
Abstract
Introduction
This study aimed to evaluate the severity of symptoms and their impact on quality of life among women experiencing hyperemesis gravidarum (HG) and nausea and vomiting of pregnancy (NVP).
Methods
A cross-sectional study was conducted in hospitals and primary healthcare centers. Data were collected using validated questionnaires that contained the Windsor 2021 criteria for HG diagnosis, PUQE-24 for symptom severity, and NVPQoL for health-related QoL.
Results
Among 380 participants, 167 (43.9%) met the Windsor 2021 criteria for HG. The mean PUQE-24 score was 5.4 ± 2.5, with 112 (29.4%) reporting moderate to severe symptoms. A prior history of HG was strongly associated with current HG diagnosis (OR = 3.47, 95% CI: 1.55-7.80, p = 0.003) and increased PUQE scores by 1.58 points (p < 0.001). PUQE score itself was a significant associated factor, with each one-point increase linked to a 30% higher likelihood of HG diagnosis (OR = 1.30, 95% CI: 1.15-1.48, p < 0.001). Gestational age was inversely related to severity (B = -0.06 per week, SE = 0.01, p < 0.001). Unhealthy or special diets were associated with higher PUQE scores (B = 0.67, SE = 0.30, p = 0.024). Each unit increase in PUQE score was linked to a 6.18-point rise in NVPQoL scores (p < 0.001). A current HG diagnosis was also significantly associated with poorer QoL, contributing to a 17.79-point increase in NVPQoL scores (p < 0.001).
Conclusions
This study provides the first comprehensive application of validated diagnostic and severity tools for NVP and HG in Palestine, highlighting global risk factors such as prior history of HG and gestational age, as well as region-specific determinants including dietary patterns and limited access to evidence-based pharmacological treatments. Findings are informative for clinicians, policymakers, and researchers, underscoring the need for context-sensitive guidelines and inclusive maternal health strategies.
Keywords
Introduction
Nausea and vomiting of pregnancy (NVP) is one of the most common medical conditions in pregnancy, affecting up to 80% of women worldwide, with approximately one-third experiencing moderate to severe symptoms that disrupt daily functioning and psychosocial well-being.1-3 Its severe form, hyperemesis gravidarum (HG), occurs in 0.3-10.8% of pregnancies and is characterized by intractable nausea, persistent vomiting, weight loss, dehydration, and electrolyte imbalance.4-6
Recent systematic reviews and scoping analyses emphasize that HG is associated with hospitalization, nutritional deficiencies, pregnancy termination, and even suicidal ideation, underscoring its devastating physical and psychological toll.6-8 Quality of life (QoL) studies consistently show marked reductions in physical, emotional, and social functioning among affected women, with fatigue, depression, and anxiety being common sequelae. Despite this global burden, data on prevalence, associated maternal factors, and management strategies remain scarce in many low- and middle-income countries, including Palestine.
Previous studies have examined sociodemographic and clinical determinants of NVP and HG, including maternal age, parity, multiple pregnancy, comorbidities, and psychosocial stress, with inconsistent findings across populations.2,5,9,10 Dietary patterns and genetic predisposition have also been implicated, yet few studies have integrated validated symptom severity scales with QoL measures to capture the full burden.2,5,9 Critically, data from low- and middle-income countries, including Palestine, are lacking, leaving unanswered questions about how regional dietary habits, healthcare access, and social support structures shape prevalence and severity.
Validated tools such as the Pregnancy-Unique Quantification of Emesis and Nausea (PUQE-24) scale and the Windsor 2021 criteria have increasingly been applied to standardize the diagnosis and severity classification of HG across diverse populations.1,3,11-13 PUQE-24 has been used in prospective cohorts in different healthcare systems to quantify symptom severity and predict hospitalization risk, demonstrating strong usability and correlation with maternal outcomes.14-16 The Windsor consensus criteria, introduced in 2021, emphasize functional impairment and inability to eat or drink normally, and have been adopted in recent studies to improve diagnostic consistency.17,18 QoL assessments have also been integrated into HG research, with studies showing that women with severe PUQE scores report marked reductions in physical, emotional, and social functioning, including fatigue, depression, and impaired work participation.5,11
Few regional studies have been conducted to assess prevalence, severity, and how cultural dietary patterns, healthcare access, and social support structures influence the burden of NVP and HG. Addressing these gaps is essential to ensure that evidence-based interventions are informed by diverse populations and contexts. Against this background, the present study was designed to comprehensively evaluate the prevalence, severity, and determinants of NVP and HG among Palestinian pregnant women. Specifically, the study aimed to quantify symptom severity, diagnose HG using standardized criteria, identify maternal factors associated with these outcomes, and evaluate their impact on QoL. By situating our findings within both regional and global contexts, this study provides novel evidence to guide clinical care, public health planning, and policy development in Palestine and comparable low-resource settings.
