
Abstract
Introduction
Digital therapeutics (DTx) represent an emerging class of software-based medical devices delivering evidence-based therapeutic interventions. Several countries have developed regulatory and reimbursement frameworks for DTx, while Korea’s evaluation system remains in its early stages. This scoping review compared regulatory and reimbursement frameworks for DTx across the United States, Germany, the United Kingdom, and Korea, and separately derived author-led policy implications for a Korean DTx evaluation framework.
Methods
Following the Arksey and O'Malley framework and PRISMA-ScR guidelines, we searched 11 databases for literature published between January 2015 and December 2025 (final search: 15 February 2026). DTx was operationalized using the Digital Therapeutics Alliance anchor definition with jurisdiction-specific application rules. Data were synthesized along five analytical dimensions: regulation, evidence assessment, reimbursement, postmarket evidence, and governance linkage.
Results
Of 2,847 records, 42 sources (19 articles, 23 policy documents) were included. Jurisdictions diverged most clearly on statutory codification of DTx, the existence of a dedicated reimbursement pathway, and regulator–payer integration. Germany’s DiGA Fast-Track had 61 products listed cumulatively (50 active, 11 removed), exceeding one million prescriptions and €234 million expenditure (GKV-SV reporting period through 31 December 2024). Korea provisionally listed four DTx products since 2023.
Conclusions
Germany’s DiGA system shares more institutional features with Korea’s evolving system than do the US or UK frameworks. We propose, as an author-derived synthesis informed by the review, a five-phase Korean DTx framework, while acknowledging substantive system-level differences (payer pluralism, pricing, benefit design, HTA procedure) that constrain direct transferability.
Keywords
Introduction
The global healthcare landscape has undergone accelerated digital transformation since the COVID-19 pandemic.1,2 Digital therapeutics (DTx) have emerged as a distinct innovation class — software-based, evidence-driven therapeutic interventions differentiated from conventional pharmaceuticals and medical devices.3-5 The Digital Therapeutics Alliance (DTA) defines DTx as software as a medical device (SaMD) delivering evidence-based therapeutic interventions for prevention, management, or treatment of disease, requiring clinical trial evidence and regulatory approval.3,6,7
Several countries have developed dedicated DTx frameworks. The US Food and Drug Administration (FDA) launched the Digital Health Innovation Action Plan 8 ; Germany enacted the Digital Healthcare Act establishing the DiGA Fast-Track (a dedicated regulatory and reimbursement pathway for digital health applications under statutory health insurance) 9 ; and the UK’s National Institute for Health and Care Excellence (NICE) published the Evidence Standards Framework (ESF), which sets tier-based evidence expectations for digital health technologies. 10 Germany achieved the world’s first statutory health insurance reimbursement for DTx, with cumulative prescriptions exceeding one million by late 2024. 11
Korea designated digital healthcare as a national competitiveness pillar, 12 yet its DTx evaluation and reimbursement systems remain at an early stage.13-15 The innovative medical technology integrated review and provisional listing system was introduced in 2023, 16 but institutional gaps persist: DTx-specific legislation is absent; reference pricing is considerably lower than international comparators; and governance is fragmented across multiple agencies. As an illustrative example, Somzz is priced at KRW 25,390 per 90-day course, whereas the DiGA median initial price is approximately €514 per 90-day activation period. This pricing comparison is illustrative rather than directly equivalent.
This scoping review pursues two epistemically distinct objectives, kept separate throughout. First, as a review-level objective, we describe and compare the regulatory and reimbursement structures of DTx across the four jurisdictions (Section 4). Second, as an author-led interpretive objective informed by — but not directly produced by — the review, we present a comparative synthesis (Section 5) and propose policy implications for Korea (Section 6). Comparators were selected because they represent three distinct healthcare-financing models — multi-payer market-based (US), multi-payer statutory health insurance (Germany), and tax-financed national health service (UK) — and each pioneered DTx-specific regulatory mechanisms. We note that Germany operates a multi-payer SHI system with approximately 95+ statutory sickness funds (Krankenkassen), NOT a single-payer system; Korea, by contrast, is a single-payer SHI system with the National Health Insurance Service (NHIS).
Methods
This scoping review followed the framework of Arksey and O'Malley 17 as enhanced by Levac et al. 18 , and adhered to PRISMA-ScR guidelines. 19 Critical appraisal of included sources was not performed, consistent with scoping review methodology. The completed PRISMA-ScR checklist accompanies this submission as Supplementary File 1.
