
Abstract
Introduction
Although Young people with disabilities (YPWDs) have similar sexual and reproductive health and rights (SRHR) and sexual desires as their non-disabled peers, equitable access to these essential services remains largely overlooked for this population segment. This exclusion exacerbates compounded vulnerabilities. To address the specific challenges faced by YPWDs, integrated and tailored SRH information and services are essential. This study aims to explore the lived experience of YPWDs in accessing SRH services in Ethiopia.
Methods
A qualitative study was conducted in Areka and Tebela towns of the Wolaita zone using the Interpretative Phenomenological Analysis (IPA) approach. Nine participants aged 10 to 24 years with physical and visual disabilities were purposively recruited for In-depth Interviews (IDIs). Data were collected using a semi-structured IDI guide and a field notebook. All IDIs were audio-recorded, averaging 30.5 minutes. The six-step structured iterative IPA framework was employed. Open code software version 4.01 was used for coding and data management. Before the commencement of data collection, the principal investigator underwent a reflexive interview and shared his philosophical point of view and aims of the study with participants. The rigor of the study is ensured by maintaining the five principles of trustworthiness.
Results
The IPA yielded four overarching themes: The dualistic SRH access paradox, Intersectional burden of disability and adolescence, The critical role of youth and disability networks, and Demands for tangible improvement in SRH inclusion. Most YPWDs who participated in this study reported that they were facing multiple barriers when seeking to access SRH services.
Conclusion
This study navigates the profound marginalization of YPWDs in accessing SRH services in Ethiopia. The healthcare system must dismantle dehumanizing societal attitudes, establish and strengthen community networks, and ensure enforcement of disability and SRH standards.
Introduction
Globally, People with disabilities (PWDs) constitute about 16% of the population, with the majority living in low and middle-income countries. 1 Of an estimated 180 million Young People with Disabilities(YPWDs) aged 10-24 years worldwide, nearly 144 million (80%) live in low-income countries, where healthcare, education, and employment are not fully attained. 2
Young people, defined as individuals aged 10-24 years, experience a critical period of human development characterized by profound physical, emotional, and psychological transformations. At this stage, they begin to navigate emerging sexuality, form identities, and establish behavioral patterns that often persist into adulthood. 3 Access to comprehensive Sexual and reproductive health (SRH) services during this stage of life is essential to ensure healthy development and early prevention of adverse outcomes, including unintended pregnancy, unsafe abortion, HIV, and other sexually transmitted diseases (STIs). 4 However, Young People with Disabilities(YPWDs) often face barriers in accessing these essential services. 5
In Africa, the situation demands urgent attention due to the rapidly growing young population. Approximately 315 million young people live in Africa, representing about 31.8% of the continent’s total population. 6 Similarly, about 33% of the Ethiopian population is found in the young age group. 7 Evidence in Ethiopia indicates that a significant portion of the population lives with disability, with the national prevalence estimated at 17.6%. 8 Despite these numbers and the recognized benefit of SRH services, substantial gaps remain in the literature, particularly regarding YPWDs’ unique SRH needs, accessibility barriers, and coping strategies, which are under-explored in Ethiopia.
All people have the right to access equitable SRH services that ensure their overall reproductive health and wellbeing. 9 Although YPWDs have similar SRH rights and sexual desires to those without disabilities, equitable access to these essential services remains overlooked for this population segment. This exclusion exacerbates the compounded vulnerability arising from being both an adolescent and disabled, putting them at a heightened risk of vulnerability. They are likely to experience marginalization if also disadvantaged by their gender, age group, ethnicity, race, or even economic standing, thereby posing additional obstacles to utilizing SRH services. 10
Despite enforcement variations, many countries, including Ethiopia, have recognized the sexual and reproductive health and rights (SRHR) of young disabled people.4,11 However, limited implementation of these global commitments may widen existing inequalities in access to SRH services and hinder progress towards achieving the third Sustainable Development Goal (SDG 3) of the 2030 United Nations (UN) Sustainable Development Agenda. 11 There has been a significant number of YPWDs in many parts of the globe, including Ethiopia, suffering from poor SRH outcomes, including STIs, unintended pregnancy, and unsafe abortion, mainly due to the unmet need for SRH services.4,12,13 This indicates that the world is still far from realizing the highest attainable SRH standards for YPWDs. 12
Evidence from Ethiopia shows that YPWDs have limited access to SRH information and services, with notable variations in utilization across geographical settings; with reported rates of 8.4% in Jimma, 14 29.4% in Bahirdar, 15 and 42% in Dessie. 13 A recent systematic review and meta-analysis study reported a pooled estimate of 36.6% SRH service utilization in the country, reinforcing the overall limited access. 16 Additionally, a study in Arbaminch shows a significant disparity in SRH service utilization between YPWDs (40.52%) and their non-disabled peers (69.1%). 17 Qualitative study findings on this topic in Ethiopia further reveal the existence of multi-level barriers to accessing and utilizing SRH services. 18 The interplay of structural, socio-cultural, diseases, and health system-related factors drives the low uptake and inequitable SRH services for YPWDs in Ethiopia.19-21
The variation in SRH service uptake across different geographic settings reflects context-specific inequalities, highlighting the need for in-depth, contextually grounded qualitative studies to inform inclusive and responsive interventions in Ethiopia. Most studies conducted in Ethiopia regarding the accessibility and utilization of SRH services by YPWDs are measurement-driven and often explored from a deficit perspective; there remains a gap in the literature from the contextualized lived experiences of YPWDs. Bridging the existing information and knowledge gap will help better understand the challenges and provide a policy foundation for inclusive actions. Grounded in intersectionality, a theoretical framework coined by Kimberlé Crenshaw (1989), which examines how various social identities such as gender, age, economic class, and disability status intersect and create compounded marginalization and subjective inequalities, 22 this study employed an interpretative phenomenological analysis to explore the lived experiences of YPWDs in accessing SRH services in Ethiopia.