Methods
Study Design and Settings
This study employed a cross-sectional design. Data collection was conducted between October 2025 and January 2026 across major hospitals and primary healthcare centers in the ten West Bank governorates: Nablus, Hebron, Tulkarm, Qalqilya, Jenin, Tubas, Salfit, Bethlehem, Ramallah, and Jericho. Participating hospitals included Al-Ittihad Hospital, Rafidia Surgical Hospital, St. Luke’s Hospital, Al-Hussein Governmental Hospital, Al-Meezan Specialized Hospital, Princess Alia Governmental Hospital, Ahli Hospital, Red Crescent Specialized Hospital, Martyr Dr. Thabet Thabet Government Hospital, Ibn Sina Specialized Hospital, Jenin Government Hospital, and Palestine Medical Complex. Primary healthcare centers included Al-Makhfiyyeh and Balata Camp Health Centers in Nablus, and Al-Salam Primary Healthcare Center in Hebron. These institutions serve diverse geographic and socioeconomic populations, ensuring a representative sample of pregnant women in the West Bank. This study was conducted in adherence to the STROBE (Strengthening the Reporting of Observational Studies in Epidemiology) checklist, with detailed compliance documented in Supplementary Table S1. This alignment with international reporting standards enhances transparency, reproducibility, and methodological rigor.
Study Population and Eligibility Criteria
The study population comprised Palestinian pregnant women aged 18 years or older, residing in the West Bank, who experienced symptoms of NVP or were diagnosed with HG; asymptomatic pregnant women were not eligible for inclusion. Eligible participants were those who had used pharmacological and/or non-pharmacological treatments to manage their symptoms and who provided written informed consent prior to enrollment.
Women were excluded if they had underlying medical conditions unrelated to pregnancy that could independently cause nausea and vomiting (e.g., gastrointestinal disorders, malignancies), if they were asymptomatic and did not report nausea or vomiting during pregnancy, or if they submitted incomplete questionnaires or insufficient data that precluded reliable analysis. This approach ensured that the study sample reflected the true burden of NVP and HG in pregnancy, while minimizing confounding from non-pregnancy-related causes of nausea and vomiting.
Study Size and Sampling
The sample size was calculated using the Raosoft sample size calculator (https://www.raosoft.com), assuming a 95% confidence level, a 5% margin of error, a 50% response distribution, and an estimated population of 30,845 pregnant women based on the Ministry of Health annual report. This yielded a minimum required sample size of 380 participants, which was achieved during the study period.
A non-probability convenience sampling technique was employed. Eligible participants attending antenatal services at the selected hospitals and primary healthcare centers were consecutively invited to participate until the required sample size was reached. This approach ensured feasibility and timely recruitment while capturing a diverse sample representative of pregnant women across different geographic and healthcare settings in the West Bank.
Variables, Measures, and Data Collection
In this study, the primary outcome was the prevalence of HG, defined according to the Windsor 2021 criteria.1,3,18 Diagnosis required the presence of severe nausea and/or vomiting, inability to eat or drink normally, and a strong impact on daily living activities, with symptom onset before 16 weeks of gestation. Contributory features such as dehydration and weight loss were also considered, though not mandatory, thereby ensuring that the definition captured both functional impairment and clinical severity. The diagnosis of HG was established at the time of study enrollment by attending obstetricians using the Windsor 2021 criteria. All participants were assessed in hospital or primary care settings, and diagnoses were confirmed through direct clinical evaluation and review of medical records. This standardized approach ensured consistency across sites and minimized misclassification.
