
Abstract
Introduction
Pelvic floor disorders (PFDs) are common conditions that negatively affect women’s quality of life, particularly in low-resource settings where awareness is often limited. Although knowledge of PFDs remains low in many developing settings, evidence from Ethiopia is limited, and the extent and determinants of women’s knowledge have not been well explored. Therefore, this study aimed to assess the knowledge of pelvic floor disorders and its determinants among women in Gurage Zone, Central Ethiopia.
Methods
A community-based cross-sectional study design was utilized, employing a multistage sampling technique to select 844 women. Data were collected through face-to-face, interviewer-administered questionnaires. The data were entered into EpiData version 3.1 and exported to SPSS version 26 for analysis. Bivariate and multivariable logistic regression analyses were used to identify factors associated with knowledge of pelvic floor disorders (PFDs). Statistical significance was declared at a p-value of less than 0.05 with a 95% confidence interval (CI).
Results
In this study, the overall prevalence of women’s knowledge of pelvic floor disorders was found to be 40.5% (95% CI: 37.1, 43.7). Higher educational status (AOR = 3.28; 95% CI: 2.02, 7.54), being an urban resident (AOR = 2.51; 95% CI: 1.37, 14.03), being multiparous (AOR = 2.43; 95% CI: 1.08, 5.47), being grand multiparous (AOR = 4.21; 95% CI: 1.81, 11.1), and having awareness of pelvic organ prolapse (POP) as a medical condition (AOR = 2.91; 95% CI: 1.57, 5.40) were identified as determinants of women’s knowledge of pelvic floor disorders.
Conclusion
Only two in five women were knowledgeable about PFD in this study area, which is considered low. These findings underscore the need for targeted educational interventions to bridge knowledge gaps, particularly among populations with lower educational attainment and those living in rural areas.
Introduction
Pelvic floor disorders (PFDs) encompass a broad range of conditions affecting the vagina, lower urinary tract, and bowel, which impair the structure and/or function of the female genital organs. The three most prevalent types of PFDs are urinary incontinence (UI), fecal incontinence (FI), and pelvic organ prolapse (POP).1,2 The International Urogynaecological Association (IUGA) and the International Continence Society (ICS) jointly define urinary incontinence (UI) as the involuntary loss of urine and fecal incontinence (FI) as the involuntary loss of solid or liquid stool. According to the combined IUGA and ICS definition, pelvic organ prolapse (POP) is characterized by a descent of the posterior vaginal wall, anterior vaginal wall, or vaginal apex (or vaginal vault after hysterectomy) due to weakened pelvic floor support or dysfunction.3,4
According to the World Health Organization (WHO), preventing pelvic floor disorders (PFDs) involves primary, secondary, and tertiary measures, targeting onset prevention, early symptom management, and reduction of existing symptoms or relapses.4,5 However, many women lack adequate knowledge about PFDs, pelvic organ prolapse (POP), and fecal incontinence (FI), making it difficult to implement preventive measures.6,7 Even due to a lack of public information on common PFDs, delays healthcare seeking until the dysfunction has progressed, making it more difficult.8-10
Pelvic floor disorders are prevalent gynecological conditions affecting a substantial proportion of women worldwide. Studies show that 1.9% to 46.5% of women globally suffer from PFD.11,12 Anal incontinence (AI) affects approximately 0.2% to 13%,13,14 pelvic organ prolapse (POP) affects about 3%–64.6%, 15 and urinary incontinence (UI) has a prevalence of approximately 1.7% to 35.5%, making them the most common types of PFD. 16
The prevalence of PFDs among women in Ethiopia has been reported to be over 20%.12,17 In the Gurage Zone, 41.1% of women reported PFDs, with the majority experiencing urinary incontinence (32.8%), followed by pelvic organ prolapse (25.5%) and fecal incontinence (4.2%). 18
The development of PFDs is multifactorial and can affect women of any age. 19 Modifiable risk factors include childbirth trauma from improper birthing practices by unskilled attendants, operative vaginal delivery, prolonged second stage of labor, third- and fourth-degree lacerations, and vaginal delivery of large or malpositioned babies. 20 Other contributing factors include poor socioeconomic status, malnutrition, adolescent pregnancy, lack of rest during and immediately after pregnancy, early marriage, multiparity, and lack of puerperal rehabilitation.21,22 This is further complicated by chronic illnesses such as chronic obstructive pulmonary disease, pulmonary tuberculosis, and obesity. 21 Several factors commonly found throughout Ethiopia that can contribute to PFDs include early marriage, grand multiparity, obstructed labor, and a lack of fully developed maternal healthcare infrastructure.13,23,24
Pelvic floor disorders have serious implications for the safety of affected women, as well as for their families, caregivers, and society at large. They cause significant social, economic, physical, and psychological issues, dramatically reducing women’s quality of life and productivity.25,26 PFDs lead to disability and embarrassment, impair social activities, and result in withdrawal from physical activity and sports, social isolation, reduced performance, and loss of personal relationships and intimacy.26,27
PFDs have significant financial implications for both healthcare systems and patients. For example, American women with severe incontinence spend around $7032 annually on routine care, 19 and over $16 billion is spent each year globally on PFDs, mostly (70%) for routine care such as incontinence products.19,28 Healthcare use for PFDs is expected to rise with an aging population,29,30 yet less than half of women with severe symptoms seek care. In the Kersa district, eastern Ethiopia, only 32% of women with PFDs accessed healthcare services. 12 Hence, studies on preventive strategies are crucial to improve individual well-being and reduce economic burden.