Methods
Study Design
A qualitative study was conducted using the Interpretative Phenomenological Analysis (IPA) framework to explore the lived experiences of young people with disabilities in accessing SRH services in Ethiopia. IPA is an idiographic methodology concerned with examining how individuals make sense of their real-life experiences. 23 The study is grounded in phenomenology and hermeneutics, informed by the interpretative philosophical perspectives of Heidegger and Gadamer, which emphasize understanding meaning through interpretation of lived experiences.23,24 It follows a double hermeneutic approach, whereby study participants interpret their lived experience, and researchers cogitatively interpret these meanings. 23 Through an iterative process, double hermeneutics enables us to explore not just what YPWDs said, but how they made sense of their SRH service-seeking experiences. The researchers were able to engage in an additional layer of interpretation to co-construct meaning from participants’ accounts. This approach is particularly suited to examine complex and under-explored experiences at the intersection of disability and adolescence (double-marginalized identities), situating intersectionality theory as the study’s core theoretical foundation. 22
Rather than complete bracketing, the study emphasizes reflexivity, acknowledging the researcher’s interpretive role and preconceptions in the research process. This approach recognizes understanding the meaning of participants’ inextricable world and acknowledges the researcher’s assumptions that could influence the research process. 25 The Consolidated criteria for Reporting Qualitative research (COREQ) Checklist was used to maintain the quality of the study. 26
Reflexivity (Reflexive Appraisal)
Before the commencement of the actual data collection, the principal Investigator (MT) participated in a reflexive interview conducted by his primary PhD supervisor, the last author (AA), to identify and clarify any presuppositions held by the researcher. The interview explored that the principal Investigator (PI) is a non-disabled public health specialist currently working on sexual and reproductive health research and programs in the country. However, due to the existing disability-inclusiveness gaps of the healthcare system, the PI held the assumption that SRH needs for YPWDs are not usually attainable. The presupposition was documented and referred back to throughout the study. Explication of such potential biases and pre-understanding of the PI on the phenomenon of interest fostered an authentic and open awareness that was continuously referred back to and reflected upon during data collection and analysis. To address potential bias arising from the PI’s positionality as a non-disabled researcher, the PI shared his philosophical viewpoint and aims of the study with participants before each interview. Additionally, the interviews were conducted in locations chosen by participants, and they were also allowed to bring their trusted family members or personal assistants if they desired.
In this study, reflexive memos were written at the initial reflexive interview, after each participant interview, and during coding. These memos were referred back to throughout the study to enable the PI to remain alert to the risk of imposing his presuppositions before hearing participants’ experiences. For example, the PI initially assumed that the unmet need for SRH services would be the dominant theme in the study. However, interviews revealed that participants frequently cited the need for SRH autonomy and compounded vulnerability arising from the intersection of adolescence and disability. This insight prompted the PI to revisit and reorganize the coding framework. Consequently, “Intersectional burden of disability and adolescence” emerged as a superordinate theme, while “ Unmet SRH needs” was retained as a supporting subtheme.
Participants Recruitment Procedure
Study participants were purposefully recruited from Areka and Tebela towns, which were identified as areas identified as having the highest number of PWDs in the Wolaoita Zone in the 2024 reporting period. 27 Kebeles (the smallest administrative unit in Ethiopia) were identified in consultation with respective district offices. Participants were targeted with the help of community Health Extension Workers (HEWs) working at the respective kebeles of the two towns. Community HEWs identified and contacted eligible participants through the existing community networks and home-to-home visits. Both urban and semi-urban kebeles were considered in the assumption that clients from a varied community setting will have varied experiences, perceptions, and perspectives related to SRH service utilization.
Nine individuals aged 10-24 years with visual and physical disabilities within the selected kebeles were purposefully selected for the study. Individuals with hearing, mental, and cognitive (learning disorder) disabilities were excluded from the study due to communication access challenges, as the research team lacked certified sign language interpreters fluent in SRH terminologies capable of undergoing deep exploration of their lived experiences. All targeted participants consented to undergo the interview. The sample size needed for this study takes into consideration previous literature experiences, 28 and the flow and power of ideas in the in-depth interview session (data saturation). 29 Data saturation was assessed by using the concept of information power rather than thematic repetition alone, with data collection continuing until new interviews from participants contributed minimal or no additional analytical insights.
Data Collection
Data were collected through in-depth interviews. A semi-structured interview guide was used to ensure a smooth, logical flow of the in-depth interview. The IDIs focused on exploring YPWD’s knowledge of SRH, experiences, barriers and enablers, unique needs, and improvement strategies regarding SRH services. Before the actual interview, the audio recording device’s functionality and the IDI guide (supplementary file) were checked with two individuals outside the study area to test the question sequence and ensure the information was easily accessible.
The in-depth interviews took place in a private and comfortable area (at their house or nearby health post) based on their preferences, allowing participants to freely express their opinions. Data were collected by the PI and a research assistant with previous experience in qualitative data collection, both of whom are proficient in local languages. The lead interviewer, a male public health specialist, had completed basic sign language training and an online disability-inclusive interviewing course.
The central questions for respondents were “What are your sexual and reproductive health experiences? What enablers and barriers governed your SRH service access? What areas do you think need to be manipulated to improve the accessibility and inclusiveness of SRH services for YPWDs? From there, probing questions were asked to explore and understand participants’ experience of SRH service utilization. Appropriate probing questions like (Would you explain more? Can you tell me an example? Would you elaborate on it more? I’m not sure I understand what you say?) and so on…) were applied as needed.
All interviews were audio-taped and lasted an average of 30.5 minutes; data collection ceased when data saturation was reached. The PI documented every relevant piece of information and modified the IDI session when needed. The PI also took notes on nonverbal cues, emotional signs, facial expressions, and participants’ tone during the interview sessions. Regular discussions with the research crew were conducted to enhance the credibility and reliability of the study findings. Data were kept in a secure file manager at all steps in the research process, and participant autonomy was maintained at all steps.
Data Analysis
Data analysis followed the structured iterative IPA framework outlined by Smith, Flowers, and Larkin 23 and the quality indicators specified by Nizza et al. 30 The audio-recorded interviews conducted in Amharic (local language) were transcribed verbatim by the research team. Transcripts were then translated into English and integrated with field notes. To preserve linguistic and semantic nuances, back-translation was performed by two independent bilingual coders who cross-checked each other’s work.
As recommended by Nizza, Farr, and Smith, 30 each in-depth interview record and field note was analyzed and interpreted independently by the two authors. Each interview was analyzed individually, enabling the construction of meaning by the participant and researcher.
The analysis began with repeated reading of the transcripts to achieve immersion into the data, followed by a detailed line-by-line (in vivo) examination of each transcription to inductively generate initial codes capturing descriptive, linguistic, and conceptual notes. This step enables the identification of salient elements (key concepts) relevant to the research question from participants’ meanings and the researcher’s psychological mechanisms. The most noticeable study participants and dyadic statements were also highlighted. The initial notes were synthesized into concise, phrase-level themes that captured the participant’s original words and the researcher’s interpretive insights. This reduction to emergent themes enables mapping of similar patterns and connectivity, and maintains the complexity of the data. The analysis proceeded ideographically, with each interview examined individually.