The secondary outcomes focused on the severity of NVP and its impact on maternal QoL. Symptom severity was measured using the Motherisk-modified Pregnancy-Unique Quantification of Emesis (PUQE-24) questionnaire,11,12,14,19,20 which quantifies the burden of NVP over the preceding 24 hours. The PUQE-24 captures three domains: the duration of nausea, the frequency of vomiting, and the number of retching episodes. Each domain is scored from 0 to 5, yielding a total score between 3 and 15. Standard cut-offs were applied to classify severity: mild (4-6), moderate (7-12), and severe (13-15). This tool has been validated internationally and was used in this study to stratify participants according to symptom burden. It is important to note that the Windsor 2021 criteria were used exclusively for the diagnosis of HG, focusing on functional impairment and inability to eat or drink normally, whereas the PUQE-24 scale was applied to measure the severity of NVP symptoms over the preceding 24 hours. This distinction ensured that diagnostic classification and symptom quantification were complementary but non-overlapping.
Maternal health-related QoL was assessed using the NVP-specific QoL (NVPQoL) questionnaire.21-25 This instrument evaluates four domains: physical, functional, emotional, and social, over the previous week. Items are scored on a seven-point Likert scale, with higher scores reflecting worse QoL. The NVPQoL has been validated in multiple populations and provides a multidimensional measure of the impact of NVP and HG on daily functioning and psychosocial well-being.
The main explanatory variables included the type of treatment received for NVP or HG, categorized as pharmacological, non-pharmacological, or combined interventions. Specific medications (e.g., meclizine, pyridoxine, ondansetron) and remedies (e.g., ginger, lemons, herbal preparations) were recorded, along with the frequency of use. Treatment-related side effects, cultural or family influences, and the level of social support were documented. Patient satisfaction with treatment was measured using a five-point Likert scale, providing insight into perceived effectiveness and acceptability. Additional independent variables were collected to describe the study population and explore potential associations with HG, NVP severity, and QoL. For clarity, explanatory variables were grouped into four categories: (1) sociodemographic factors (age, residence, education, employment, household income satisfaction), (2) behavioral factors (smoking status, pack-year), (3) clinical and obstetric factors (gestational age, trimester, parity, multiple pregnancy, body mass index (BMI), prior HG diagnosis, dietary patterns), and (4) medical history and chronic medication use (comorbidities and medications). The final questionnaire is provided in Supplementary Table S3.
All tools used in this study were previously validated instruments. The questionnaire was translated from English into Arabic using a forward-backward translation process to ensure linguistic clarity and conceptual equivalence. Translations were reviewed by bilingual experts, and a pilot study with 20 pregnant women was conducted to assess feasibility, comprehension, and reliability. Internal consistency was evaluated using Cronbach’s alpha (>0.70), confirming the robustness of the tools in the local context. Data collection was performed through structured face-to-face interviews administered by trained research staff who were 3 final year medical students, following standardized protocols to minimize interviewer bias and ensure consistency across sites.
Statistical Analysis
All data were initially entered into Microsoft Excel and subsequently analyzed using the Statistical Package for Social Sciences (IBM SPSS), version 27. Descriptive statistics were used to summarize participant characteristics. Continuous variables were expressed as means with standard deviations (SD), while categorical variables were presented as frequencies (n) and percentages (%). Given the sample size and distribution patterns observed, parametric tests were applied under the assumption of normality.
To explore associations between the primary outcome (HG diagnosis according to Windsor et al., 2021) and secondary outcomes (PUQE severity categories, PUQE scores, and NVPQoL scores), a series of univariate analyses were conducted. Chi-square tests were used to assess associations with categorical variables, while independent-samples t-tests compared continuous variables between groups. Pearson correlation coefficients were applied to examine relationships between continuous variables. Where comparisons involved more than two groups, one-way analysis of variance (ANOVA) was performed, followed by post-hoc tests when appropriate.
To identify independent predictors of PUQE scores and NVPQoL scores, multivariable linear regression analyses were conducted. Variables were entered into the models if they demonstrated statistical significance (p < 0.05). Regression diagnostics included assessment of multicollinearity (variance inflation factor (VIF) < 5 and tolerance > 0.2), normality of residuals (Shapiro-Wilk test and Q-Q plots), homoscedasticity (Breusch-Pagan test), and linearity of relationships. Model fit was evaluated using adjusted R2 values and residual plots. Results were reported as unstandardized coefficients (B), standard errors (SE), and 95% confidence intervals (CI).