The evidence revealed that lack of care-seeking is linked to misconceptions about these conditions. For example, the study found that 81% of women do not consider urinary incontinence (UI) abnormal and believe that PFDs are a normal part of childbirth and aging.31,32 Moreover, other barriers include personal embarrassment, concealment of the condition, which can lead to issues such as domestic violence and lack of awareness that PFDs are a medical disorder, and unawareness of available medical treatments.33,34 The study also indicates that a low level of knowledge about pelvic floor dysfunction is associated with a higher incidence of the conditions. 35 While PFDs are widespread in Ethiopia, there is little or no published data on women’s knowledge of these disorders. 36
Numerous studies have shown that women’s knowledge of pelvic floor disorders can be influenced by factors such as age, occupation, education, lack of awareness of PFDs as a medical condition, parity, no history of care-seeking for PFDs, age at first childbirth, and age at marriage.36,37 Despite this, little is known about women’s knowledge of pelvic floor disorders in Ethiopia, particularly in the study area. Therefore, this study aims to assess knowledge of pelvic floor disorders and its determinants among women in the Gurage Zone, Central Ethiopia.
The objective of this study is to assess knowledge of pelvic floor disorders and its determinants among women in the Gurage Zone, Central Ethiopia, in 2024.
Methods and Materials
Study Setting, Design, and Period
A community-based analytical cross-sectional study was conducted in the Gurage Zone, Central Ethiopia, from March 1 to 30, 2024. The zone borders the Oromia Region to the north and east, Kebena Special Woreda to the northwest, Hadiya and Yem Zones to the southeast, and Silte to the southeast. Administratively, it comprises five towns and ten woredas, each further divided into kebeles. According to the 2007 National Household Census, the zone has an estimated population of 1,280,483, including 657,568 women. 38 The Gurage Zone was selected as the study area based on the study’s objectives and feasibility.
Population
All women in the Gurage Zone constituted the source population. The study population consisted of all women selected from the chosen kebeles.
Eligibility Criteria
Women residing in the Gurage Zone for at least six months and willing to participate were eligible, whereas critically ill women were excluded.
Sample Size Determination
The researcher determined the sample size for this study using a single population proportion formula, considering the following assumptions: a 95% confidence level; the proportion of women with good knowledge about POP and UI, which were 24.1% and 27%, respectively, 36 a 50% population proportion for women’s knowledge of FI, since no prior research exists on this topic in Ethiopia; and a 5% margin of error.
Sample Size Determination for the Women Who had Good Knowledge of POP

Sample Size Determination for the Women Who had Good Knowledge of UI

Sample Size Determination for the Women Who had Good Knowledge of FI

The sample size calculated for n3 was greater than that of n1 and n2. Therefore, n3, which is 422, was used for this study. After applying a design effect of 2, the final sample size was 844. The design effect of 2 was applied based on standard recommendations for community-based studies in similar settings, as a conventional approach to increase the sample size and improve the precision of estimates in the absence of prior intra-cluster correlation estimates for this population.
Sampling Techniques and Procedures
A multistage sampling technique was applied to select a total of 844 women. The Gurage Zone has ten woredas and five administrative towns. Five woredas (Gumer, Ezha, Abeshge, Geta, and Edegagn) and three administrative towns (Gunchure, Wolkite, and Arakit) were randomly selected using a lottery method. From each selected woreda and administrative town, three and two kebeles were chosen at random, respectively. The final sample size was distributed proportionately based on the number of households in each kebele. Eligible women were then recruited from each household using a systematic random sampling technique, with the sampling frame derived from Health Extension Worker (HEW) registration records and kebele administrative records. When multiple women meeting the eligibility criteria were identified in a selected household, one woman was chosen using a lottery method. Two attempts were made to reach selected households if they were closed or if the women were absent during data collection. If both attempts were unsuccessful, the household was recorded as “absent.”
Data Collection Tool and Procedures
Data were collected through face-to-face, interviewer-administered questionnaires conducted at the participants’ homes. Only one woman was interviewed at a time. The data collection tool was adapted from previous studies conducted on a similar outcome of interest.39-43 The Prolapse and Incontinence Knowledge Questionnaire (PIKQ) was used to assess women’s knowledge of PFDs.42-44 The PIKQ was developed in the United States in 2008 as a valid instrument to evaluate patient knowledge about pelvic organ prolapse, urinary and fecal incontinence, and overall knowledge of pelvic floor disorders. Its validity and reliability were found to be satisfactory in studies conducted among gynecologic and urogynaecological patient populations. The tool consists of two 12-item subscales for POP and UI, and an additional 10 items assessing fecal incontinence (FI). Each item has two response options (Agree/Disagree), with one point awarded for each correct response. The total score for each subscale was obtained by summing correct responses. For the PIKQ-POP and FI subscales, a score of ≥50% was considered good knowledge, while for the PIKQ-UI subscale, a score of ≥80% was considered good knowledge. 44
For the overall assessment, a 34-item composite PFD knowledge scale was constructed by combining items from the POP, UI, and FI domains. The total score ranged from 0 to 34. Participants scoring ≥50% were classified as having good overall knowledge of PFDs, while those scoring below 50% were considered to have poor knowledge, based on cutoffs used in previous studies.42,43,45
The questionnaire also included items on women’s socio-demographic characteristics, obstetric variables, awareness of pelvic floor disorders (PFDs), diagnosis-related questions, and questions assessing knowledge of PFDs. To ensure cultural and contextual appropriateness, the questionnaire was forward–backward translated into Amharic and Guragigna by language experts to ensure semantic and conceptual equivalence. The translated versions were reviewed by a panel of experts, including a gynecologist, an epidemiologist, and an assistant professor in maternity and reproductive health nursing, to assess face and content validity. Content validity was ensured using the content validity index and content validity ratio, as evaluated by local experts, to confirm the relevance and essentiality of the items. Based on local expert feedback, minor modifications were made to improve clarity and cultural relevance. A pretest was conducted on a sample of women outside the study area to assess the clarity, understandability, and flow of the questionnaire. Necessary adjustments were made based on the pretest findings. Furthermore, the internal consistency reliability of the final tool was assessed using Cronbach’s alpha, which yielded a value of 0.89, indicating good reliability.
