
Abstract
Introduction
Social frailty is a multidimensional construct encompassing social behaviors, social resources, and the fulfillment of basic social needs, and is increasingly recognized as an important factor influencing cognitive function. This study aimed to evaluate the association between social frailty and incident dementia as well as changes in cognitive function among middle-aged and older adults, providing novel evidence through a longitudinal cohort applying a multidimensional social frailty framework.
Methods
Data were derived from the China Health and Retirement Longitudinal Study (CHARLS). Social frailty was defined across four dimensions: general resources, social behavior, social resources, and basic social needs. Cognitive function was assessed using tests of memory, orientation, and executive function. Cox proportional hazards models were used to analyze the association between social frailty and incident dementia, and linear mixed-effects models were applied to examine the relationships between social frailty and changes in overall and domain-specific cognitive function.
Results
Compared with the socially robust group, the socially frail group showed an increased risk of incident dementia in Model 1 and Model 3 (HR = 2.42, 95% CI: 1.50–3.89, P < 0.001; HR = 1.52, 95% CI: 0.92–2.53, P = 0.102, respectively). Among the dimensions, only the social behavior dimension remained significantly positively associated with dementia risk (HR = 1.38, 95% CI: 1.11–1.73, P = 0.004). Regarding cognitive function changes, social frailty was significantly associated with decline in overall cognitive function (β = −0.12, 95% CI: −0.18 to −0.06, P < 0.001), primarily reflected in memory decline (β = −0.14, 95% CI: −0.21 to −0.08, P < 0.001), whereas no significant associations were observed for orientation or executive function.
Conclusion
Social frailty is associated with a higher risk of incident dementia and faster cognitive decline, highlighting its potential as an early and modifiable risk marker for cognitive aging.
1. Introduction
Frailty is a complex syndrome involving multiple factors and is generally regarded as a preclinical stage characterized by declines in physiological and social reserves, increased vulnerability, and rising needs for long-term care. 1 Its essence lies in a dynamic process in which the resources required for maintaining basic social functioning gradually decrease or are at risk of insufficiency. 2 In this context, social frailty, as an important dimension of frailty, has attracted increasing attention. Epidemiological studies indicate that among individuals aged ≥60 years, the prevalence of social frailty ranges from 18.8% to 47.3%, 3 suggesting a high occurrence and a potential public health burden in aging populations.
Previous studies have shown that social frailty is closely associated with various cognitive impairments, including motoric cognitive risk syndrome 4 and Alzheimer’s disease. 5 Further longitudinal studies have found that individuals with social frailty tend to exhibit a more rapid trajectory of cognitive decline.6-8 However, the magnitude and pathways through which different social factors affect cognitive function vary,9,10 indicating the need for a systematic evaluation of the combined effects of social factors from a multidimensional perspective.
Conceptually, social frailty is a multidimensional construct encompassing several aspects, including social behavior (e.g., participation in social activities or group organizations), social resources (e.g., marital or partnership status), general resources (e.g., economic status), and basic social needs (e.g., level of social support).11,12 Studies have shown that social frailty is not only associated with an increased risk of chronic physical conditions such as cardiovascular and cerebrovascular diseases, 13 but is also closely related to a higher risk of functional disability, deterioration in mental health status, and decline in neuropsychological function. 14 In addition, substantial epidemiological evidence further confirms that social frailty is significantly associated with the occurrence of disability, 15 depressive symptoms, 16 and increased risk of all-cause mortality,17,18 highlighting its importance in the management of health in older adults.
Although existing studies have preliminarily revealed associations between social factors and cognitive function, current evidence still has several limitations. First, most studies focus on a single social dimension,19,20 making it difficult to fully capture the multidimensional structure of an individual’s social environment and its potential synergistic effects, which may lead to underestimation of the overall impact of social factors on cognitive function. Second, some studies adopt cross-sectional designs, limiting the ability to characterize the dynamic changes in cognitive function over time. 21 Third, substantial heterogeneity exists across studies in terms of measurement tools for social factors, study populations, and statistical analysis methods, reducing the comparability and generalizability of findings. Furthermore, although some longitudinal studies suggest that social frailty is associated with cognitive decline and increased risk of dementia, detailed analyses of changes across different cognitive domains remain limited, and its independent role and combined effects in the process of cognitive aging have not been fully elucidated. Meanwhile, previous studies have mostly focused on single countries or specific regions, and differences in study periods and analytical strategies further limit the general applicability of the findings.