For the binary outcome of HG diagnosis, logistic regression analyses were performed to identify independent predictors. Variables were selected using the same criteria as for linear regression. Diagnostics included evaluation of model fit (Hosmer-Lemeshow goodness-of-fit test), discrimination (area under the receiver operating characteristic curve, AUC), and multicollinearity (VIF). Results were reported as odds ratios (OR) with 95% CI. All statistical tests were two-sided, and a p-value < 0.05 was considered statistically significant. Cases with missing or incomplete data were excluded from analyses to maintain data integrity.
Results
Of 467 women approached, 380 met eligibility criteria and were enrolled. The recruitment process is shown in Supplementary Figure S1.
Sociodemographic, Health, Pregnancy-Related, and Lifestyle Characteristics of the Study Participants
Participants had a mean age of 27.4 ± 4.8 years and BMI of 26.9 ± 4.6 kg/m2. Most were university educated (78.6%) and unemployed (77.3%). About one-fifth reported comorbidities, while strong social support was common (61.3%). The mean gestational age was 23.8 weeks, and over one-third were in their first pregnancy. Dietary patterns were largely balanced (82.8%), with only small proportions reporting unhealthy or special diets. Full details are provided in Supplementary Tables S3-S4.
Prevalence and Severity of NVP Symptoms
The mean PUQE-24 score was 5.4 ± 2.5, with nearly one-third of participants (29.4%) experiencing moderate to severe symptoms. Nausea was common, while frequent vomiting or retching episodes were rare. Detailed distributions are presented in Supplementary Table S5.
Associations Between Maternal Variables and PUQE-24 Score and Severity Classification
Maternal Factors Independently Associated With PUQE-24 Scores
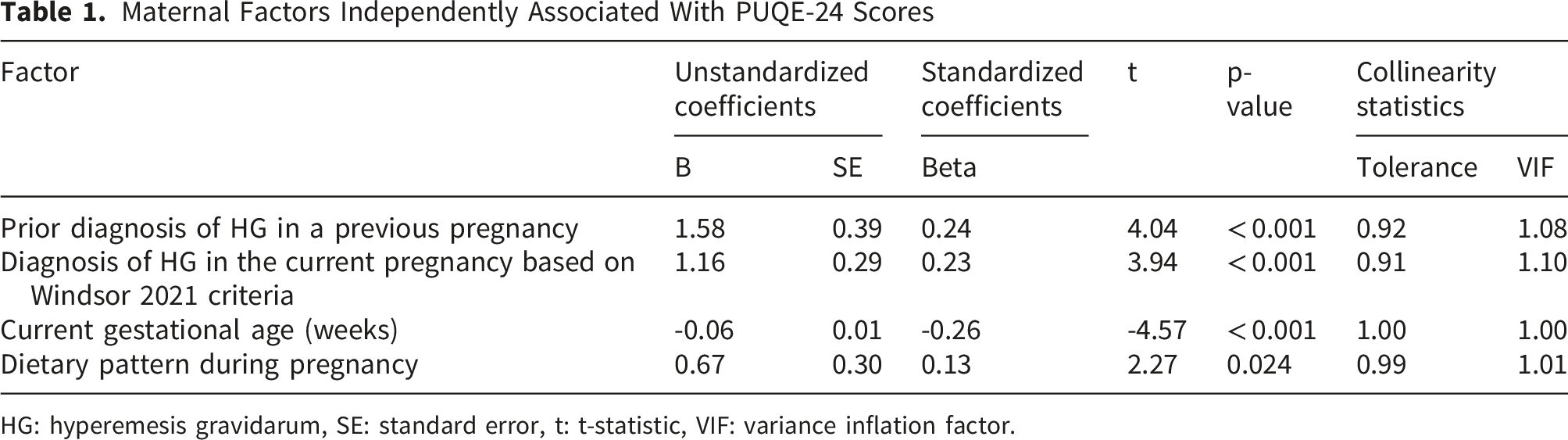
HG: hyperemesis gravidarum, SE: standard error, t: t-statistic, VIF: variance inflation factor.
Prevalence of HG
Using Windsor criteria, 43.9% of participants were diagnosed with HG. Most reported severe NVP or inability to eat and drink, with over half noting a strong impact on daily activities. Early symptom onset and dehydration were common, while complications such as weight loss (11.8%), malnutrition (7.8%), and hospitalization (5.0%) were less frequent. Full distributions are provided in Supplementary Table S7.