Following the individual analyses, the two researchers jointly shared and discussed their analyses to prevent bias and ensure reflexivity in the study. 23 All codes were reviewed by the two authors, and the dominant codes formed clusters of themes. A distinctive construct of themes was developed inductively from a cluster of themes that reflect more similar experiences (similar patterns across cases) and from any highlighted idiosyncratic differences. 31 The iterative process of writing and reworking the codes and emergent themes was continued until a coherent interpretation emerged. 32 Open code software version 4.0.3 for Windows 64 was used for data coding and management.
Finally, to make things vivid for readers, findings are vigorously reported through the direct quotations of participants, and a few identifiers alongside their socio-demographic characteristics were presented using descriptive statistics. Figure 1 illustrates the overall demonstration of IPA in the study. Flowchart of Interpretative Phenomenological Analysis in the study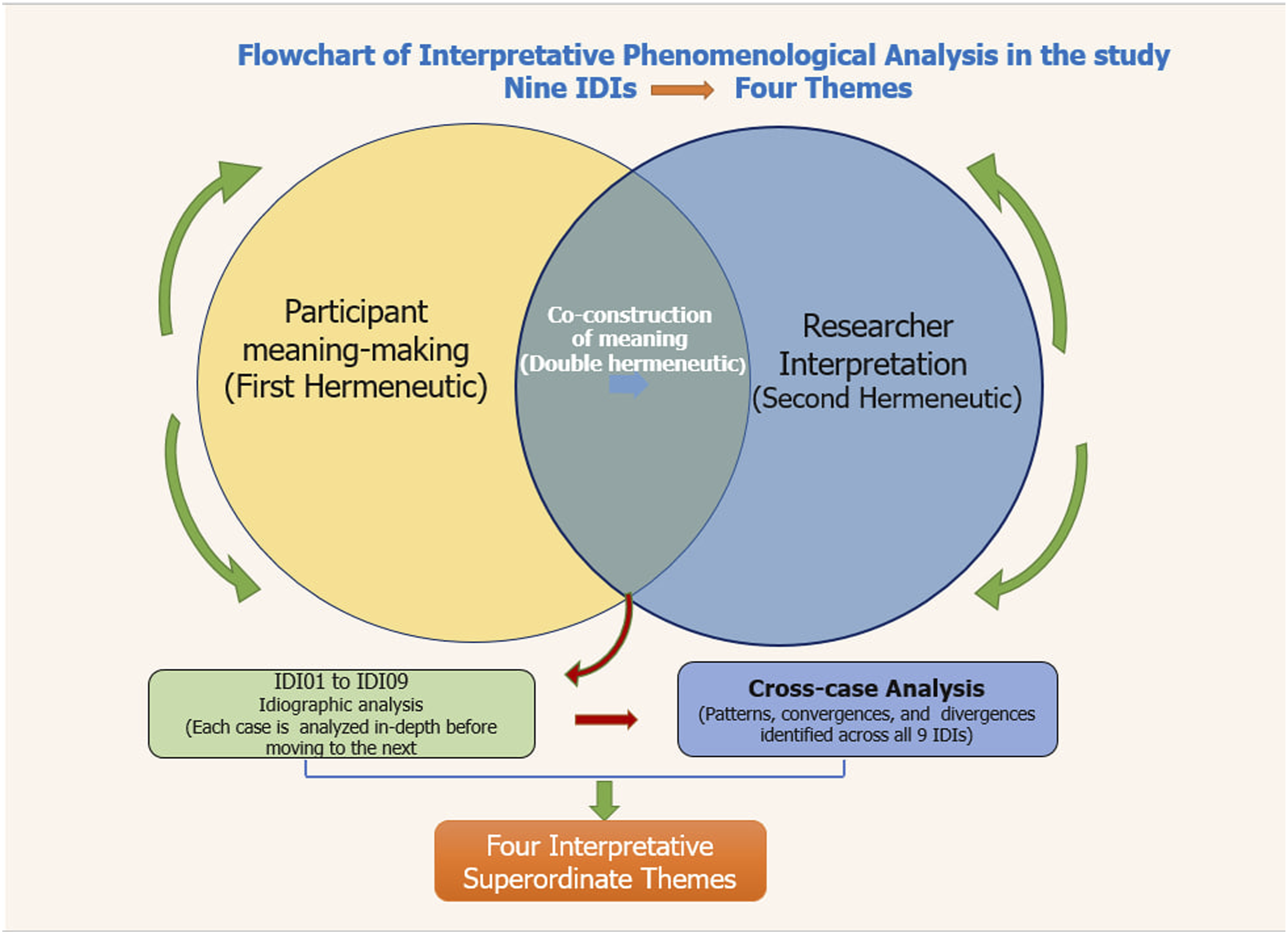
Trustworthiness
Trustworthiness refers to the application of predictable characteristics in a research process that can be trusted and consistently expressed on different occasions. 29 To maintain the rigor of the study, the five criteria of trustworthiness (credibility, transferability, dependability, conformability, and authenticity) were maintained.
Prolonged Stay in the field area helps us develop rapport and recruit the right participants to acquire deep insight into the phenomena of interest. In order to minimize bias, we used different team members with different experiences in qualitative studies for data triangulation. A copy of the transcribed text and distribution of preliminary findings to study participants were conducted to check for any inconsistencies, if present, and to supply them with additional information. All the participants responded that all themes and ideas listed in the preliminary findings were congruent with their lived experiences. To allow judgments about transferability made by readers, a thick and sufficient description of data and reports is provided. Purposive selection of the study area and participants ensured the transferability of findings. A clear method and ways of participant recruitment were employed to ensure the utilization of the findings in other comparable settings. In order to replicate the findings of the study in similar study contexts, the study included sections devoted to the research design, study area, participant selection, data collection procedures, and the researchers’ reflective appraisal statement.
This study ensured that to what extent our findings are not affected by personal interests and biases, and the degree to which the results reflect the depth of the enquiry, not the personal biases. An adequate audit trail was left for any third party to trace the sources of the research findings for confirmation upon reasonable request. In the process of conducting this phenomenological research, the principles of authenticity (the standards used to ensure the integrity, credibility, and reliability of qualitative studies 33 ) have been maintained by emphasizing genuine representation of the participants’ experiences, contexts, and perspectives as it is.
Ethical Considerations
All procedures followed the Declaration of Helsinki for human subjects. Ethical approval was obtained from the institutional review board (IRB) of Wolaita Sodo University (Ref.no. WSU 41/52/875) on 23/02/2026. Before data collection, the nature of the study, the objective, the relevance, and the level of their participation were explained to participants. Participants were asked about their willingness to be included in the study. All participants aged 18 years or older signed an informed written consent (figure printed), and those under the age of 18 years were consented to verbally, and their guardians signed the assent form. They were assured that they could withdraw from the study at any point. Confidentiality was assured by using personal ID and excluding the names of the respondents from any responses and study reports.