Based on the above research background and limitations, the relationships between social frailty, cognitive decline, and dementia remain to be further explored. This study hypothesizes that social frailty is associated with accelerated cognitive decline and an increased risk of dementia. To test this hypothesis, the present study conducted analyses based on longitudinal data, aiming to systematically evaluate the associations between social frailty and overall cognitive function as well as changes in specific cognitive domains among middle-aged and older adults, in order to provide a theoretical basis for the early identification and intervention of cognitive decline. By applying a multidimensional framework of social frailty in a large, nationally representative longitudinal cohort, this study provides new evidence on its association with incident dementia and domain-specific cognitive decline.
2. Methods
2.1. Study Design and Participants
The China Health and Retirement Longitudinal Study (CHARLS) is a nationally representative prospective cohort study organized and implemented, aiming to systematically assess the aging process and related health issues among individuals aged 45 years and older in China. The study employs a multistage, probability-proportional-to-size (PPS) sampling strategy, covering 28 provinces (autonomous regions and municipalities) across China. Household surveys were conducted in 150 rural villages and urban communities. Trained interviewers administered standardized structured questionnaires to systematically collect information on demographic characteristics, socioeconomic status, health behaviors and lifestyles, and a variety of health-related outcomes. The study protocol was approved and all participants provided written informed consent prior to participation. 22 This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines for cohort studies. 23
Baseline data were obtained from Wave 1 (2011), and participants were prospectively tracked through subsequent follow-up waves up to Wave 4 (2018). The inclusion criteria for this study were as follows: (1) participants aged ≥50 years at baseline; (2) availability of data on social frailty and cognitive function indicators; (3) participants without dementia at baseline; and (4) at least one follow-up assessment. After applying these criteria, a total of 6,431 participants were included in the final analysis (Figure 1). Flow chart of the study population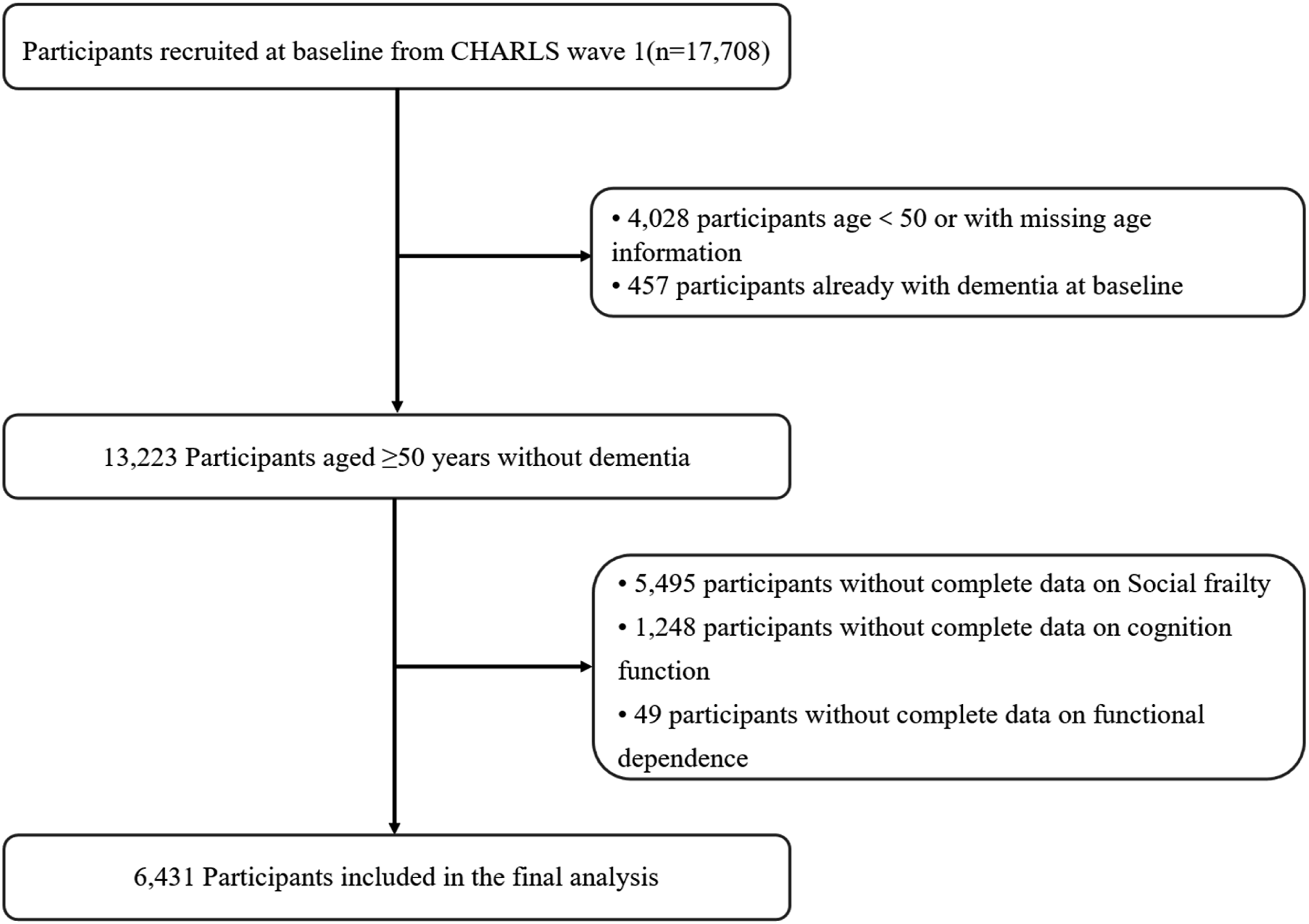
2.2. Social Frailty
Social frailty was assessed at baseline. According to a previous scoping review, social frailty was evaluated across four domains, including general resources, social behaviors, social resources, and basic social needs.