For data collection, eight personnel who were fluent in English and the local languages (Amharic and Guragigna) were recruited. These included eight BSc midwives and two MSc nurses who served as data collectors and supervisors. Two days of training were provided on the overall objectives of the study, questionnaire clarification, sampling strategies, ethical considerations, and procedures for facilitating and supervising the data collection process. This study was reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cross-sectional studies. 46
Variables of the Study
Dependent Variable
Knowledge of pelvic floor disorders (PFDs).
Independent Variables
The variables included age of the respondent, residence, religion, marital status, educational status, occupational status, income, age at marriage, parity, age at first childbirth, awareness of PFDs, and diagnosis of PFDs.
Operational Definitions
Overall Pelvic Floor Disorders (PFDs) Knowledge Score
In this study,
Domain-specific Women’s Knowledge Scores
Data Quality Control
To ensure data quality, language experts translated the questionnaire into Amharic and Guragigna. The tool was ensured to be relevant and understandable to the local context, and the translation was accurate and conceptually equivalent to the original tool. Two days of training were provided for data collectors, including one day of theoretical instruction and one day of practical exercises. The training covered the study objectives, data collection tools and procedures, respondent approach, and confidentiality measures. The principal investigators reviewed all completed questionnaires daily to ensure completeness and consistency. A pretest was conducted on 5% of the sample (42 participants) to evaluate the clarity and appropriateness of the questions. Necessary revisions were made to improve wording, sequencing, and comprehension, and the average time required for data collection was estimated. Each questionnaire was assigned a unique identification code and double-entered into EpiData. All data files were securely stored and accessible only to the principal investigator.
Data Processing and Analysis
After data collection, the questionnaires were coded, checked for completeness, and entered into EpiData before being exported to the Statistical Package for the Social Sciences (SPSS) Version 26 for analysis. Descriptive statistics, including frequencies, percentages, means, and standard deviations, were used to describe the study population with respect to relevant variables. In the present study, the overall PFD knowledge score (≥50% cutoff) was used as the primary dependent variable for the main outcome analysis and regression models. Subscale scores were analyzed separately for descriptive and exploratory purposes only. Bivariate and multivariable logistic regression analyses were conducted to assess the association between independent and dependent variables. Variables with a p-value < 0.25 in the bivariate analysis were included in the multivariable logistic regression model. A p-value < 0.05 was considered statistically significant in the multivariable analysis. The Hosmer–Lemeshow goodness-of-fit test (p = 0.389) was used to assess model fitness. Multicollinearity was examined using the variance inflation factor (VIF) and standard errors to identify potential linear associations among independent variables with no collinearity issues. Finally, the findings were presented in narration, tables, and figures.
Ethical Clearance and Consent to Participate
Ethical clearance was obtained from the Institutional Health Research Ethics Review board of Wolkite University (Ref. No. RCSUILC/19031/16 EC). The study was conducted based on the ethical standards of the Declaration of Helsinki. The ethical letter was given to Gurage Zone town, Woredas, and each kebele to initiate the permission process to collect data. The purpose of the study, participants’ right to refuse, confidentiality, and voluntary participation were explained in detail to the study participants, and informed written consent was obtained. Moreover, consent from participants with no formal education was obtained after the information sheet was read aloud in the local language and documented by thumb impression with a witness. Additionally, written informed consent was obtained from the legally authorized representatives of all participants under the age of 18 years before enrollment. Coding was implemented to remove respondents’ names and other personal identifiers throughout the study to ensure participant confidentiality.
Results
From a total of 844 study participants, 835 study participants were enrolled in the study. The results were presented as follows: 835 study participants were interviewed, and gave a response rate of 98.9% and the results were presented.