Operational Definition of DTx Across Jurisdictions
Because DTx terminology is not standardized internationally, we applied a two-layer operational definition. The unifying anchor was the DTA (2018) definition. 3 Jurisdiction-specific application rules were: United States — prescription digital therapeutics (PDTs) and SaMD products meeting the DTA anchor; Germany — DiGA listed in the BfArM §139e directory under DVG/DiGAV/DigiG9,20-22; United Kingdom — digital health technologies stratified at NICE ESF Tier 3a/3b only (broader Tier 1–2 tools excluded unless the source addressed therapeutic-tier policy) 10 ; Korea — “digital therapeutic device” under MFDS guideline (2020) and the Digital Medical Products Act (DMPA, 2024).23,24 NICE ESF is broader than DTx, whereas DiGA is a specific reimbursable category — this conceptual difference was tracked. Broader policy documents were included only where DTx-relevant content was extractable; a borderline-decision log of 14 sources is provided as Supplementary File 2.
Source Inclusion Criteria
Inclusion and exclusion criteria followed the Population, Concept, Context (PCC) framework. 19 Population: DTx researchers, policymakers, industry stakeholders, healthcare providers. Concept: DTx regulatory approval, evaluation, reimbursement, and clinical-evidence requirements. Context: Korea-focused or international comparative studies involving the US, Germany, or UK. Eligible sources included peer-reviewed articles and government/institutional policy documents in English or Korean published between January 2015 and December 2025. We excluded studies on individual DTx clinical outcomes without regulatory/reimbursement focus, studies on general digital health solutions not meeting the DTx operational definition, conference abstracts, editorials, and correspondence. Each source was coded against one analytical dimension where possible, to prevent double-counting in the comparative synthesis.
Search Strategy
Six international databases (CINAHL, Cochrane Library, Embase, MEDLINE via Ovid, Scopus, Web of Science) and five Korean databases (KISS, KMBASE, KoreaMed, RISS, ScienceON) were searched (final search: 15 February 2026). Database searches were systematic; institutional database searches (FDA, BfArM, NICE, HIRA, MFDS, NECA) were targeted/purposive, restricted to DTx-relevant directories and guidance documents, and complemented (not replaced) the systematic searches. The full search strategy with database-specific strings is in Supplementary File 3. The 2015 start year was chosen because (i) FDA Medical Device Data Systems guidance and digital-health regulatory discussions began in 2015, (ii) early PDT developers entered formal regulatory engagement around 2014–2015, and (iii) the canonical DTA (2018) definition was applied retrospectively to pre-2018 sources, with borderline cases flagged. A sensitivity analysis restricting to ≥2018 sources (n=37 of 42) yielded substantively unchanged findings.