11
This multidimensional framework has been widely used in previous studies to capture the complexity of social vulnerability and has demonstrated its validity in predicting adverse health outcomes among older adults. In addition, similar composite indices of social frailty have been shown to be associated with functional decline, mortality, and cognitive impairment, supporting the use of this approach in population-based studies.17,24 Based on data availability, two variables were used to construct each domain of social frailty in this study. (1) General resources were assessed using educational attainment and total household wealth, both dichotomized. Participants with either educational attainment or total household wealth below the first tertile were classified as having general resource frailty (assigned 1 point); otherwise, they were classified as non-frail (assigned 0 points). (2) Social behaviors were assessed using frequency of social activities and labor force status. Participants who reported no social activities per month or were unemployed were classified as having social behavior frailty (assigned 1 point); otherwise, they were classified as non-frail (assigned 0 points). (3) Social resources were assessed using marital status and the presence of living children. Participants who reported being unmarried or without a partner, or having no living children, were classified as having social resource frailty (assigned 1 point); otherwise, they were classified as non-frail (assigned 0 points). (4) Basic social needs were assessed using information on life satisfaction and frequency of contact with children. Participants with life satisfaction below the mean, or with no weekly contact with their children, were classified as having frailty in basic social needs (assigned 1 point); otherwise, they were classified as non-frail (assigned 0 points). Detailed information on the assessment of social frailty in this study is provided in Supplementary Table 1.
Social frailty was categorized based on the sum of scores across the above domains into three groups, namely socially robust (first tertile, score 0 or 1), social pre-frailty (second tertile, score 2), and social frailty (third tertile, score 3–4). 25 Social pre-frailty represents an intermediate state between social frailty and social robustness, and numerous studies have shown that it is significantly associated with adverse health outcomes.26-28
2.3. Cognitive Assessment and Dementia
Cognitive function was assessed across three domains, including episodic memory, orientation, and executive function.