Results
Characteristics of Participants
Socio-Demographic Characteristics of Study Participants (Source: Field Work, February 2025)
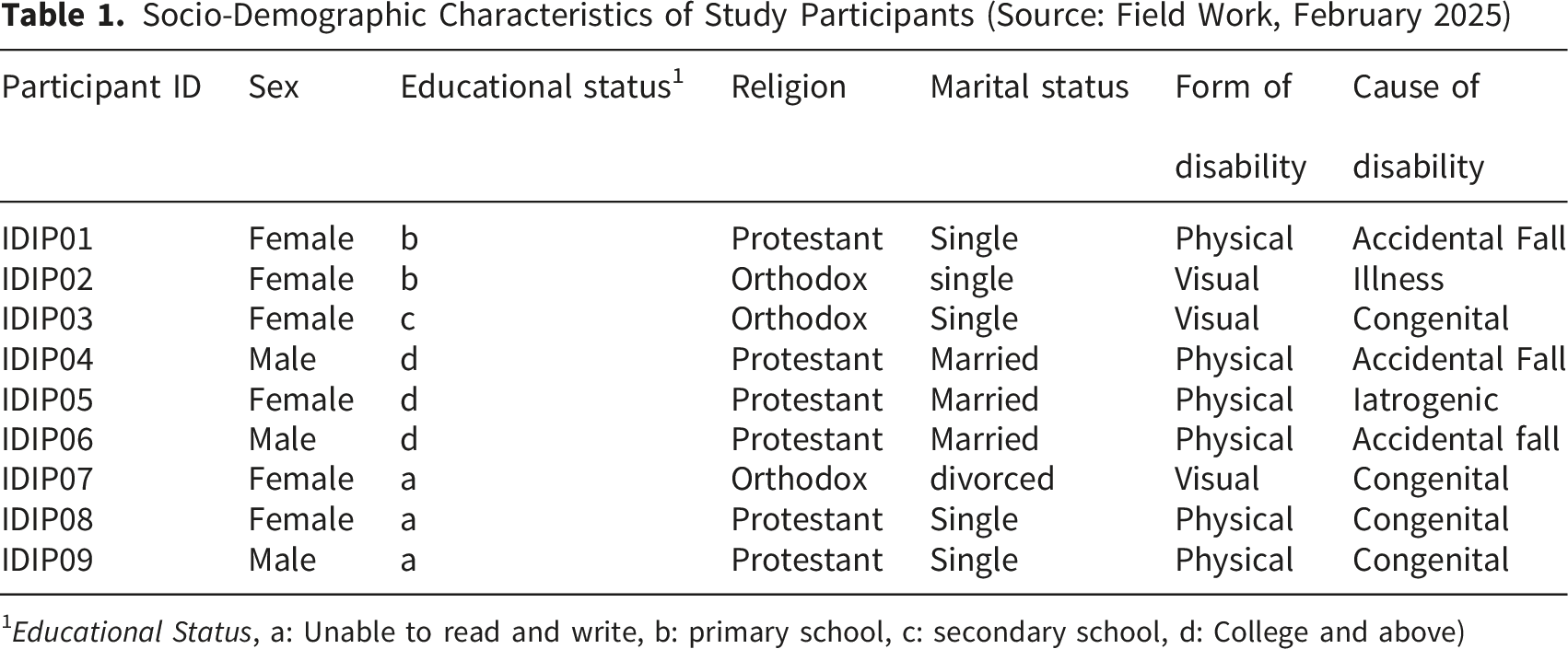
1Educational Status, a: Unable to read and write, b: primary school, c: secondary school, d: College and above)
Themes Emerged in the Study
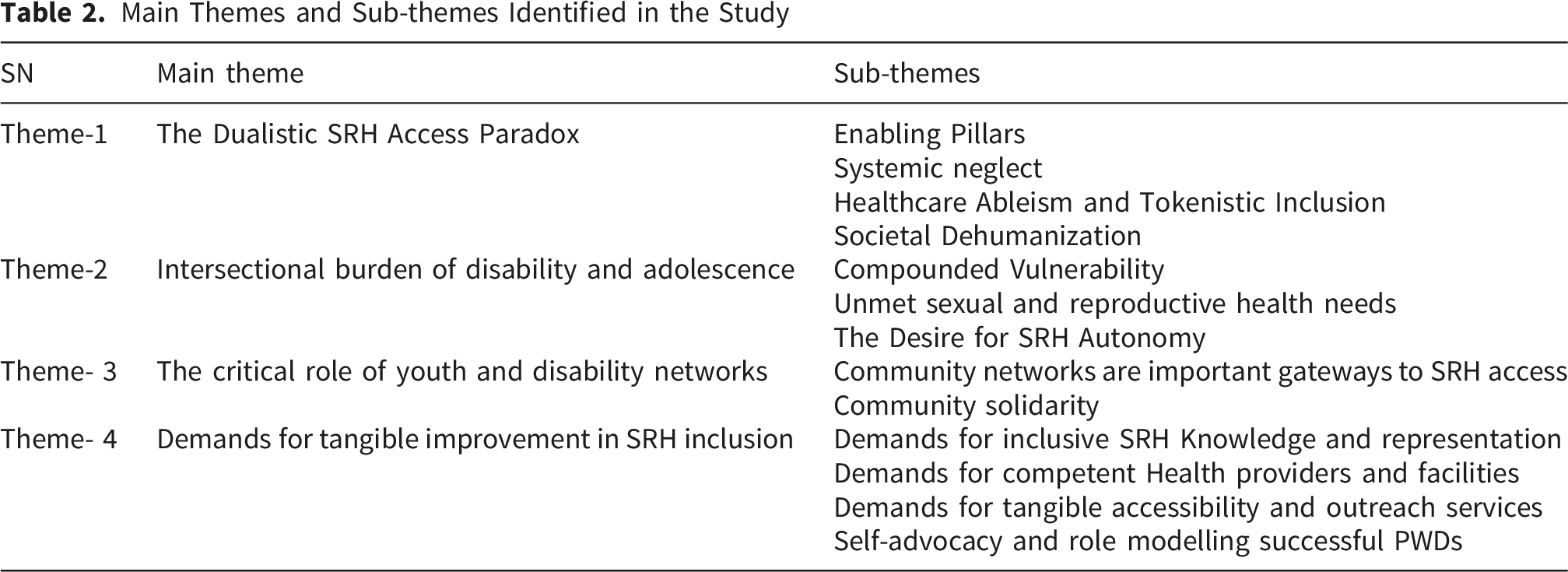
Main Themes and Sub-themes Identified in the Study
Theme 1- the Dualistic SRH Access Paradox
This theme explored the exiting paradox in the SRH service ecosystem for YPWDs. Participants recognize both the enabling pillars and the pervasive disabling systemic failure within the study area. Four sub-themes were emerged under this major theme.