Associations Between Maternal Variables and HG
Maternal Factors Independently Associated With Likelihood of Being Diagnosed With HG in the Current Pregnancy Based on Windsor 2021 Criteria
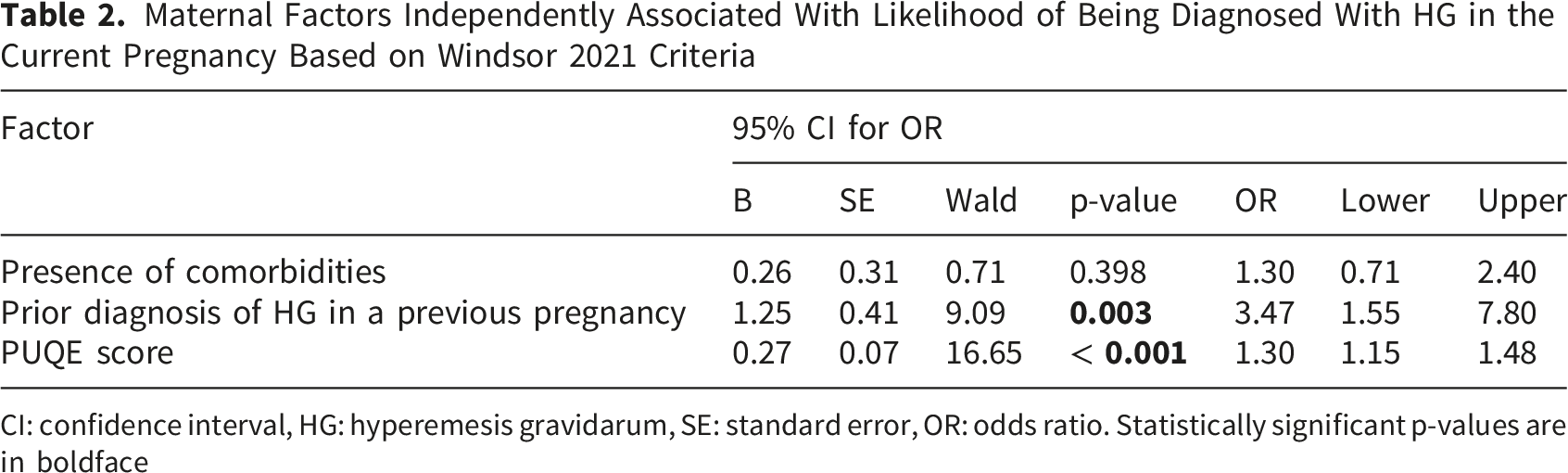
CI: confidence interval, HG: hyperemesis gravidarum, SE: standard error, OR: odds ratio. Statistically significant p-values are in boldface
QoL Scores and Symptom Impact
The mean NVPQoL score was 108.8 ± 33.5, indicating a substantial symptom burden (Supplementary Table S9). Fatigue and emotional distress were the most prominent domains, with high scores for tiredness, lack of energy, and feeling emotional or depressed. Functional limitations were also common, as many women reported reduced social and work activities and reliance on partners for daily tasks. Nausea-specific items showed moderate severity, while reassurance that symptoms were part of normal pregnancy scored relatively high, suggesting some psychological comfort despite the burden. Full item-level distributions are presented in Supplementary Table S9.