Episodic memory was measured using immediate and delayed recall of 10 unrelated words. Each correctly recalled word was assigned 1 point, with a total score ranging from 0 to 20; higher scores indicate better memory function. Orientation was assessed using four questions, including year, month, date, and day of the week, with 1 point assigned for each correct answer, yielding a total score ranging from 0 to 4. Executive function was evaluated using the Serial Seven test, with a total score ranging from 0 to 5. The overall cognitive function score was calculated as the sum of the three domain scores, with a total range of 0 to 29; higher scores indicate better cognitive performance. The reliability and validity of these cognitive assessment tools have been validated in previous studies. 29
To improve comparability across individuals and follow-up time points, scores for each cognitive domain and overall cognitive function were standardized based on baseline data. Specifically, individual scores were transformed into z-scores by subtracting the baseline mean and dividing by the corresponding standard deviation (SD). A z-score of 1 indicates that the individual’s cognitive performance is one standard deviation above the baseline mean.
Dementia was defined based on the coexistence of cognitive impairment and functional dependence. 30 Cognitive impairment was defined as a score in any cognitive domain that was more than 1.5 standard deviations below the mean of the population stratified by educational level. Functional dependence was defined as self-reported difficulty in at least one activity of daily living (ADL), including bathing, eating, dressing, transferring (e.g., getting up), or walking within a room.
2.4. Covariates
Participants’ demographic characteristics were collected using structured questionnaires, including age, sex (male/female), marital status (married or partnered/other marital status), educational attainment (below high school, high school, and college or above), 31 and type of residence (rural/urban).
Information on lifestyle and health status was also collected, including current smoking status (yes/no), current alcohol consumption (yes/no), depressive symptoms assessed by the Center for Epidemiologic Studies Depression Scale (CES-D), and physician-diagnosed medical history (including hypertension, diabetes, cardiovascular disease, and stroke).
Anthropometric measurements and biochemical indicators were obtained through standardized physical examinations and blood sample analyses. Anthropometric measures included body mass index (BMI), systolic blood pressure (SBP), and diastolic blood pressure (DBP). Biochemical indicators included C-reactive protein (CRP), glycated hemoglobin (HbA1c), total cholesterol (TC), and high-density lipoprotein cholesterol (HDL-C).
2.5. Statistical Analysis
Continuous variables are presented as means ± standard deviations (SD), while categorical variables are expressed as frequencies and percentages.Group differences were assessed using analysis of variance (ANOVA) or the Kruskal–Wallis test for continuous variables, depending on data distribution, and the chi-square test for categorical variables.
To assess the association between social frailty and the risk of incident dementia, Cox proportional hazards models were used to estimate hazard ratios (HRs) and 95% confidence intervals (CIs), with stepwise adjustment for potential confounders. Three models were constructed: Model 1 was unadjusted; Model 2 was additionally adjusted for age, sex, marital status, educational attainment, and residence; Model 3 was further adjusted for current smoking status, current alcohol consumption, hs-CRP, HbA1c, TC, and HDL-C based on Model 2.
Mixed-effects linear models were used to analyze the association between social frailty status and changes in cognitive function, with β coefficients and their 95% confidence intervals (CIs) estimated. Fixed effects included social frailty, follow-up time (years), and their interaction term; random effects included random intercepts and random slopes to account for individual differences in baseline levels and changes over time.
Subgroup analyses were conducted to evaluate whether the association between social frailty and incident dementia was modified by demographic and clinical characteristics. Stratification variables included age (<60 years, 60–70 years, ≥70 years), sex, educational attainment, residence, current smoking status, current alcohol consumption, and the presence of hypertension, diabetes, cardiovascular disease, and stroke. Interaction effects were assessed by including interaction terms in the models and using likelihood ratio tests.
Sensitivity analyses were performed to assess the robustness of the results. First, participants who developed dementia at the first follow-up were excluded to reduce the impact of reverse causation. Second, missing values in outcome variables were imputed using multiple imputation via chained equations under the assumption of missing at random, with five imputations conducted.
All statistical analyses were performed using Stata version 18.0 and R version 4.4.2. Statistical significance was defined as a two-sided P value <0.05.