Source Selection
Two reviewers independently screened titles/abstracts then full texts. Cohen’s kappa was 0.84 at title/abstract and 0.91 at full-text screening. Disagreements were resolved by discussion; unresolved cases referred to a third reviewer. The selection process is shown in Figure 1 (PRISMA-ScR flow diagram). PRISMA-ScR flow diagram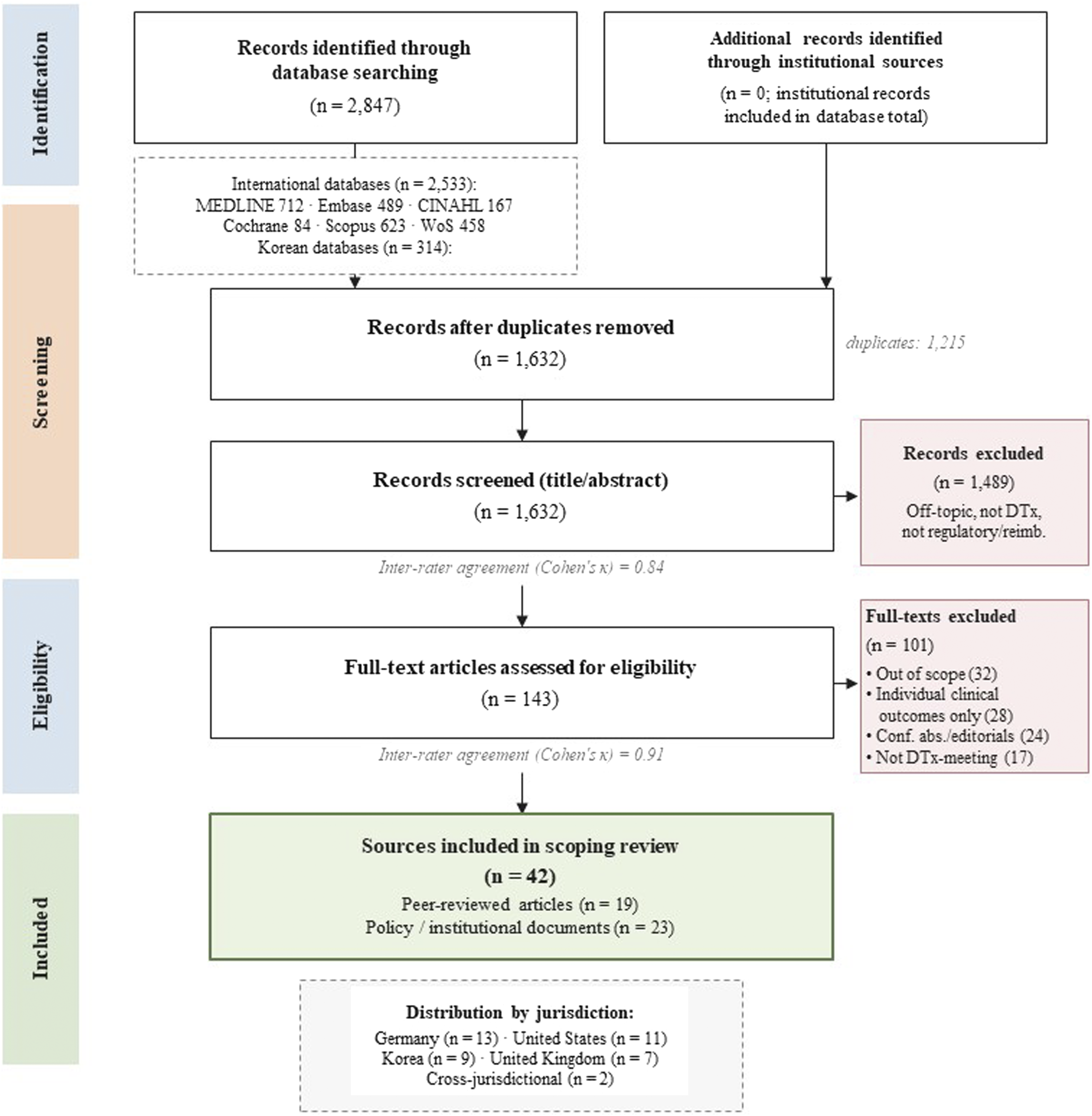
Data Charting and the Five-Dimension Analytical Framework
A standardized data-charting form was pilot-tested on five sources. To address conceptual non-equivalence across jurisdictions, extracted data were organized along five distinct analytical dimensions, each treated as a separate axis: (1) Regulation — authorization, certification, and classification mechanisms; (2) Evidence assessment — clinical-evidence and effectiveness-evaluation criteria; (3) Reimbursement — listing and payment structure; (4) Postmarket evidence — post-listing evidence generation, real-world evidence, and re-evaluation; (5) Governance linkage — institutional coupling between regulator, payer, and HTA bodies. Synthesis followed the three-stage thematic synthesis approach of Thomas and Harden. 25 Within each dimension, country-level descriptive findings were charted first; cross-country comparative interpretations and policy implications were drawn only thereafter.
Included Evidence Characteristics
Of 2,847 records, 1,215 duplicates were removed; 1,632 records underwent title/abstract screening; 143 full texts were assessed; and 42 sources were included (19 peer-reviewed articles, 23 policy documents/institutional reports). The PRISMA-ScR flow diagram is shown in Figure 1. Source distribution by jurisdiction: Germany (n=13), United States (n=11), Korea (n=9), United Kingdom (n=7), cross-jurisdictional (n=2). Source-type distribution differed by country: peer-reviewed articles predominated for the US and Germany, whereas Korean sources were predominantly policy and institutional reports — a distribution itself relevant to the limitations.
Country-specific Regulatory and Reimbursement Pathways
The findings in this section are descriptive results of the scoping review. Cross-country comparative synthesis is in Section 5; author-derived policy implications are in Section 6.