Subtheme-1: Enabling Pillars
Study participants acknowledged the presence of enabling policy frameworks on equitable SRH service delivery to people with disabilities. Availability of service provision rooms, Maternity Waiting Homes (MWHs), the presence of peer educators, and the attempts made to make cost-free contraception services were among the reported enabling factors for YPWDs to access SRH services. Maternity waiting homes are locally constructed residential areas within or near to a healthcare facility arranged for pregnant women reached term to tackle geographical challenges to facility delivery. One of the Participants had to say: “Uh … during my last visit, the good thing I noticed in the facility is the cost-free access for family planning and maternity waiting homes whenever needed.” -IDIP 05, Female
Another participant added more on enabling factors: “…the presence of peer-to-peer educators assigned by the health center enables us to obtain information about condom, rape prevention, and family planning services.”- IDIP 07, female
Subtheme-2: Systemic Neglect
Young people with disabilities consistently discussed the presence of systemic barriers at different levels, beginning from the denial of tailored SRH information and advocacy support in the system to physically inaccessible health facilities. Though the presence of integrated outreach activities for other health programs and population segments, the SRH issue of YPWDs is reported as overlooked, especially in hard-to-reach areas. The shortage of necessary commodities and supplies within the healthcare facility also poses an additional burden to accessing the service.
One of the participants said that: “The difficult road to the facility is the primary reason for me for not using the sexual and reproductive health services. In times when I get a vehicle and reach to the facility, the difficult stairs within the facility again became another headache.” - IDIP 08, female
Another IDIP adds. “After moving all that long distance to the facility, facing the dangerous stairs in front of service delivery rooms makes me hopeless.” - IDIP 8, female.
Subtheme-3: Healthcare Ableism and Tokenistic Inclusion
Tokenistic inclusion refers to the various superficial efforts that appear inclusive without addressing the real barriers, 34 while healthcare ableism is a systemic discrimination against disabled people within health services, including a lack of accessible infrastructure, service prioritization mechanisms, and sign-language support. 35 Young people with disabilities described that they are not meaningfully included in healthcare as services fail to adapt to their unique SRH needs despite policy inclusion. They face long waiting hours, difficulty of accessing service delivery rooms, and lack of effective communication, makes YPWDs contribute to frustration and reduced SRH service uptake.
Accordingly, participant 6 stated, “…healthcare facilities in our area lack mechanisms in place to prioritize service provision for us, nor are there extra working hours like on weekends to address our needs.” - IDIP 06, Male
Participants also reported that healthcare systems are frequently neglecting PWDs, thereby marginalizing them in creating access for equitable, dignified SRH services. They have noted that they were facing various discriminatory attitudes, practices, and judgmental approaches within the healthcare setup.
One of the IDIP participants said, “… I heard some of the healthcare providers laughing at me while I was asking them for emergency pills for my girlfriend.” - IDIP 04, Male
Limited access to disability-inclusive SRH information and education services was also reported by study participants, contributing to not using SRH services among YPWDs. They revealed that people with hearing problems have no options to obtain the messages from HCPs. “While I was participating in a mass health education program organized for disabled individuals of different forms, I noticed that the deaf were symbolically kept in the room so that they couldn’t hear anything about what the educator was saying.” - IDIP 04, Male
Subtheme-4: Societal De-humanization
Most of the study participants disclosed that they are facing societal dehumanization in many subtle ways. Societal de-humanization is the act of considering disabled people as less worthy than fully human, often evidenced when providers or others ignore the disabled person and address their relatives/companions. 36 Many of them explained the manifestations of societal de-humanization in terms of social exclusion (being left out of school, no access to SRH information at public places, being voiceless in their matters), stigmatization, and stereotyping (assuming them as asexual, foul-minded, dependent, living with charity). Some participants disclosed the fact that such societal acts cause YPWDs to gradually develop a reminiscence effect, which they feel as if something is lost.
An IDI Participant stated it as; “I encounter many people who believe that physically disabled individuals are foul-minded, who are incapable of doing comparable tasks as they do.”- IDIP 04, Male
Another participant added, “…. Honestly speaking, beyond respecting our SRH needs, what matters most for us is being accepted as human beings in the community.” – IDIP 09, Male
Theme-2: The Intersectional Burden of Disability and Adolescence
This theme dives into how multiple intersecting identities of study participants shape their SRH service utilization experiences.
Subtheme-1: Compounded Vulnerability
The burden of intersectionality between disability and the age of adolescence has been reported as the frontline barrier for accessing SRH services. Some participants explained their poor sexual and reproductive health-related outcomes in accordance with the challenge of facing double marginalization in accessing the services. A student with physical disability stated the burden of intersectionality as “Since I’m now at school, I have the opportunity to hear something from my friends and healthcare providers, but after I saw my first menstruation and felt the stress, I always worry for deaf girls in our village who haven’t heard any solution yet in their lives.”- IDIP 07, female
Another participant added; “… disability by itself is a difficult situation; when experienced in this turbulent, fiery age, the problem gets even worse.”- IDIP08, female “… Beyond living with disability, if we again acquire HIV or any sexually transmitted disease, we couldn’t cope with the situation at all, and then it will become an additional burden for the government too.” - IDIP04, male
Subtheme-2: Unmet Sexual and Reproductive Health Needs
The sexual and reproductive health service needs of young disabled study participants were overlooked due to multiple systemic, community-based, and personnel contributors. Despite the existing need, many participants reported that the absence of medical supplies and commodities at healthcare facilities increased their vulnerability to SRH problems. Additionally, lack of adolescent and disability-friendly approaches like distribution of condoms and post-pills at accessible areas coupled with the high medical cost, is found to be the cause for unmet need of SRH services for YPWDs.
One of the IDI participants stated as, “Previously, condoms were freely accessible everywhere in the hotels, pensions, health facilities, and youth centers, but nowadays it is totally absent. Some adolescents told me that they are practicing bare sex due to the unaffordable cost of condoms. One condom cost about 70 birrs (reported in January 2026 in the study area)” IDIP 04, male
Subtheme-3: The Desire for SRH Autonomy
Some young people with disabilities in this study expressed a strong aspiration for their SRH autonomy and informed voluntary decision-making capacity at healthcare facilities. They feel that they were poorly understood by healthcare providers. “I have experienced that while I went to the facility with my wife for family planning services, the providers push us to choose their long-acting FP preferences despite our needs” IDIP06, male
Theme 3- the Critical Role of Youth and Disability Networks
Under this major theme, two subsequent sub-themes, Peer and disability networks as important gateways to SRH access and Community solidarity, emerged from the analysis.