Socio-Demographic Characteristics of Participants
Socio-Demographic Characteristics of Women Who Participated in the Study in Gurage Zone, Central Ethiopia, in 2024 (n = 835)
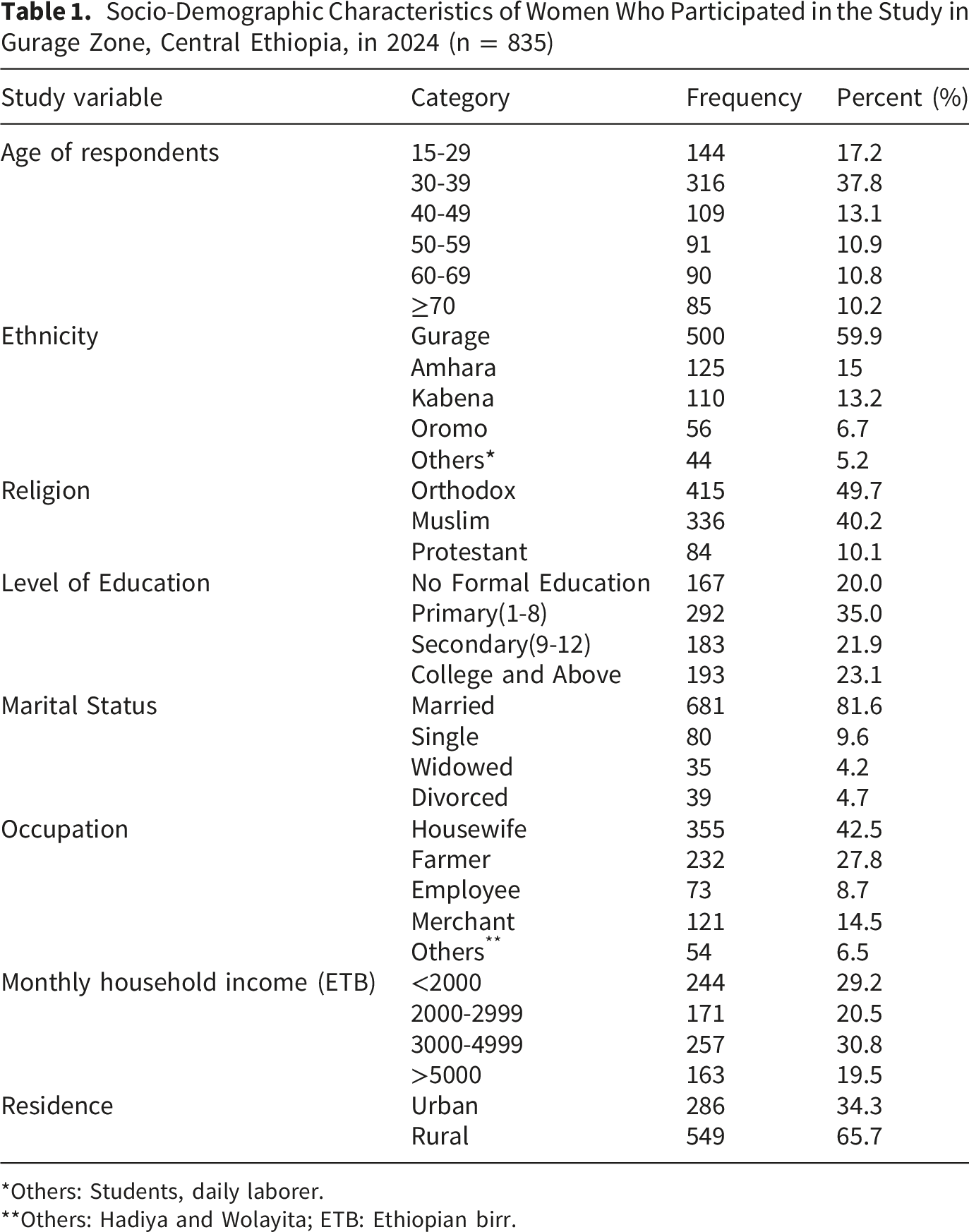
*Others: Students, daily laborer.
**Others: Hadiya and Wolayita; ETB: Ethiopian birr.
Obstetric and Other Characteristics of the Study Participants
Obstetric Characteristics of Women Who Participated in the Study in Gurage Zone, Central Ethiopia, in 2024 (n = 835)

The Prevalence of Knowledge of Pelvic Floor Disorders