Germany — DiGA System
Germany enacted the DVG in November 2019, establishing a legal basis for reimbursing DiGA under the multi-payer SHI system in which approximately 95+ Krankenkassen provide coverage under the centrally defined benefit catalogue.9,26 The DiGA Fast-Track enables manufacturers to apply for directory listing through BfArM. Provisionally listed DiGA have 12–24 months to demonstrate a positive care effect (positive Versorgungseffekt, pVE) through medical benefit (medizinischer Nutzen, mN) or patient-relevant structural and procedural improvements (patientenrelevante Struktur-und Verfahrensverbesserung, pSVV).20,21 As of 15 February 2026, 61 products had been listed cumulatively in the BfArM DiGA directory; 50 were active and 11 had been removed. Cumulative prescriptions exceeded one million and reimbursement expenditure reached €234 million during the GKV-SV reporting period 1 September 2020 – 31 December 2024.11,27,28 Removed products primarily failed to demonstrate pVE within the provisional period. 29 Under DigiG (2024), the framework will expand to Class IIb devices, mandate continuous outcome measurement (Anwendungsbegleitende Erfolgsmessung, AbEM), and shorten insurer activation code issuance from 14 to 2 days. 22
United States — FDA/Multi-Payer Reimbursement
The FDA operates the Digital Health Center of Excellence and applies the SaMD Risk Framework to DTx. 8 DTx products typically enter the market via 510(k), De Novo, or PMA. The multi-payer reimbursement structure creates a structural disconnect between regulatory approval and reimbursement. 30 Centers for Medicare and Medicaid Services (CMS) coverage relies on Category III CPT codes, the New Technology Add-on Payment for hospital settings, and transitional pass-through; commercial-payer coverage is plan-by-plan and varies by state Medicaid policy. Recent commercial-payer pilots include Highmark and Blue Shield of California PDT initiatives. The 2023 bankruptcy of Pear Therapeutics, despite FDA clearance for three DTx products, is reported as illustrating the consequences of regulatory approval without sustainable reimbursement.31-34
United Kingdom — NICE ESF/NHS
NICE’s ESF (2019, updated 2022) stratifies digital health technologies by functional classification, applying proportionate evidence requirements across Tiers 1–3b.10,35,36 ESF operates alongside the Digital Technology Assessment Criteria (DTAC) used by NHS England for system-level due diligence, and the NHS Apps Library/ORCHA review. The NHS Improving Access to Psychological Therapies program facilitated early DTx integration in mental health care. In 2023–2024 NICE introduced the Early Value Assessment (EVA) route and subsequently the HealthTech Guidance (HTG) format. In January 2026, NICE issued HTG for eating-disorder digital self-management and hip/knee osteoarthritis digital management. 37 The ESF operates as guidance without statutory enforcement; NHS adoption is determined locally by commissioning structures.