3. Results
3.1. Characteristics of the Study Population
Baseline Characteristics of Included Participants According to Social Frailty
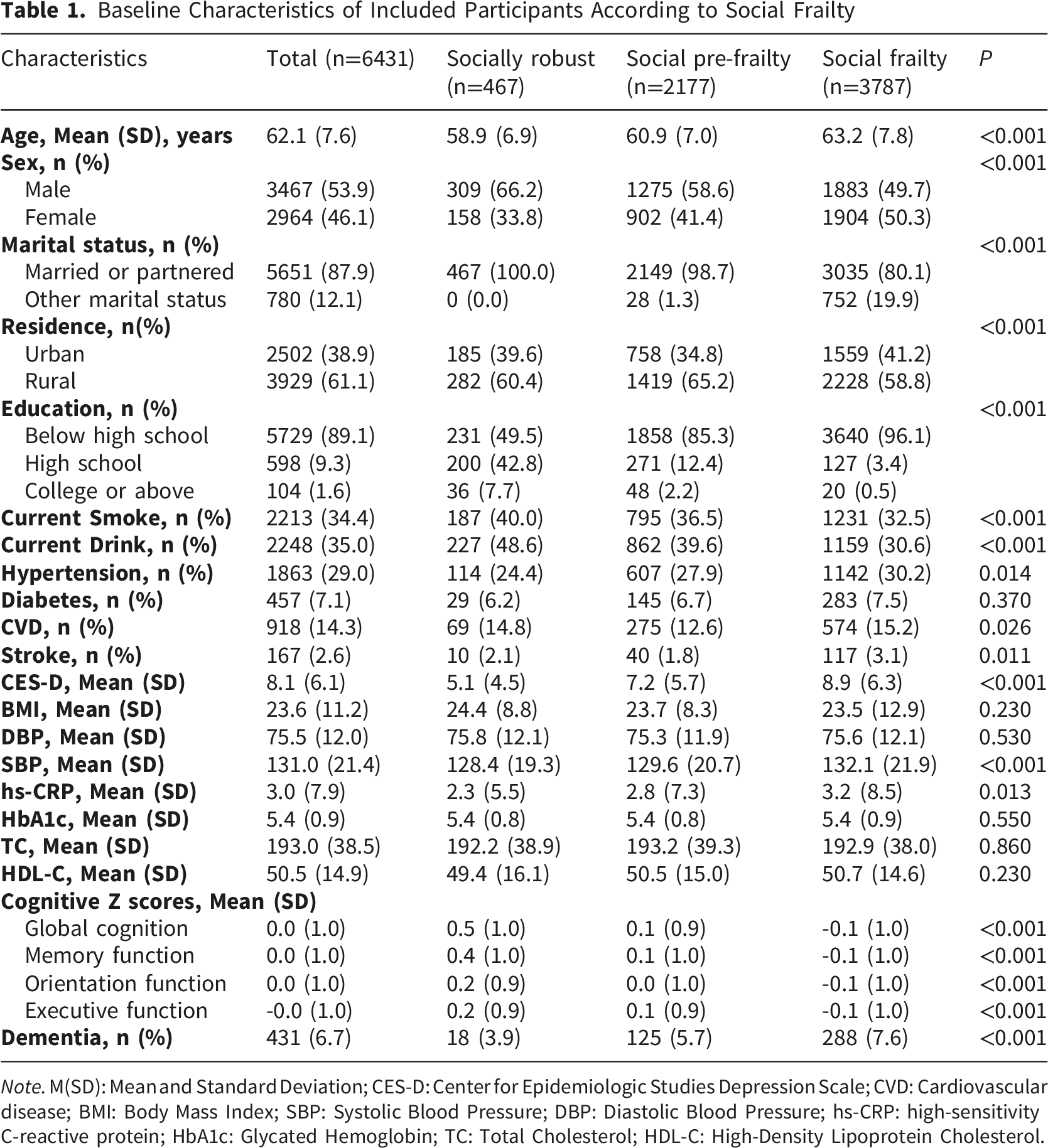
Note. M(SD): Mean and Standard Deviation; CES-D: Center for Epidemiologic Studies Depression Scale; CVD: Cardiovascular disease; BMI: Body Mass Index; SBP: Systolic Blood Pressure; DBP: Diastolic Blood Pressure; hs-CRP: high-sensitivity C-reactive protein; HbA1c: Glycated Hemoglobin; TC: Total Cholesterol; HDL-C: High-Density Lipoprotein Cholesterol.