In this study, the magnitude of women’s knowledge of pelvic floor disorders (PFDs) among the study participants was found to be 338 (40.5%; 95% CI: 37.1, 43.7) (Figure 1). Magnitude of women’s knowledge of pelvic floor disorders among women in Gurage Zone, Central Ethiopia, 2024 (n = 835)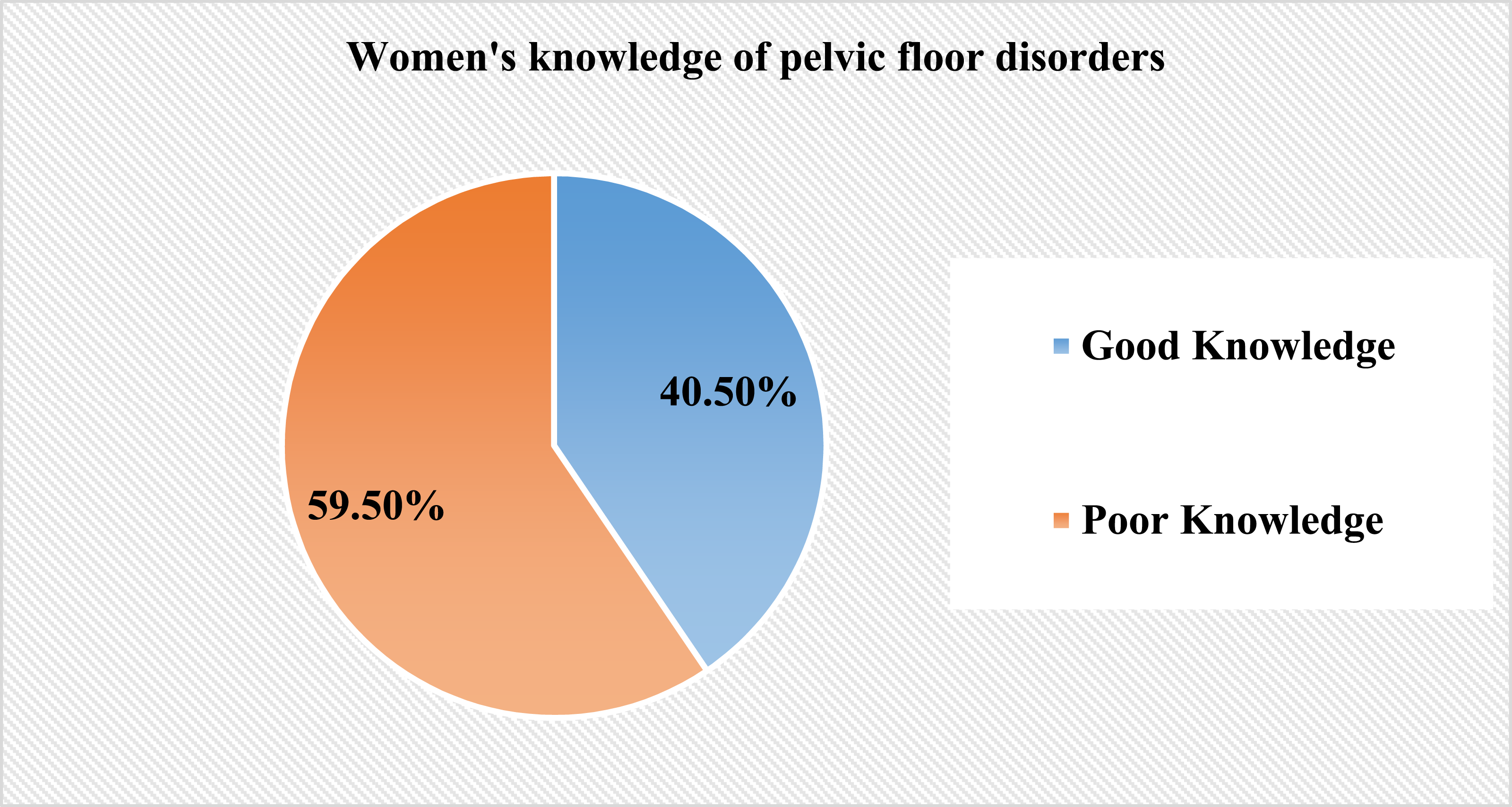
Domain-specific Women’s Knowledge
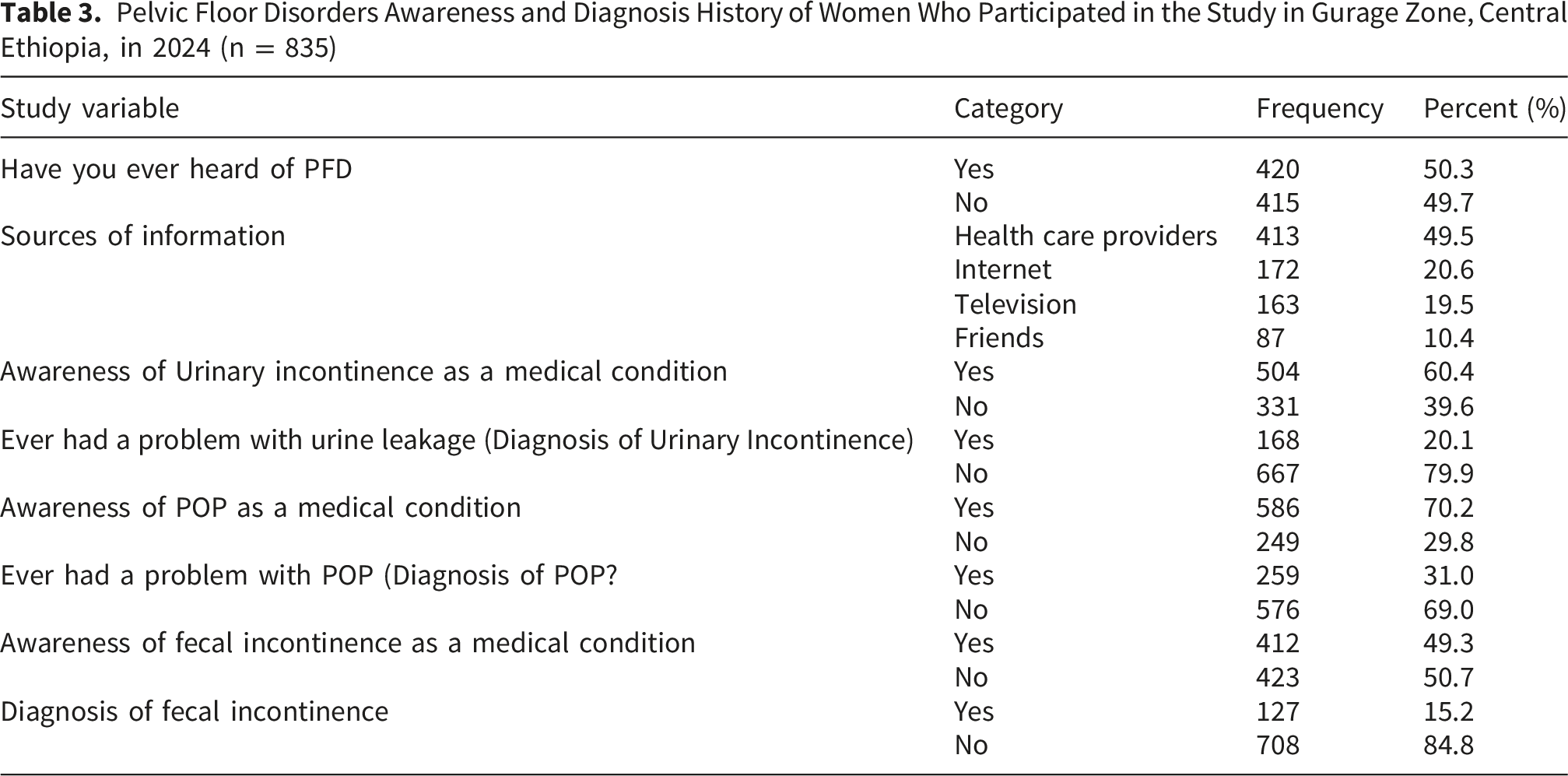
Regarding subscale knowledge analysis, 383 participants (45.9%) demonstrated good knowledge of pelvic organ prolapse (POP), while 176 participants (21.1%) demonstrated good knowledge of urinary incontinence (UI), and 489 participants (58.6%) demonstrated good knowledge of fecal incontinence (FI).