Korea — Innovative Medical Technology System
Korea initiated its innovative medical technology integrated review system in 2023, aiming to reduce DTx market entry timelines from 390 to 80 days through concurrent MFDS, HIRA, and NECA assessments. 16 As of July 2025, 18 technologies had been designated (14 AI-based, 4 DTx). 38 DTx products with provisional listing include Somzz (chronic insomnia CBT-I; June 2023–May 2026), Welt-I/Welt-IP, and Vivid Brain (post-stroke visual rehabilitation).39,40 Provisional listing reference prices (Somzz KRW 25,390 per 90-day course; Welt-I KRW 21,660) are administered ex-ante reference prices set by HIRA, distinct from manufacturer-set free pricing during the DiGA provisional period. HIRA commenced formal listing review in 2025, targeting formal listing by late 2026 or early 2027. 39
Comparative Synthesis Across the Five Analytical Dimensions
Cross-Country Overview Across the Five Analytical Dimensions
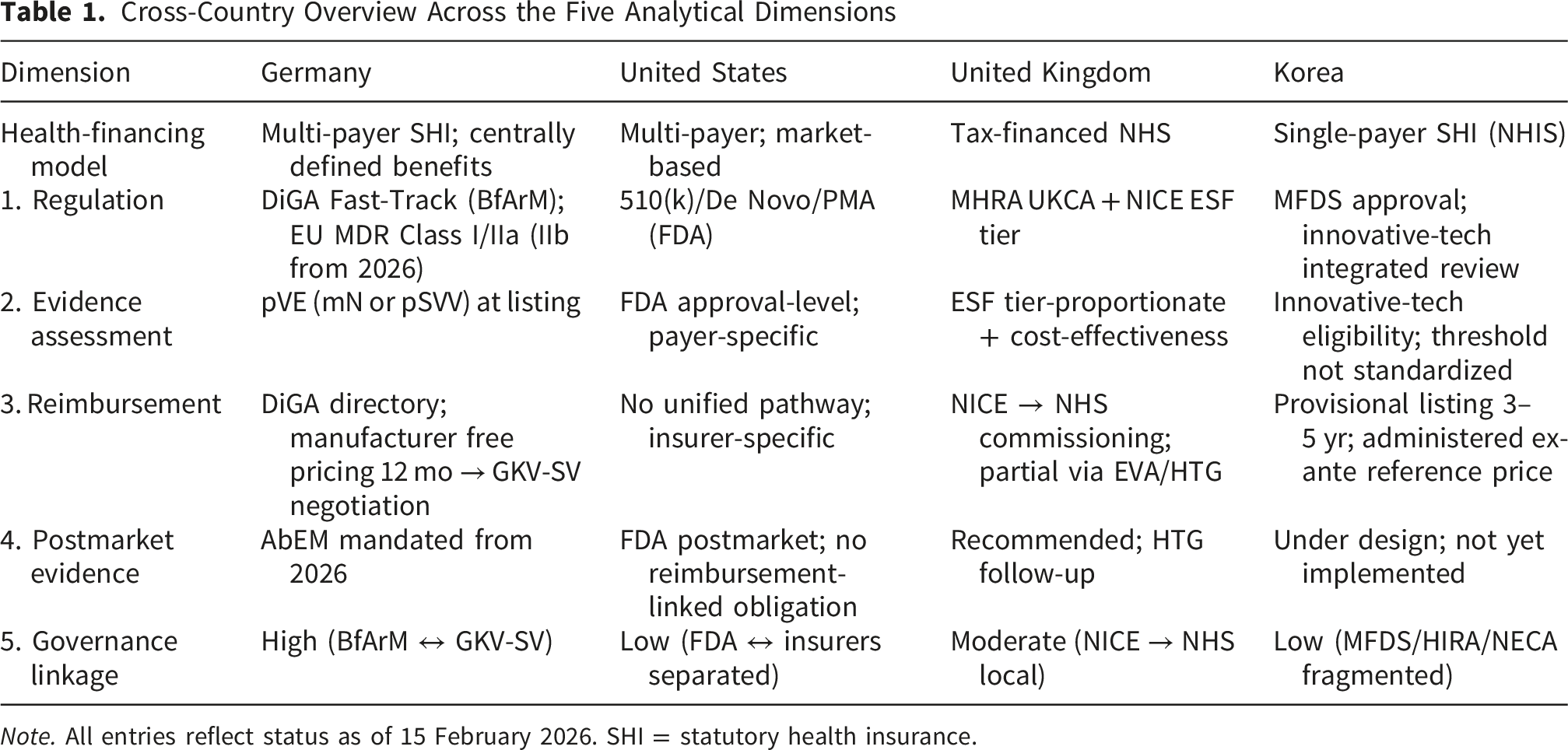
Note. All entries reflect status as of 15 February 2026. SHI = statutory health insurance.
Regulation
Regulatory authorization is the most institutionally mature dimension; all four jurisdictions have functioning DTx market-entry pathways. The principal axis of divergence is statutory codification of DTx as a distinct category. Germany codified DiGA at the statute level (DVG §33a; SGB V §139e). 41 The US codifies SaMD at statute level (FD&C Act, 21st Century Cures Act); the UK ESF operates as guidance without statutory enforcement; Korea relied on MFDS guideline until the DMPA (2024) provided a general (not DTx-specific) legal foundation. As the included US sources show, regulatory approval without secured reimbursement can lead to commercial failure (Pear Therapeutics).
Evidence Assessment
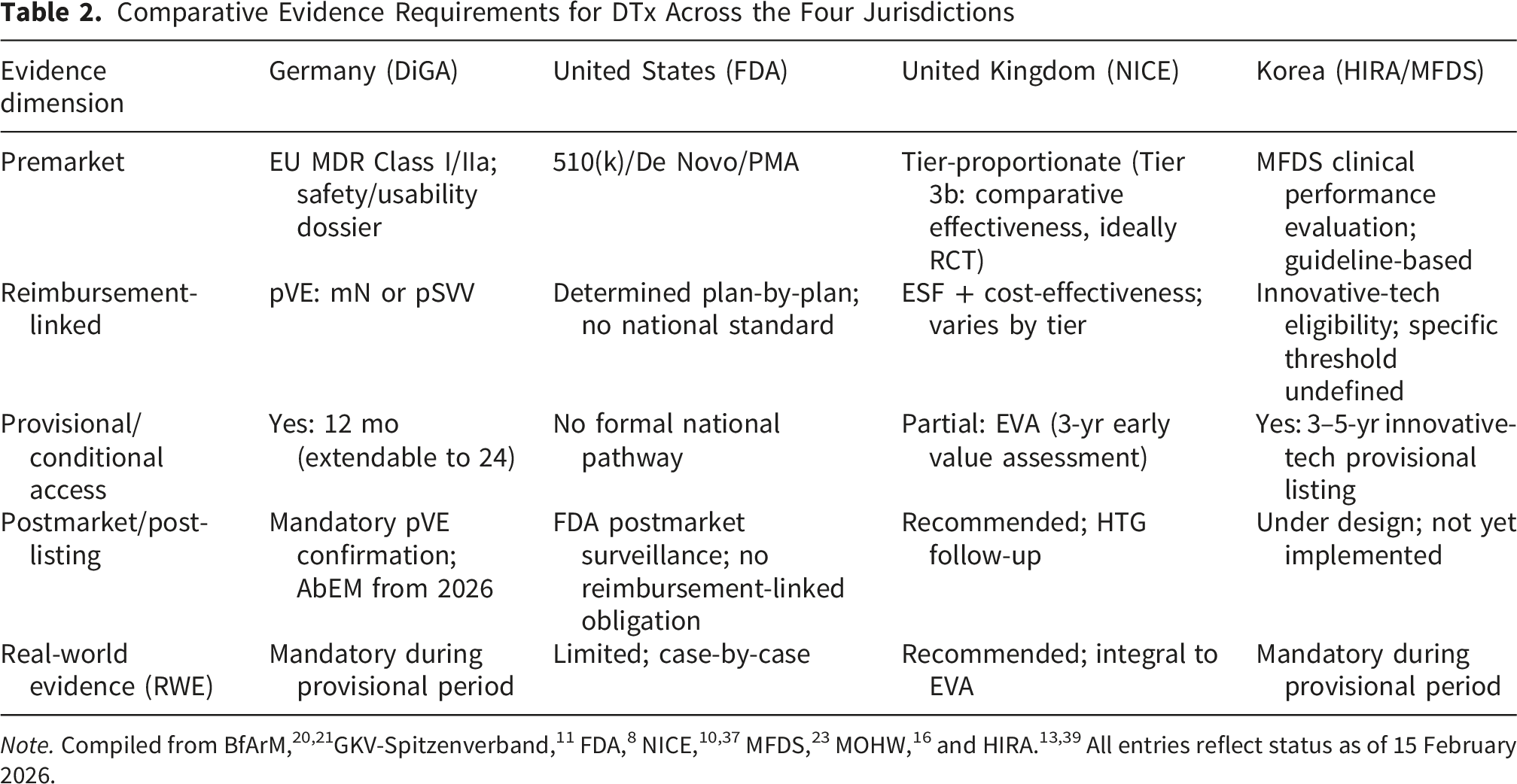
Comparative Evidence Requirements for DTx Across the Four Jurisdictions
Reimbursement
Reimbursement is the dimension on which jurisdictions diverge most starkly. Only Germany operates a DTx-specific reimbursement pathway integrated with regulatory listing. The US lacks a unified DTx-specific pathway; coverage is plan-by-plan. The UK funds digital health primarily through standard NHS commissioning. Korea operates a provisional-listing pathway, but with administered ex-ante reference pricing rather than DiGA-style manufacturer-set free pricing.
Postmarket Evidence