Sub-Theme-1 Peer and Disability Networks as Important Gateways to SRH Access
Participants expressed their views on the effectiveness of peer-led SRH discussions and awareness creation approaches on their tendency to access SRH services. The role of local organization of People with Disabilities (OPDs) in providing tailored SRH information for YPWDs has also been recognized by some of the study participants. “The local disability association in our district helped me to access sexual health-related and non-communicable disease prevention-related information during our monthly meeting.” - IDIP 01, female
Sub-theme-2 Community solidarity
All forms of community support and social inclusion activities are needed to improve health-seeking behaviors among YPWDs. They have reported that continued support from the family, community, and institutions is vital to deal with their SRH lives. “In the summertime, when roads to the facility become muddy, my fellow brothers usually assist me in reaching the facility for services.” - IDIP 01, female
Theme 4. Demands for tangible improvement in SRH inclusion
Young people with disabilities who participated in the study echoed the ultimate need for tangible sexual and reproductive health services accessibility for this marginalized segment of the population. They consistently described their aspiration for a better SRH inclusion through engaging SRH information and representation mechanisms, meaningful access via integrated outreach services, ensuring all year-round physical accessibility of health facilities and service provision rooms, and a separate disability friendly adolescent clinic.
Subtheme-1: Demands for Inclusive SRH Knowledge and Representation
Many YPWDs reported that they do not know many of the SRH services, the platform for obtaining SRH information, and the lack of representation in SRH advocacy. Participants revealed that disengagement from various disability-focused initiatives limited their decision-making power in their own SRH needs and rights. Moreover, the lack of different assistive devices in the healthcare setting aggravates the communication gap and service inaccessibility. A girl with visual impairment said: “Following my mother’s death, I go to the church early in the morning to beg from people for a living. I have no means to hear about sexual and reproductive health-related information.”- IDIP02, female
Another participant had this to add: “… wherever you go through the healthcare facilities, you may not find a single information and education poster representing people with disabilities. That’s why I’m saying that disability-inclusion is still on paper.” - IDIP 06, Male, government employed
Subtheme-2 Demands for competent Healthcare providers and Facilities
Healthcare facility arrangements and providers working in the SRH units of the facilities have been mentioned as barriers to obtaining SRH services by YPWDs. Participants noted that independent disability-friendly service providing units along with competent healthcare providers are required to ensure the provision of quality SRH service for YPWDs. “Healthcare facilities need to arrange independent blocks that are easily accessible by disabled individuals, more preferably around the entrance gate of the facility, rather than those with complex turns and difficult stairs.” – IDIP 04, Male
Subtheme-3: Demands for tangible SRH service accessibility
Most of the study participants described the need for meaningful accessibility of SRH services for YPWDs. Many of them spoke of their diminished ability to reach the facility as the road to the facility is not firm and functional all year round, and access to SRH services as they want. Roads to the facility are muddy; in some areas, there is no transportation to the facility, even for the non-disabled ones. “Though we are voiceless, I strongly insist all the relevant parties have firm and easy access to the facility,” IDIP 08, Female
Subtheme-4: Self-advocacy and role modelling successful PWDs
Some study participants argued that YPWDs lack an accurate understanding of their sexual and reproductive rights, do not advocate for their needs, and have limited engagement in decision-making. To cope with the existing under-representation, many of the study participants suggested active engagement of PWDs in all matters regarding their sexual and reproductive health. The importance of role modelling of successful people with disabilities is another area of insight mentioned by participants to navigate their experiences, challenge the negative societal stereotyping, and demonstrate that disability is not inability.
An IDI participant said: “…we young people with disabilities by ourselves should develop our confidence. We need to accept our disability status and accept the condition as normal.” (IDIP 04, Male)
Another participant had to say more: Umm … young people with disabilities have to think that they are capable of doing things as perfectly as their counterparts do; they can lead their family, run businesses, and even a country.” – IDIP 05, Female
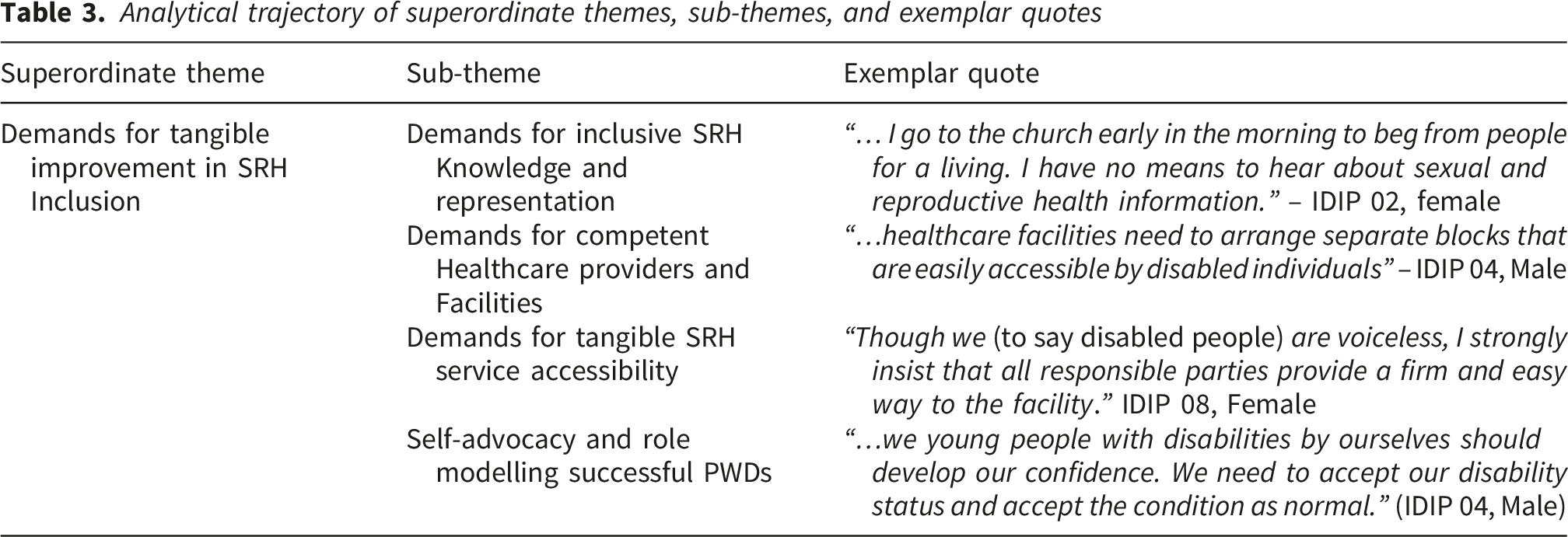
Analytical trajectory of superordinate themes, sub-themes, and exemplar quotes
Discussion
This study sought to answer the research question: What barriers and facilitating factors influence access to SRH services among YPWD in Ethiopia? By exploring participants’ lived experiences through IPA grounded in intersectionality theory, 22 the findings shed light on the profound and multi-layered interplay of barriers facing YPWDs regarding their SRH rights and service access in Ethiopia. The study findings confirm known barriers (e.g., physical inaccessibility, lack of transportation, discrimination, and lack of disability-inclusive provider training) while also contributing to new insights, including the SRH accessibility paradox, SRH autonomy demands, intersectional burden of disability and adolescence, and the call for tangible SRH inclusion.