Pelvic Floor Disorders Diagnosis and Awareness
Pelvic Floor Disorders Awareness and Diagnosis History of Women Who Participated in the Study in Gurage Zone, Central Ethiopia, in 2024 (n = 835)
Determinants of Women’s Knowledge of Pelvic Floor Disorders
Bivariate logistic regression analysis was conducted to identify the determinants of the outcome variable. Age of respondents, educational status, miscarriage, residence, parity, PFDs awareness, and diagnosis were selected as candidate variables for multivariate analysis at a p-value less than <0.25. In the multivariable logistic regression analysis, educational status, residence, parity, and PFDs awareness were found to be significantly associated with PFDs knowledge at a p-value of <0.05.
Bivariate and Multivariable Analysis of Determinants of Knowledge of PFDs Among Women Who Participated in the Study in Gurage Zone, Central Ethiopia, in 2024 (n = 835)
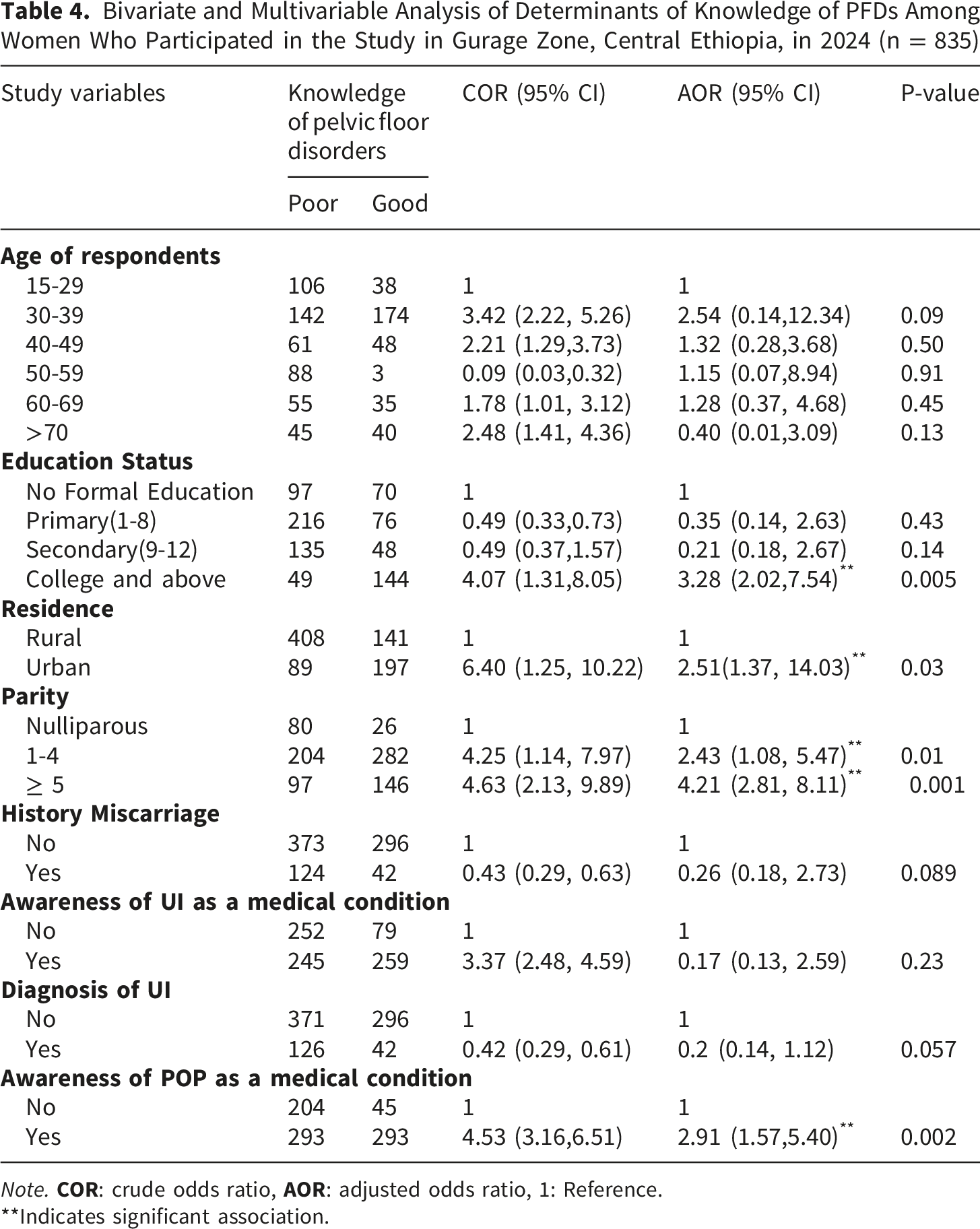
Note.