Only Germany formally couples postmarket evidence to reimbursement continuation (AbEM, from 2026). The UK’s HTG follow-up review provides a partial postmarket function. The US has FDA postmarket surveillance but no reimbursement-linked postmarket-evidence requirement. Korea’s postmarket framework is under design but not yet implemented. The German experience (11 DiGA removals) suggests that a credible exit mechanism, paired with a credible entry mechanism, is institutionally important.
Governance Linkage
Germany shows tight regulator–payer integration (BfArM evaluates; GKV-SV reimburses on that basis); the UK shows moderate integration (NICE → NHS commissioning, with local discretion); the US shows low integration (FDA approval is structurally separated from payer decisions); Korea shows low integration (MFDS, HIRA, NECA operate with distinct mandates, although the innovative medical technology integrated review is intended to reduce fragmentation). We interpret this dimension as the strongest predictor among the five—more so than regulation alone—of whether regulatory approval translates into reimbursable market access. This pattern is visible in both the Pear Therapeutics case (US) and the Korean pattern of non-reimbursed retail launches.
Policy Implications for Korea
The proposals below are explicitly author-derived: informed by, but not directly produced by, the scoping review evidence in Sections 4–5. The inferential step from comparative description to policy prescription requires interpretive judgment beyond what scoping-review evidence can independently support.
Korea–Germany Comparison: Bounded Structural Similarity
Among the comparators, Germany shares more institutional features with Korea’s evolving system than do the US or UK frameworks: both define DTx-related benefits at a statutory or quasi-statutory level, both operate centralized payer-side decision-making (GKV-SV/NHIS), and both implement a provisional-listing-with-evidence-generation logic. Substantive differences constrain direct transferability: (a) payer structure — multi-payer SHI (DE) vs single-payer SHI (KR); (b) pricing process — manufacturer free pricing then GKV-SV negotiation (DE) vs administered ex-ante reference price (KR); (c) benefit design — G-BA (DE) vs HIRA (KR); (d) HTA procedure — distinct statutory linkage (NECA vs BfArM–GKV-SV chain). DiGA is therefore presented as a structurally relevant reference for selected design choices, NOT a directly transferable model. The Korea–Germany pricing comparison (Somzz KRW 25,390 vs DiGA median ∼€514, both per 90-day course) is illustrative — intended to convey relative price level under non-equivalent pricing mechanisms, not as directly equivalent unit-price comparison.