This discussion synthesizes the four major themes that emerged from the study: The dualistic SRH access paradox, the intersectional burden of disability and adolescence, the critical role of youth and disability networks, and demands for tangible improvement in SRH inclusion. The discussion situated the thirteen subsequent sub-themes within the broader empirical evidence and disability policy frameworks.
The Dualistic SRH Service Access Paradox
The study findings revealed the existence of a fundamental paradox in sexual and reproductive health services access among YPWDs. Although national 37 and international38,39 policy frameworks recognize the right to equitable SRH services, our findings indicate that YPWDs continue to experience limited access. Some study participants recognized enabling factors such as the presence of dedicated SRH service rooms, maternal waiting homes, and free contraception access; yet many YPWDs still face several systemic gaps. The necessary structural pillars that create access remain systemically neglected, and the prevalent tokenistic inclusion often reinforces the marginalization of YPWDs. These findings broadly align with previous studies conducted in Ghana, 40 South Africa, 41 Uganda, 42 and Nepal, 43 underscoring the need for SRH and disability policy enforcement in Ethiopia through integrated leadership engagement.
The profound healthcare ableism(discrimination) and societal dehumanization against YPWDs make it difficult to have open SRH communication with healthcare providers, community members, and their families. Lack of prioritization mechanisms, difficulty of accessing service delivery rooms, and lack of effective communication within the healthcare setup, along with the subtle societal stereotyping, constrain YPWDs from accessing SRH services. This finding is in line with previous study findings.14,20,41,44 A qualitative study conducted in Addis Ababa disclosed that HCPs were very surprised when YPWDs sought to access SRH services. 18 Another systematic review and meta-analysis study in Ethiopia corroborates these findings, reporting a pooled estimate of 29.11%. 45 This finding highlights a need for the enforcement of global and national disability strategies on the ground, hastening the meaningful inclusion of YPWDs in the healthcare system by addressing the structural and attitudinal barriers. Provider capacity building on disability-inclusiveness, sign language, value clarification and attitude transformation, and rights-based SRH training should be cascaded to all SRH staff. Additionally, to resolve the SRH access paradox, it is essential to establish district-level youth disability councils to co-design, monitor, and evaluate SRH services, ensuring accountability from policy to practice.
Navigating the Intersectional Burden of Disability and Adolescence
Young people with disabilities’ narratives in this study reveal the existence of compounded vulnerability arising from the intersectional jeopardy of disability and adolescence, which heightens unmet needs and increases the risk of sexual and reproductive health (SRH) problems. Consistent with the study’s core theoretical underpinning, 22 the findings demonstrate that this intersectionality, shaped by both age-related and disability-related discrimination, creates additional barriers to access SRH services compared with their non-disabled peers in Ethiopia. The limited availability of tailored adolescent and disability-friendly SRH information and services for young disabled individuals, coupled with the unmet desire for SRH autonomy at healthcare facilities, puts them at a decreased probability of accessing SRH services, suggesting that the healthcare system is not designed to meet the developmental needs of YPWDs. This finding contradicts Article 25 of the United Nations Convention on the Rights of Persons with Disabilities (UNCRPD) that mandates the health system to provide equitable access for inclusive SRH services for PWDs. 46 To monitor the progress, disability-disaggregated indicators must be integrated into the routine health information system to timely track service utilization patterns across disability types.
The desire for SRH autonomy expressed by participants in this study directly resonates with the paternalistic attitudes present at health facilities where caregivers and HCPs make SRH decisions for YPWDs rather than supporting them to exercise informed voluntary decision-making (IVDM) practice. This finding is supported by previous studies from multiple sub-Saharan countries, 20 Ghana, 47 and Tanzania. 48 This gap underscores the need for implementing inclusive, adolescent, and disability-responsive SRH programs that ensure accessible information, trained providers, and active engagement of YPWDs in the design and delivery of SRH services in Ethiopia.
Strengthened Youth and Disability Networks as Enablers
The findings of this study extend beyond revealing the limited access of SRH services to identifying peer and disability networks as vital pipelines for accessing SRH services by YPWDs. Young people with disabilities’ ability to access SRH services at healthcare facilities was subject to the presence of peer and or disability networks in their residency. Young people who have access to engage in a peer education program were more likely to utilize the services than those without access. Similarly, YPWDs who are enrolled in Organizations of Persons with Disabilities (OPDs) were more likely to obtain SRH information and services than those without local engagement with OPDs. Findings show that most of the study participants were unable to access local engagement to peer-to-peer SRH education programs, and never enrolled in OPDs, leading to limited SRH service utilization. Likewise, the SRH service uptake of YPWDs was dependent on the existing family and community support. Most YPWDs reported that they were not accessing adequate family and community support to discuss SRH issues and were frequently obliged to hide their SRH needs.
This study finding is supported by previous studies conducted in Ethiopia,19,49 Ghana, 50 and Zambia. 51 A CRCT study conducted in Zambia reported a 63.8% SRH service utilization among intervention groups (who received peer-led education) compared to a 5.4% service uptake in the control group. 51 A recent implementation research conducted by Ipas Ethiopia supports this finding by demonstrating that peer education and integrated youth leadership significantly improved SRH service utilization. 52 This study finding indicates the need for an integrated peer education system and community solidarity, supported by regular value clarification and attitude transformation (VCAT) trainings and community-based coffee ceremony activities, to enhance YPWD engagement in SRH awareness sessions. Moreover, to strengthen ownership among YPWDs, the establishment of regional- and district-level youth with disability councils and associations are necessary.
Demands for Tangible Improvement in SRH Inclusion
Beyond consistently listing grievances regarding SRH access barriers, YPWDs participating in the current study state a clear set of demands for tangible and actionable strategic changes. The fourth theme goes far from describing the barriers to articulating tangible solutions towards the improvement of SRH access for YPWDs.