Associations Between QoL and Maternal Variables
Maternal Factors Independently Associated With NVPQoL Scores
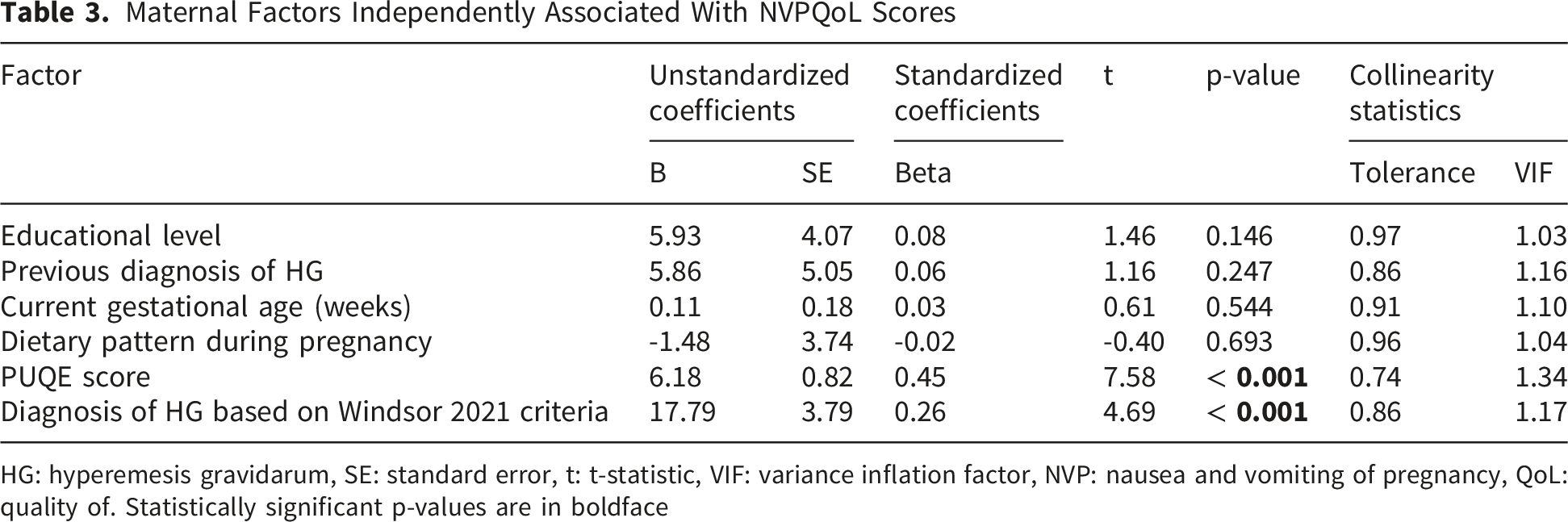
HG: hyperemesis gravidarum, SE: standard error, t: t-statistic, VIF: variance inflation factor, NVP: nausea and vomiting of pregnancy, QoL: quality of. Statistically significant p-values are in boldface
Management Approaches for NVP and HG
Nearly one-quarter of women (22.3%) reported receiving no treatment for NVP or HG. Pharmacological interventions were most common, with about one-third using medications alone and another 17.6% combining them with non-medication approaches. The predominant regimen was meclizine with pyridoxine (40.5%), while ondansetron was less frequently prescribed. Non-pharmacological strategies such as herbal remedies, ginger, and lemons were also reported, though less widely. Most women used interventions once daily, and satisfaction averaged 3.5, reflecting moderate benefit. Side effects were uncommon, with drowsiness and fatigue the most frequent, while persistent nausea and constipation were reported by only a small minority (Supplementary Table S11).
Discussion
HG continues to be recognized as an important complication of early pregnancy, exerting a profound impact on maternal health, psychosocial well-being, and healthcare utilization.16,17,22 While NVP is often dismissed as a benign and self-limiting condition, recent evidence underscores that its severe forms, particularly HG, are associated with nutritional deficiencies, electrolyte imbalance, impaired QoL, and even pregnancy termination in extreme cases.3,5 Against this backdrop, our study contributes novel data from Palestine, a region where systematic evidence remains scarce, thereby filling an important gap in the global literature. The findings are particularly informative for clinicians, who require standardized diagnostic and severity tools to guide management; for public health policymakers, who must allocate resources and design maternal health strategies responsive to local needs; and for researchers, who can build upon this evidence to explore cultural, dietary, and psychosocial determinants of HG in low-resource settings. Moreover, the study offers valuable insights for patients and advocacy groups, by validating the lived experiences of women and highlighting the importance of integrating QoL measures into routine care. In this way, the study not only advances scientific understanding but also provides actionable knowledge for multiple stakeholders committed to improving maternal health outcomes.
Notably, the prevalence of HG in our cohort (43.9%) appears higher than most global estimates.5,6 Several contextual factors may explain this higher prevalence. First, our study applied the Windsor 2021 criteria, which emphasize functional impairment and inability to eat or drink normally, thereby capturing cases that may have been under-recognized in earlier studies using narrower definitions. Second, the reliance on hospital and primary care recruitment may have enriched the sample with women experiencing more severe symptoms, inflating prevalence compared to community-based cohorts. Third, region-specific determinants such as dietary patterns, limited access to evidence-based pharmacological treatments, and psychosocial stressors may contribute to higher symptom burden in Palestine. Taken together, these methodological and contextual considerations suggest that our prevalence estimate reflects both rigorous diagnostic application and unique local realities, rather than a true divergence from global epidemiology.