Author-Derived Five-phase Korean DTx Evaluation Framework
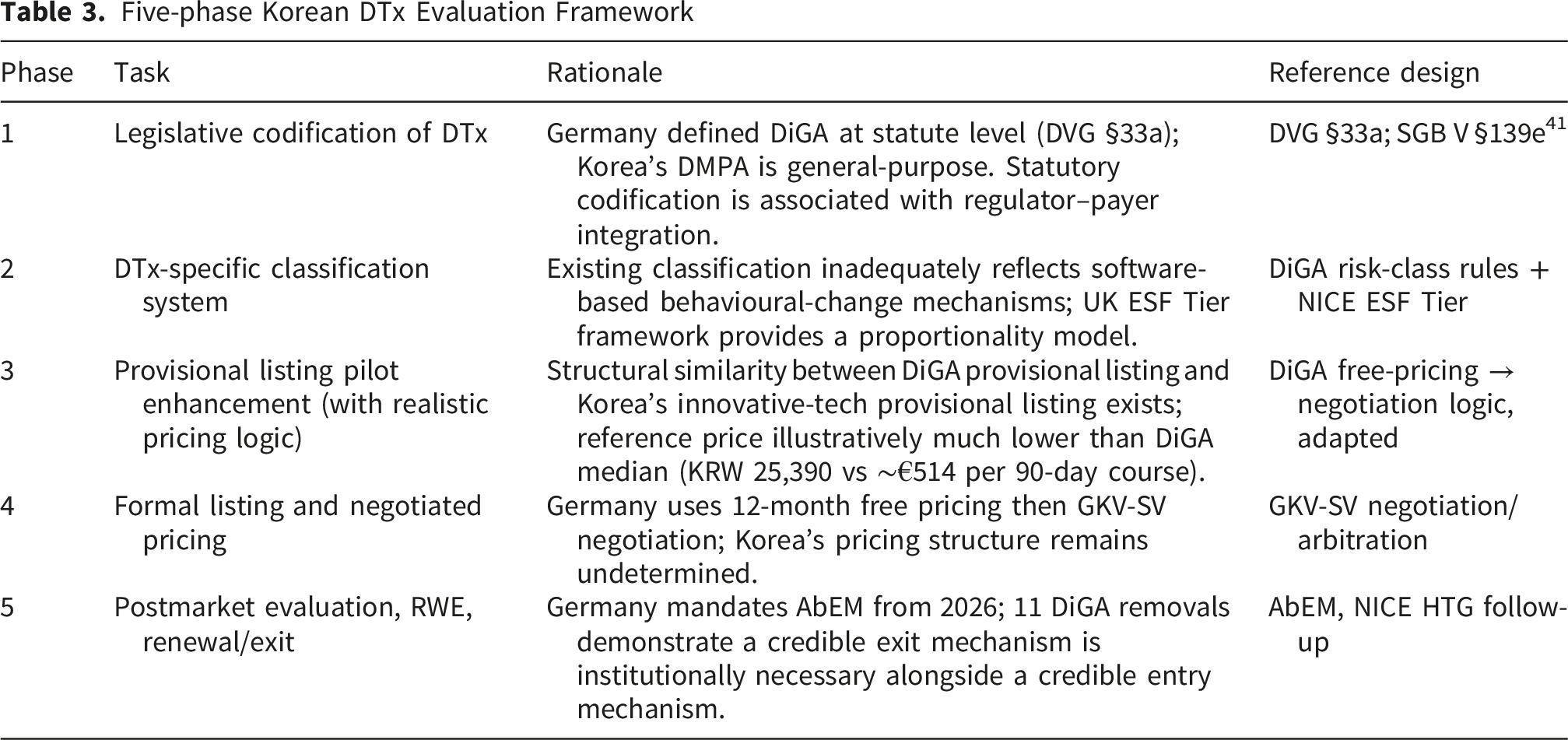
Five-phase Korean DTx Evaluation Framework
Implementation Mechanisms
Concrete operational suggestions: (a) Pricing — phased free-pricing-then-negotiation adapted from DiGA, with ceiling-discount band, transparency disclosure, and value-based reassessment at 12 and 24 months; (b) Ethics review — a dedicated DTx ethics-review subcommittee under the existing IRB framework, with explicit competencies for software updates, algorithmic change, and data protection; (c) Stakeholder consultation — a multi-ministerial working body (MOHW, MFDS, HIRA, NECA, MoTIE) operating with a structured public-consultation procedure modelled on G-BA and on NICE topic-selection processes; (d) Workforce — a tiered curriculum for advanced practice nurses, school health nurses, and community health nurses.
Industry Perspectives
Within the included sources, manufacturer-side perspectives recur as a determinant of pathway uptake. In Korea, several developers opted for non-reimbursed retail pricing rather than provisional listing, reflecting concerns that reference-price levels did not allow recovery of development cost. 39 In the US, the post-Pear-Therapeutics period has been associated with a chilling effect on PDT investment and increased emphasis on commercial-payer engagement before FDA submission. 32 In Germany, manufacturers raised concerns about the 12-month free-pricing window narrowing under stricter post-listing renegotiation rules in DigiG.22,28 In the UK, SMEs report compliance burden from parallel ESF/DTAC/NHS Apps Library reviews. 42 This synthesis draws from policy commentary and case-based sources within the included set, not primary stakeholder interviews.