**Indicates significant association.
Discussions
This is the first study to examine the knowledge of PFDs among Ethiopian women of all ages. The results indicated that 40.5% (95% CI: 37.1, 43.7) of the respondents have good knowledge of pelvic floor disorders (PFDs). This result is lower than that reported in studies conducted in England and Texas, United States, where 45% 47 and 63% 48 of the study participants had good knowledge of pelvic floor disorders, respectively. This finding is lower than reports from England and the United States. This difference may be explained by evidence from Ethiopian studies showing generally low awareness and knowledge of pelvic floor disorders and related preventive measures. Recent studies in Ethiopia reported that only about one-third of women have good knowledge of pelvic floor muscle exercises, and overall awareness of pelvic floor conditions remains low. This may be due to limited access to health information, lower educational status, and inadequate integration of pelvic health education into routine maternal care. Furthermore, pelvic floor disorders are often under-recognized and influenced by sociocultural factors and stigma, which may further limit discussion and awareness.49,50
On the contrary, the results of the present study are higher than those of studies conducted in Connecticut, United States, where only 25.8% 51 of participants showed proficiency in knowledge of pelvic floor disorders (PFDs), and in India, where 15.6% 52 of participants were found to be proficient in PFD knowledge. The possible justification may stem from differences in study settings and participant socio-demographics. For instance, studies conducted in England and the United States focused on pregnant and postpartum women, who may receive antenatal and postnatal education, whereas our study concentrates on the general female population. Furthermore, the observed difference may be explained by recent improvements in maternal health education in Ethiopia, particularly through antenatal care services and community-based health education programs, which may have contributed to increased awareness of pelvic floor disorders compared to earlier studies conducted in other settings. 49
In the subscale analysis of pelvic floor disorder (PFD) knowledge, the lowest proficiency score was observed for urinary incontinence (UI) (21%), followed by pelvic organ prolapse (POP), with 45% of respondents demonstrating proficiency in knowledge of POP. This result is consistent with findings from previous studies conducted in Malaysia 53 and Baltimore, Maryland, United States, and New Haven County, Connecticut, United States.41,54 However, the findings of the present study contradict studies conducted in Singapore, South Asia, 55 Spain, 56 and Northwest Ethiopia, 36 where the majority of participants had adequate knowledge of urinary incontinence (UI). This may be attributed to the normalization of urinary leakage and pelvic organ prolapse, rather than recognition of these conditions as medical disorders. Therefore, raising awareness about the signs, symptoms, treatment, and preventive measures of PFD could enhance knowledge, reduce the risk of developing PFDs, and promote timely healthcare-seeking behavior 51 .
In this study, higher educational status, parity, residence, and awareness of POP as a medical condition were determinants of women’s knowledge of pelvic floor disorders. Women who had attended college or higher education were 3.28 times more likely to be proficient in PFDs knowledge than those with no formal education.
This finding is supported by studies conducted in China, 57 England, 47 New Haven County, Connecticut, United States, 54 Singapore, South Asia, 55 and Malaysia, 53 which indicate that higher education levels are associated with greater proficiency in PFDs. One possible explanation is that women from higher socioeconomic backgrounds tend to have greater health literacy. 58 Furthermore, a recent study conducted in Ethiopia indicated that as educational status increases, the level of knowledge about pelvic floor disorders and preventive measures, such as pelvic floor exercises, also increases. 49
Moreover, the present study found a significant association between residency and knowledge about pelvic floor disorders. Women living in urban areas were 2.51 times more likely to be proficient in PFD knowledge compared to those living in rural areas. This finding aligns with studies conducted in China 57 and Canada, 59 which showed a positive correlation between urban residency and higher levels of PFDs knowledge among participants. This implies that women living in urban areas may have better access to educational resources and healthcare services that can help them better understand pelvic floor disorders. Consequently, they may be able to recognize their symptoms earlier and seek prompt medical attention, thereby improving their health outcomes. Therefore, PFDs-directed educational campaigns in rural settings may bridge the knowledge awareness gap and promote patient empowerment to seek relevant care. Evidence from sub-Saharan African countries suggests that women residing in urban areas tend to have better health-related knowledge, including awareness of pelvic floor disorders, largely due to improved access to education, media, and healthcare services. 22
Women who were aware of pelvic floor disorders (PFDs) were more knowledgeable about PFDs. Those who knew that pelvic organ prolapse (POP) is a medical condition were 2.91 times more likely to possess knowledge about PFDs compared to their counterparts. This finding is supported by studies conducted in Baltimore, Maryland, United States, and New Haven County, Connecticut, United States41,54 and China, 57 which reported that self-reported awareness of POP as a medical condition was the strongest predictor of PFDs knowledge proficiency. Based on this finding, healthcare providers could consider asking women whether they are aware that urinary incontinence (UI), fecal incontinence (FI), and pelvic organ prolapse (POP) are medical conditions with available treatment options, rather than normal parts of aging or childbearing, as part of a basic screening strategy during antenatal care (ANC). If a woman is not aware, healthcare providers can give her a brief explanation of these conditions, provide educational resources, and emphasize that both effective non-surgical and surgical treatments are available. Evidence from Nigeria and Ethiopia indicates that lack of awareness of pelvic floor disorders is strongly associated with poor knowledge and represents a major barrier to both knowledge acquisition and care-seeking.23,60
Knowledge of pelvic floor disorders was significantly associated with parity. Compared to nulliparous women, multiparous women were 2.43 times more likely to be proficient in PFDs knowledge, while grand multiparous women were nearly 4.21 times more likely to have adequate knowledge of pelvic floor disorders.