According to social frailty status, 467 participants (7.3%) were classified as socially robust, 2,177 (33.9%) as social pre-frailty, and 3,787 (58.9%) as social frailty. Compared with the social frailty group, the socially robust group was younger, had a higher proportion of men, and all were married or cohabiting. In addition, the socially robust group had relatively higher educational attainment and a higher proportion of current smokers and alcohol consumers.
Further analyses showed that baseline characteristics stratified by incident dementia status are presented in Supplementary Table 2, and baseline characteristics across different social frailty groups are shown in Supplementary Table 3 – Supplementary Table 6.
3.2. Association Between Social Frailty and Risk of Incident Dementia
Incidence Rates and Hazard Ratios for the Associations Between Social Frailty, Domains of Social Frailty, and Incident Dementia
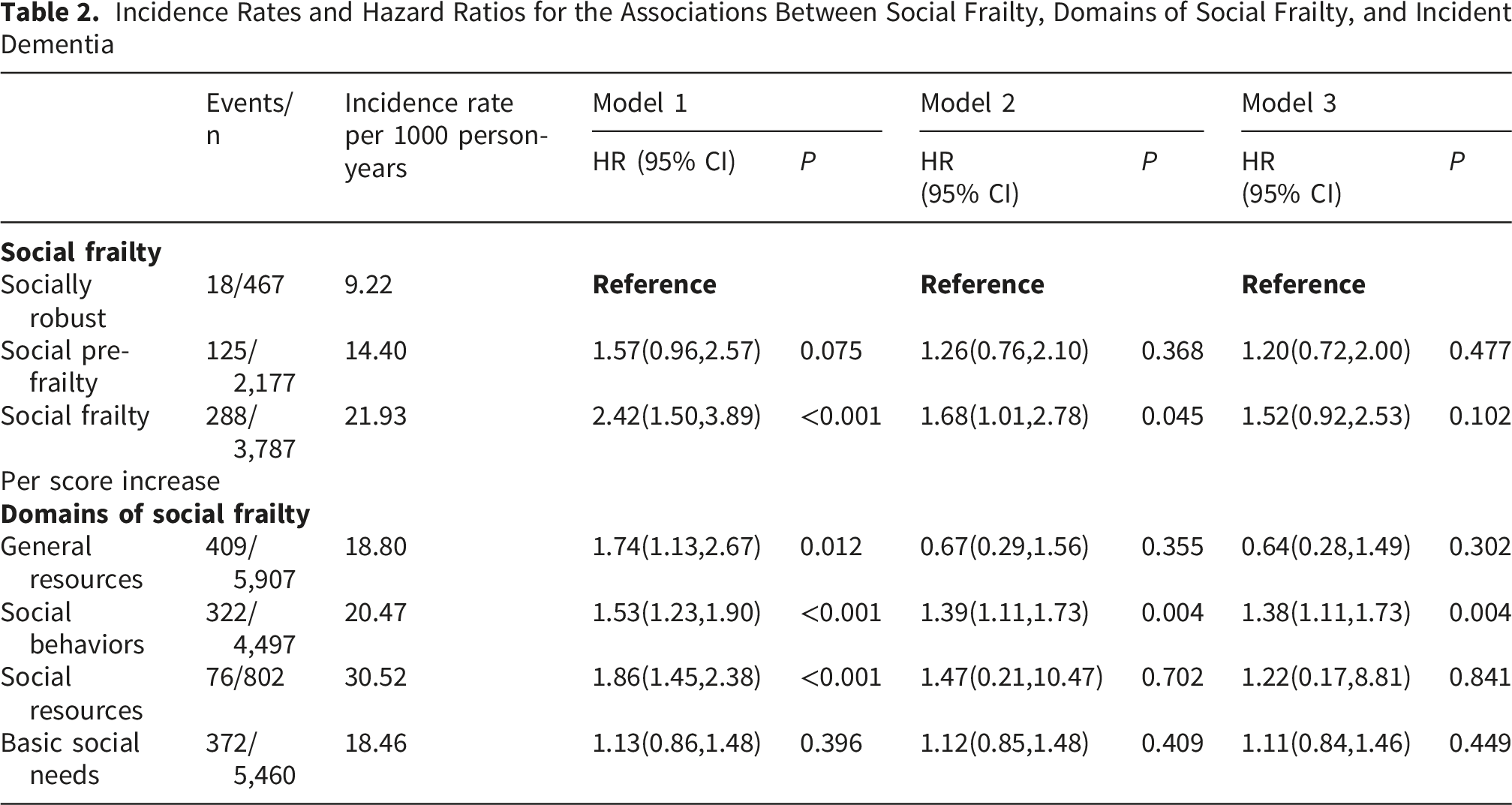
In the Cox proportional hazards model analysis, with the socially robust group as the reference, the unadjusted model (Model 1) showed that social pre-frailty was marginally associated with an increased risk of incident dementia (HR = 1.57, 95% CI: 0.96–2.57), whereas social frailty was significantly associated with a higher risk of incident dementia (HR = 2.42, 95% CI: 1.50–3.89, P < 0.001).