Study participants strongly emphasized the need for inclusive SRH knowledge and representation, underscoring the persistent exclusion of YPWDs from mainstream information and education channels. Consistent with previous literature,17,18 the need for inclusive SRH knowledge and representation of YPWDs originates from the limited inclusivity of SRH education materials, leaving many YPWDs unaware of their SRH rights and available services. The call for inclusive SRH knowledge by YPWD’s in the current study resonates with previous research findings in Jima that reports only 21.4% of YPWDs were aware of the presence of SRH services, 14 and another study conducted in Dessie reported that disabled youths with poor SRH knowledge were 90% less likely to use the services than participants with good knowledge. 13 The under-representation of YPWDs in SRH matters also contributes to the societal misunderstandings that PWDs are not entitled to enjoy their sexual and reproductive lives or are considered asexual. This finding highlights the persistent gap in disability-inclusive advocacy approaches that need to be addressed through proper design of integrated adolescent and disability-inclusive content in community awareness creation, mainstream SRH information platforms, social media, and disability inclusive school curricula.
In agreement with prior research,13,44 another key finding in this study underlines YPWDs’ aspiration for competent HCPs and disability inclusive health facilities. Study participants reported difficulty of communication with HCPs (absence of sign language trained providers), limited access for making informed SRH decisions, providers lacking necessary skill trainings (e.g., safe abortion), providers’ negative attitude, and lack of access to service provision rooms, whereby the safety and confidentiality of YPWDs are maintained in the facility. The demand for competent providers and facilities is empirically supported with previous studies documenting positive provider attitude, 18 sign language training, 48 and skill-based professional development measures, 52 which constitute key enabling factors for SRH service utilization among YPWDs. This finding spotlights the persistent technical and attitudinal gaps associated with providers and the respective health facilities’ management systems. Thus, the finding implies the need for a structured facility-based gap identification system for the provision of skill-based SRH technical trainings, sign language trainings, and VCAT trainings for providers working on SRH rooms. This finding amplifies YPWDs’ aspirations to be represented in SRH education and awareness creation platforms.
Young people with disabilities expressed a strong demand for improved SRH services access, including physical, financial, and outreach services. Recent evidence in Ethiopia substantiated the effectiveness of modification of facilities, including ramps, signage, toilets, and arrangement of regular community outreach services to enhance inclusive and equitable SRH utilization. 53 Likewise, previous research conducted in South Africa, 54 Tanzania, 48 Uganda, 42 and Kenya 55 demonstrates that the presence of physical and financial barriers continues to exclude YPWDs from accessing SRH services. The finding implies a clear gap in balancing the demand and supply of SRH services for YPWDs in Ethiopia, informing urgent reinforcement of the national SRH and disability strategies targeting to expand outreach, provide affordable services, and actively involve YPWDs in planning and advocacy.
Study participants emphasized the importance of self-advocacy and role modelling of successful PWDs. YPWDs’ substantial exposure to empowered individuals with disabilities is reported as an instrumental means to build confidence, tackle societal stereotyping, and share positive SRH experiences. Evidence suggests that enhancing self-advocacy among PWDs builds a high sense of subjective well-being and positive relationships crucial in challenging the existing discriminatory attitudes and societal assumptions that PWDs are incapable of making decisions on their own health and social relationships. 56 However, despite global commitment to disability and adolescent inclusion, YPWDs in many settings lack such participation opportunities. This shows a critical system gap in creating the medium for YPWDs to build a high sense of subjective well-being and positive relationships. This finding, therefore, informs the need for responsive health programming involving the establishment of peer-led advocacy groups, peer mentorship programs, and partnering with and strengthening of disability-led organizations to enhance collective advocacy and shared accountability within the health system.
Strengths and Limitations of the Study
This study demonstrates a scientific way of exploring the lived experiences of YPWDs in accessing SRH services, a topic underexplored in Ethiopia and sub-Saharan countries. Through an interpretative phenomenological analysis approach, the study contributes to the growing body of evidence centering the voices of young disabled individuals, emphasizing the end of double marginalization through multi-level comprehensive enhancement of disability inclusive health systems.
However, the study findings should be interpreted by considering the limitations. The study recruited a relatively small sample size, which may limit the generalizability of the findings in similar contexts. Study participants having only physical and visual impairments were taken from two districts, which may not fully reflect the diverse experiences of YPWDs having different forms of disability across different geographic areas. Future researchers in this area should prioritize accessible and inclusive methodologies to include the voices of young people with hearing, mental, and cognitive disabilities in Ethiopia. Despite these limitations, the study provides contextual insights that can inform future research, policy, and programs aimed at improving equitable access to SRH services.
Conclusion
This study navigates the profound marginalization of YPWDs in accessing SRH services in Ethiopia. The existence of inequitable SRH service access, unmet SRH autonomy, intersection burden of disability, and adolescence. Though the pervasive systemic neglect, YPWDs by themselves are articulating clear and actionable eternal demands, revealing the source of resilience and hope. The healthcare system must dismantle dehumanizing societal attitudes, establish and strengthen community networks, including peer-led education programs, and strengthen the OPDs to respond to YPWD’s demands for inclusive SRH access through competent HCPs; thereby ensuring their SRH rights in Ethiopia.
Supplemental Material
Supplemental Material - The Lived Experiences of Young People With Disabilities in Accessing Sexual and Reproductive Health Services in Ethiopia: An Interpretative Phenomenological Analysis
Supplemental Material for The Lived Experiences of Young People With Disabilities in Accessing Sexual and Reproductive Health Services in Ethiopia: An Interpretative Phenomenological Analysis by Mihiret Tesfaw, Takele Tadesse, Kassa Daka and Amene Abebe in Inquiry: The Journal Of Health Care Organization, Provision, And Financing.
Supplemental Material
Supplemental Material - The Lived Experiences of Young People With Disabilities in Accessing Sexual and Reproductive Health Services in Ethiopia: An Interpretative Phenomenological Analysis
Supplemental Material for The Lived Experiences of Young People With Disabilities in Accessing Sexual and Reproductive Health Services in Ethiopia: An Interpretative Phenomenological Analysis by Mihiret Tesfaw, Takele Tadesse, Kassa Daka and Amene Abebe in Inquiry: The Journal Of Health Care Organization, Provision, And Financing.
Footnotes
Acknowledgment
We thank all study participants who took part and shared their lived experiences and perspectives in the study.
Consent to Participate
Informed consent was secured from all participants.
Authors Contribution
Conceptualization, M.T. and T.T., methodology, M.T., A.A, T.T, and K.D. Software, M.T., A.A.; formal analysis, M.T., A.A., T.T., and K.D.; writing-original draft preparation, M.T; writing, review and editing, M.T., A.A., T.T., and K.D. All authors have read and agreed to the current version of the manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article
Data Availability Statement
All data used for the analysis in this study are available upon reasonable request of the corresponding author.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.