The findings of this study are supported by research from Singapore, South Asia, 55 and Denmark, 58 which found that multiparous women had better knowledge of PFDs than nulliparous women. Possibly, women may have learned about pelvic floor disorders through antenatal education from a previous pregnancy. Additionally, the previous study conducted in China showed that nulliparous women had a better awareness of PFDs than multiparous women. 57 This result does not match those observed from this study. This could be because increasing parity does not mean increasing knowledge, since knowledge might be hindered by the need for a mother to pay much attention to child-caring. Moreover, early childbearing age may correlate with lower education level and employment opportunities for women. 61 Therefore, these findings reveal significant gaps in women’s knowledge of pelvic floor disorders in the Gurage Zone of Central Ethiopia. Improving awareness could help reduce maternal morbidity related to PFDs. The study also identified key determinants of knowledge and underscores important policy and health system implications, including strengthening provider training, integrating PFD education into maternal health services, and enhancing community, antenatal, and postnatal health education to improve maternal health outcomes.
Strengths and Limitations of the Study
The study employed a community-based cross-sectional design with a large sample size, enhancing the reliability and representativeness of the findings. Potential biases were minimized through clear objectives, pretested questionnaires, training of data collectors and supervisors, random sampling, and statistical adjustments for confounding variables. Ethical guidelines were followed to ensure unbiased participation. However, several limitations should be acknowledged. Although multistage sampling was used, clustering was not accounted for in the analysis, which may have affected standard errors. The wide confidence interval for urban residence suggests limited precision, likely due to category imbalance and small cell sizes, and should be interpreted cautiously. The study may be subject to social desirability bias, recall bias, cultural stigma affecting self-reporting, and interviewer-administered response bias. In addition, since this is a cross-sectional study, it does not show cause-and-effect relationships.
Conclusions
In the present study, only two in five women were knowledgeable about pelvic floor disorders, which is considered low. Higher educational status, urban residence, awareness of POP as a medical condition, and being multiparous were identified as determinants of women’s knowledge of pelvic floor disorders.
These findings encouraged targeted educational interventions to bridge knowledge gaps, particularly among women with lower educational attainment and those living in rural areas. Increasing awareness through community-based programs and healthcare initiatives could significantly empower women with the essential knowledge needed to prevent, recognize, and manage pelvic floor disorders more effectively.
Recommendations
The following recommendations were given based on the findings to the concerned bodies:
Healthcare Providers
It is encouraged to educate women about PFDs during routine visits, especially those with low education and from rural areas, by using simple and local language.
Gurage Zone Health Bureau
It is better to integrate PFD education into existing maternal and reproductive health programs. Furthermore, launch community-based PFD awareness campaigns targeting rural populations. Moreover, train frontline health workers to deliver PFD information effectively, and prioritize resource allocation for underserved areas.
For Researchers
It is encouraged to evaluate the effectiveness of various educational interventions to increase knowledge of PFDs. Further investigate the impact of knowledge on prevention and care-seeking behavior and apply survey-adjusted analytical methods to improve the precision and robustness of estimates.
Supplemental Material
Supplemental Material - Women’s Knowledge of Pelvic Floor Disorders and Its Determinants in the Gurage Zone, Central Ethiopia: A Community-Based Cross-Sectional Study
Supplemental Material for Women’s Knowledge of Pelvic Floor Disorders and Its Determinants in the Gurage Zone, Central Ethiopia: A Community-Based Cross-Sectional Study by Tolesa Gemeda Gudeta, Ayele Sahile Abdo, Aberash Beyene Derribow, Hirut Dinku Jiru, Ayana Benti Terefe, Girma Teferi Mengistu, Seboka Abebe Sori and Mangistu Abera in INQUIRY: The Journal of Health Care Organization, Provision, and Financing.
Footnotes
Acknowledgments
The authors would like to thank Wolkite University for allowing us to conduct the research and for granting ethical approval. Authors also extend our gratitude to the study participants, data collectors, and the supervisor for their unreserved efforts and willingness to participate in this research study.
Author Contributions
T.G.G, S.A.S, A.B.D, H.D.J, A.S.A, A.B.T, and M.A participated in conception and design, acquisition of data, analysis and interpretation of data, and took part in drafting the article. S.A.S, A.B.D, H.D.J, A.S.A, A.B.T, and M.A participated in the sequence alignment and design of the study and performed the statistical analysis. T.G.G., M.A., and S.A.S conceived the study and participated in its design and coordination, and helped with editing the English language. S.A.S, G.T.M, T.G.G, and M.A critically reviewed and revised the manuscript for important intellectual content and participated in the revision. All authors made substantial contributions to the work, critically reviewed the manuscript, approved the final version for publication, and agree to be accountable for all aspects of the work.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Data that support the findings are available from the corresponding author upon a reasonable request.
Supplemental Material
Supplemental material for this article is available online.
Appendix
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.