Our findings align with prior studies but specifically highlight that a prior diagnosis of HG, current HG diagnosis based on Windsor 2021 criteria, gestational age, and dietary patterns were the significant maternal factors associated with symptom severity and QoL deterioration in this cohort.15,20,26-28 However, the demonstration that dietary patterns and social support were associated with symptom severity and QoL underscores the importance of contextual determinants that are often overlooked in Western cohorts. This resonates with emerging evidence from Eastern countries, where cultural dietary practices and psychosocial stressors have been shown to exacerbate NVP severity. 11 Such contrasts emphasize that while biological risk factors may be universal, the lived experience of HG is shaped by sociocultural and healthcare system contexts. Comparative evidence underscores that differences between Eastern and Western populations are not merely generalized but supported by empirical studies. In Western cohorts, the prevalence of HG was typically between 0.3-1.1%, with risk factors including younger maternal age, obesity, and psychosocial stress.4-6 Conversely, Eastern studies have highlighted cultural and dietary influences. 29 For instance, studies in eastern cultures found higher HG incidence among women with specific dietary restrictions and psychosocial stressors, while some cohorts showed HG rates up to four-fold higher than European women. 29 Migration studies also reveal that immigrant women in Canada experienced HG at 4.5 times higher prevalence, linked to cultural isolation and lack of supportive dietary practices. 30 These findings suggest that while biological risk factors are universal, cultural dietary habits, healthcare access, and psychosocial contexts significantly shape the lived experience and prevalence of HG across regions.
The integration of useful tools as PUQE-24 for symptom severity and NVPQoL for QoL, strengthens the methodological rigor of our study and allows direct comparison with international data. International studies have consistently demonstrated that women with severe PUQE scores report marked reductions in physical, emotional, and social functioning, 5 and our findings confirm that these multidimensional burdens are equally pronounced in Palestine. Importantly, the reliance on non-pharmacological remedies such as ginger, lemon, and herbal preparations reflects both cultural preferences and limited access to evidence-based pharmacotherapy, contrasting with cohorts in high-income countries where antiemetics such as ondansetron and pyridoxine are more widely available. 31 This divergence underscores the need for context-sensitive clinical guidelines that balance global evidence with local realities.
Our cohort highlighted important sociodemographic realities. Despite high levels of university education, most women were unemployed, reflecting broader structural challenges in Palestine where female education rates are high but labor market participation remains limited due to economic fragility and conflict-related restrictions.32-34 At the same time, strong social support was reported by the majority, underscoring the role of family and community networks in buffering the psychosocial burden of HG and NVP in low-resource settings.
From a policy perspective, the findings may inform integrating HG into maternal health strategies in Palestine and comparable low-resource settings. Standardized use of Windsor 2021 criteria and PUQE-24 in antenatal care would enable early recognition and consistent management, while ensuring comparability with global research. At the clinical level, expanding access to safe pharmacological treatments, alongside culturally accepted non-pharmacological remedies, would provide women with a broader range of effective options. At the research level, future studies should explore the interplay between dietary habits, psychosocial stress, and HG severity in Middle Eastern populations, and conduct randomized trials to evaluate the effectiveness of locally used remedies.
This study provides the first comprehensive application of Windsor 2021, PUQE-24, and NVPQoL among Palestinian pregnant women, thereby filling a critical gap in the global literature on HG. Unlike most prior investigations from high-income countries, our work uniquely integrates clinical, sociodemographic, behavioral, and cultural determinants within a low-resource Middle Eastern context, highlighting how dietary patterns, healthcare access, and social support structures shape the burden of HG. By situating Palestinian data within international evidence, this study not only confirms the universality of HG’s impact on maternal QoL but also reveals region-specific challenges and coping strategies that have been largely overlooked. The novelty of this research lies in its multidimensional approach, combining standardized diagnostic tools with contextual variables, to generate actionable insights for clinicians, policymakers, and researchers. Ultimately, this study stands out as a pioneering effort to elevate regional evidence to international standards, underscoring the importance of inclusive, context-sensitive research in advancing maternal health worldwide.
