion Interventions: A Scoping Review by Musen Hua, Jinping Bai, Zanteng Li, Shuya Chen, Jiacheng Su, Fuyan Zhang, Bowen Zheng and Li Yang in INQUIRY: The Journal of Health Care Organization, Provision, and Financing.
Supplemental Material
Supplemental Material - Virtual Reality Technology in Individual Self-Compassion Interventions: A Scoping Review
Supplemental Material for Virtual Reality Technology in Individual Self-Compassion Interventions: A Scoping Review by Musen Hua, Jinping Bai, Zanteng Li, Shuya Chen, Jiacheng Su, Fuyan Zhang, Bowen Zheng and Li Yang in INQUIRY: The Journal of Health Care Organization, Provision, and Financing.
Footnotes
Ethical Considerations
Our study did not require an ethical board approval because this manuscript is a scoping review.
Author Contributions
HMS and BJP was responsible for the study design, developing the literature search strategy, literature search, data extraction and writing the first draft. LZT, CSY, SJC, ZFY and ZBW was responsible for the literature search, data extraction and writing part of the first draft. YL was responsible for providing their expertise, making suggestions and critically revising the first draft. Musen Hua and Jinping Bai made equal contributions to this manuscript.
Funding
The research in this paper was supported by the University-Level Educational Teaching Reform Research Project of Shandong First Medical University & Shandong Academy of Medical Sciences (Grant No.:XM2024032).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
No datasets were generated or analysed during the current study. All relevant data are within the paper and its Supporting Information files.
Declaration of Generative AI and AI-assisted technologies in the writing process
No AI tools/services were used during the preparation of this work.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.