After further adjustment for age, sex, marital status, educational attainment, and residence (Model 2), social frailty remained significantly associated with incident dementia (HR = 1.68, 95% CI: 1.01–2.78, P = 0.045), whereas the association for social pre-frailty was no longer significant (HR = 1.26, 95% CI: 0.76–2.10).
After additional adjustment for lifestyle factors and biological indicators (Model 3), the association between social frailty and incident dementia was attenuated and no longer statistically significant (HR = 1.52, 95% CI: 0.92–2.53), and no significant association was observed for social pre-frailty (HR = 1.20, 95% CI: 0.72–2.00).
In analyses of individual dimensions of social frailty, social behaviors remained significantly positively associated with the risk of incident dementia (Model 3: HR = 1.38, 95% CI: 1.11–1.73, P = 0.004). In contrast, no significant associations were observed for general resources, social resources, or basic social needs in the fully adjusted model.
3.3. Associations of Social Status With Overall Cognitive Function and Specific Cognitive Domains
Mean Differences in the Rate of Changes in Global and Sub-domain Cognition Scores Between Social Frailty
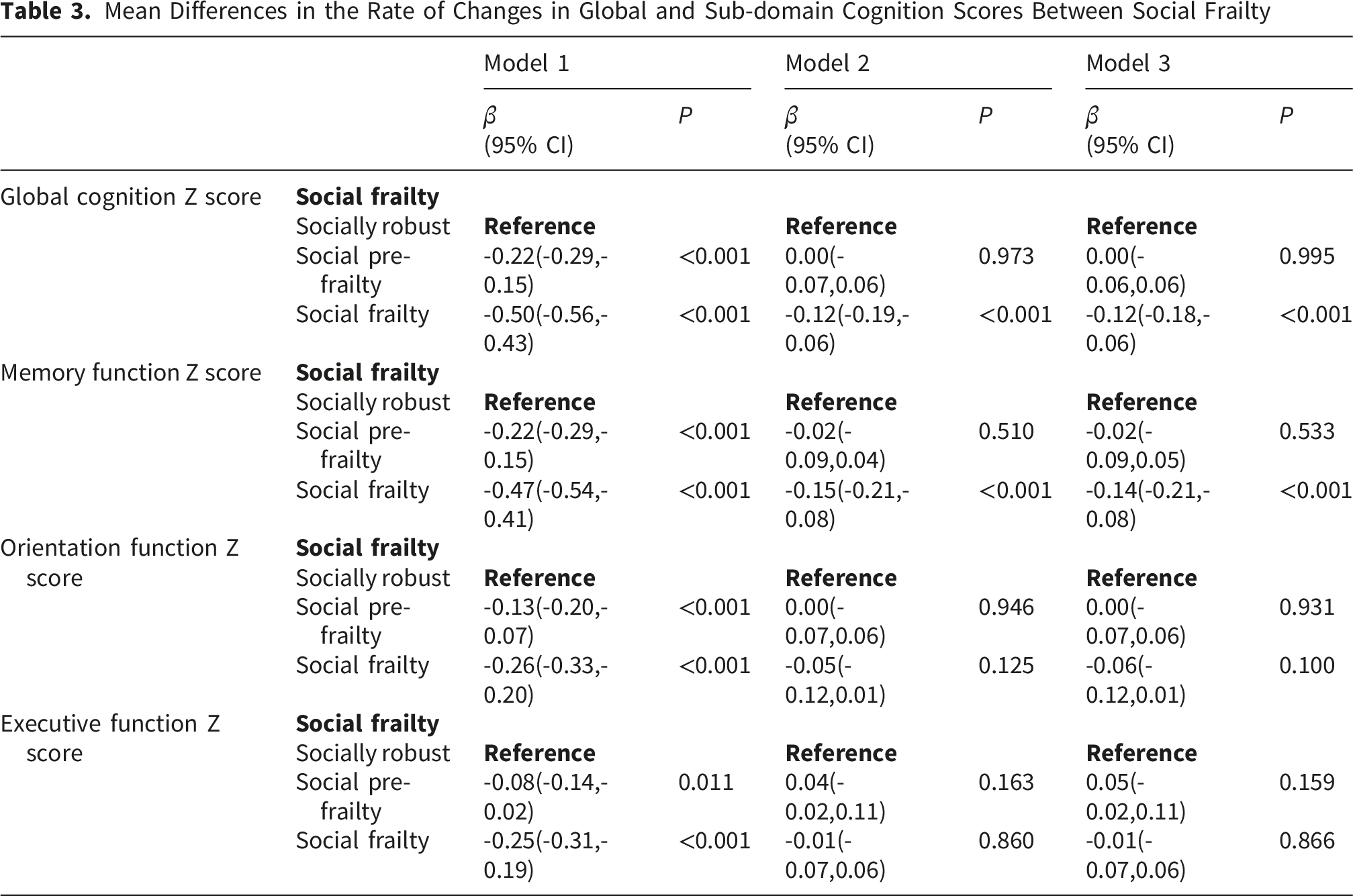
For overall cognitive function, in the fully adjusted model (Model 3), no statistically significant difference in baseline overall cognitive z-scores was observed between the social pre-frailty group and the socially robust group (β = 0.00, 95% CI: −0.06 to 0.06, P = 0.995), whereas the social frailty group had significantly lower overall cognitive function (β = −0.12, 95% CI: −0.18 to −0.06, P < 0.001). In the unadjusted model (Model 1), these associations were more pronounced (social pre-frailty: β = −0.22, 95% CI: −0.29 to −0.15; social frailty: β = −0.50, 95% CI: −0.56 to −0.43; both P < 0.001); however, after stepwise adjustment for covariates, the association for the social pre-frailty group was no longer significant in both Model 2 and Model 3, whereas the negative association for the social frailty group remained stable.