Strengths and Limitations
This study has several notable strengths. Foremost is its novel application of international tools (Windsor 2021 criteria, PUQE-24, and NVPQoL) in a Palestinian population, representing the first standardized assessment of HG diagnosis and severity in the region. The multicenter design across hospitals and primary healthcare centers in ten West Bank cities ensured diverse sociodemographic and healthcare contexts. By integrating clinical, sociodemographic, behavioral, and cultural determinants, the study provides a multidimensional perspective beyond biomedical risk factors. The large sample size, calculated using robust methods, enhances reliability of estimates. Rigorous translation and pilot testing of questionnaires ensured linguistic validity, while adherence to the STROBE checklist underscores transparency and reproducibility.
Nonetheless, several limitations should be acknowledged. The use of convenience sampling may introduce selection bias, though multicenter recruitment across diverse settings helped mitigate this. The cross-sectional design limits causal inference, but remains appropriate for estimating prevalence and burden. Reliance on self-reported data may involve recall bias, yet validated instruments (PUQE-24, NVPQoL) enhance reliability. The absence of biochemical markers of dehydration or nutrition may restrict clinical characterization, though Windsor 2021 criteria emphasize functional impairment rather than laboratory confirmation. Finally, findings from the West Bank may not be fully generalizable to other regions, but they provide a novel foundation for future comparative research.
Conclusion
This study represents the first comprehensive investigation of HG and severe NVP in Palestine using international diagnostic criteria, severity scales, and QoL measures. By integrating clinical, sociodemographic, behavioral, and cultural determinants within a multicenter design, it offers a broad perspective that strengthens regional evidence and aligns it with international standards. The findings confirm that HG in Palestine mirrors the global burden in terms of severity and QoL impairment, while also revealing distinct contextual influences, dietary practices, healthcare access, and social support that shape maternal experiences in low-resource settings. This underscores the importance of inclusive research that accounts for diverse populations, ensuring that clinical guidelines and policy interventions are both globally informed and locally relevant. Ultimately, the study provides an important contribution to maternal health research in the Middle East, offering actionable insights for clinicians, policymakers, and researchers committed to improving outcomes for women affected by HG worldwide.
Supplemental Material
Supplemental Material - Symptom Severity and Quality of Life Impact in Hyperemesis Gravidarum and Nausea of Pregnancy: Evidence From a Large Cross-Sectional Study
Supplemental Material for Symptom Severity and Quality of Life Impact in Hyperemesis Gravidarum and Nausea of Pregnancy: Evidence From a Large Cross-Sectional Study by Hadeel Shabana, Adan Abu Harthieh, Sima Abu Gharbyeh, Taysir Alsadder, Mohammad Jaber and Ramzi Shawahna in Inquiry: The Journal of Health Care Organization, Provision, and Financing.
Footnotes
Acknowledgements
An-Najah National University (https://www.najah.edu) and An-Najah National University Hospital (![]() ) are acknowledged for making this study possible. The authors would like to thank the participating hospitals.
) are acknowledged for making this study possible. The authors would like to thank the participating hospitals.
Ethical Considerations
Ethical approval for this study was obtained from the Institutional Review Board of An-Najah National University (Approval #: NNU-IRB: Pharm-01-25-30). Additional permissions were secured from the Palestinian Ministry of Health as well as the participating hospitals and clinics. All procedures were conducted in accordance with local regulatory requirements and international ethical principles, including the Declaration of Helsinki.
Consent to Participate
Written informed consent was obtained from all participants prior to enrollment. Participation was entirely voluntary, with the right to withdraw at any stage without consequence. To safeguard confidentiality and privacy, all data were anonymized using unique study codes and were accessible only to the research team.
Author Contributions
Funding
This study did not receive any specific funding.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
All data analyzed in this study were included in the manuscript and supplementary materials. The datasets used in the analysis or entered into statistical software can be obtained from the corresponding author upon making a reasonable request.
Declaration of Generative AI and AI-Assisted Technologies in the Writing Process
In line with the journal’s policy on transparency, the authors wish to declare that during the preparation of the manuscript, the authors used Grammarly (Superhuman Platform Inc., San Francisco, California), Copilot (Microsoft Inc., Redmond, Washington), and ChatGPT (OpenAI, San Francisco, California) solely to edit the language and improve grammar, spelling, punctuation, readability, and style of the manuscript. After using these tools/services, the authors reviewed and edited the content as needed and take full responsibility for the scientific content, accuracy, and integrity of the manuscript. Artificial intelligence tools/services were not used for generative editorial work, autonomous content creation, data analysis, statistical interpretation, or the generation of scientific content.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.