Health Workforce Competency
We retain workforce as one of five priority recommendations, grounded in six included sources that explicitly raise workforce/prescriber competency as a determinant of DTx adoption.13,15,32,43-45 Germany’s DiGA pathway grants prescribing authority to physicians and psychotherapists.43,44 This recommendation is an author-derived extension informed by these sources rather than a direct review finding. Korea should develop training curricula for advanced practice nurses, school health nurses, and community health nurses to support DTx prescribing assistance, patient education, and adherence monitoring.
Limitations
Several limitations should be noted. First, consistent with scoping review methodology, methodological quality appraisal of included sources was not performed.17,19 Second, English- and Korean-language inclusion may have excluded relevant German-language primary sources. Third, Japan, Australia, France, and Belgium were not included as comparators. Fourth, systematic limitations in grey-literature selection remain. Fifth, the rapidly evolving DTx policy landscape means post-analysis developments may not be captured. Sixth, scoping reviews compare partly non-equivalent policy constructs across jurisdictions; despite our explicit operational definition and five-dimension framework, residual conceptual asymmetries (e.g., NICE ESF as guideline vs DiGA as statutory entitlement) cannot be fully eliminated. Seventh, much of the comparative source base consists of policy documents and grey literature, especially for Korea. Eighth, outcome-level data are limited for the UK and Korea, where DTx implementation experience is short. Ninth, publication and reporting bias may favour jurisdictions with established English-language policy analyses (notably Germany).
Conclusion
This scoping review analyzed 42 sources comparing DTx regulatory and reimbursement frameworks across the US, Germany, the UK, and Korea along five distinct analytical dimensions. Across these dimensions, Germany’s DiGA Fast-Track shares more institutional features with Korea’s evolving system than do the US or UK frameworks, while substantive system-level differences (payer pluralism, pricing mechanism, benefit design, HTA procedure) constrain direct transferability. Korea’s innovative medical technology integrated review and provisional listing system represents a meaningful initial pathway, but addressing reference pricing levels considerably lower than international comparators and developing a standardized DTx-specific evaluation framework remain priorities. We propose, as an author-derived synthesis, five priority policy tasks: legislative codification, provisional listing pilot enhancement with realistic pricing, health workforce competency development, multi-ministerial coordination, and component-specific evaluation criteria. These proposals are intended as a policy reference for Korea and for other countries designing DTx reimbursement within statutory health insurance systems.
Supplemental Material
Supplemental Material - Divergent Regulatory and Reimbursement Pathways for Digital Therapeutics: A Scoping Review With Implications for Korea
Supplemental Material for Divergent Regulatory and Reimbursement Pathways for Digital Therapeutics: A Scoping Review with Implications for Korea by Mincheol Kim, and Gaeun Kim in INQUIRY: The Journal of Health Care Organization, Provision, and Financing.
Supplemental Material
Supplemental Material - Divergent Regulatory and Reimbursement Pathways for Digital Therapeutics: A Scoping Review With Implications for Korea
Supplemental Material for Divergent Regulatory and Reimbursement Pathways for Digital Therapeutics: A Scoping Review with Implications for Korea by Mincheol Kim, and Gaeun Kim in INQUIRY: The Journal of Health Care Organization, Provision, and Financing.
Supplemental Material
Supplemental Material - Divergent Regulatory and Reimbursement Pathways for Digital Therapeutics: A Scoping Review With Implications for Korea
Supplemental Material for Divergent Regulatory and Reimbursement Pathways for Digital Therapeutics: A Scoping Review with Implications for Korea by Mincheol Kim, and Gaeun Kim in INQUIRY: The Journal of Health Care Organization, Provision, and Financing.
Footnotes
Ethical Considerations
This is a literature-based scoping review using only publicly available sources. The study did not involve human or animal participants and therefore did not require institutional review board approval.
Author Contributions
Conceptualization — Gaeun Kim; Methodology — Gaeun Kim and Mihcheol Kim; Formal analysis — Mihcheol Kim; Investigation, including literature screening and data charting — Mihcheol Kim; Writing — original draft — Mihcheol Kim; Writing — review and editing — Gaeun Kim and Mihcheol Kim; Supervision — Gaeun Kim. Gaeun Kim served as the corresponding author. Both authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Research Foundation of Korea (NRF) grant funded by the Korean government (MSIT) (No. 2022R1A2C1012697).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All sources are publicly available. The completed PRISMA-ScR checklist (Supplementary File 1), borderline-decision log (Supplementary File 2), and full search strategy (Supplementary File 3) accompany this submission.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.