For memory function, after full adjustment (Model 3), no statistically significant difference was observed between the social pre-frailty group and the socially robust group (β = −0.02, 95% CI: −0.09 to 0.05, P = 0.533), whereas the social frailty group had significantly lower memory performance (β = −0.14, 95% CI: −0.21 to −0.08, P < 0.001). Similarly, in the unadjusted model, both groups showed significantly lower memory levels (both P < 0.001), but after adjustment, only the association for the social frailty group remained significant.
For orientation, the fully adjusted model showed no statistically significant differences compared with the socially robust group for either the social pre-frailty group (β = 0.00, 95% CI: −0.07 to 0.06, P = 0.931) or the social frailty group (β = −0.06, 95% CI: −0.12 to 0.01, P = 0.100). However, in the unadjusted model, both groups exhibited significantly lower orientation scores (social pre-frailty: β = −0.13, 95% CI: −0.20 to −0.07, P < 0.001; social frailty: β = −0.26, 95% CI: −0.33 to −0.20, P < 0.001).
For executive function, no significant associations were observed after full adjustment (social pre-frailty: β = 0.05, 95% CI: −0.02 to 0.11, P = 0.159; social frailty: β = −0.01, 95% CI: −0.07 to 0.06, P = 0.866). In the unadjusted model, both the social pre-frailty group (β = −0.08, 95% CI: −0.14 to −0.02, P = 0.011) and the social frailty group (β = −0.25, 95% CI: −0.31 to −0.19, P < 0.001) showed lower executive function, but these associations were no longer present after multivariable adjustment.
3.4. Subgroup and Sensitivity Analyses
Further stratified analyses were conducted to evaluate the consistency of the association between social frailty and outcomes across different populations (Figure 2). Subgroup analyses on the association of social frailty with the risk of dementia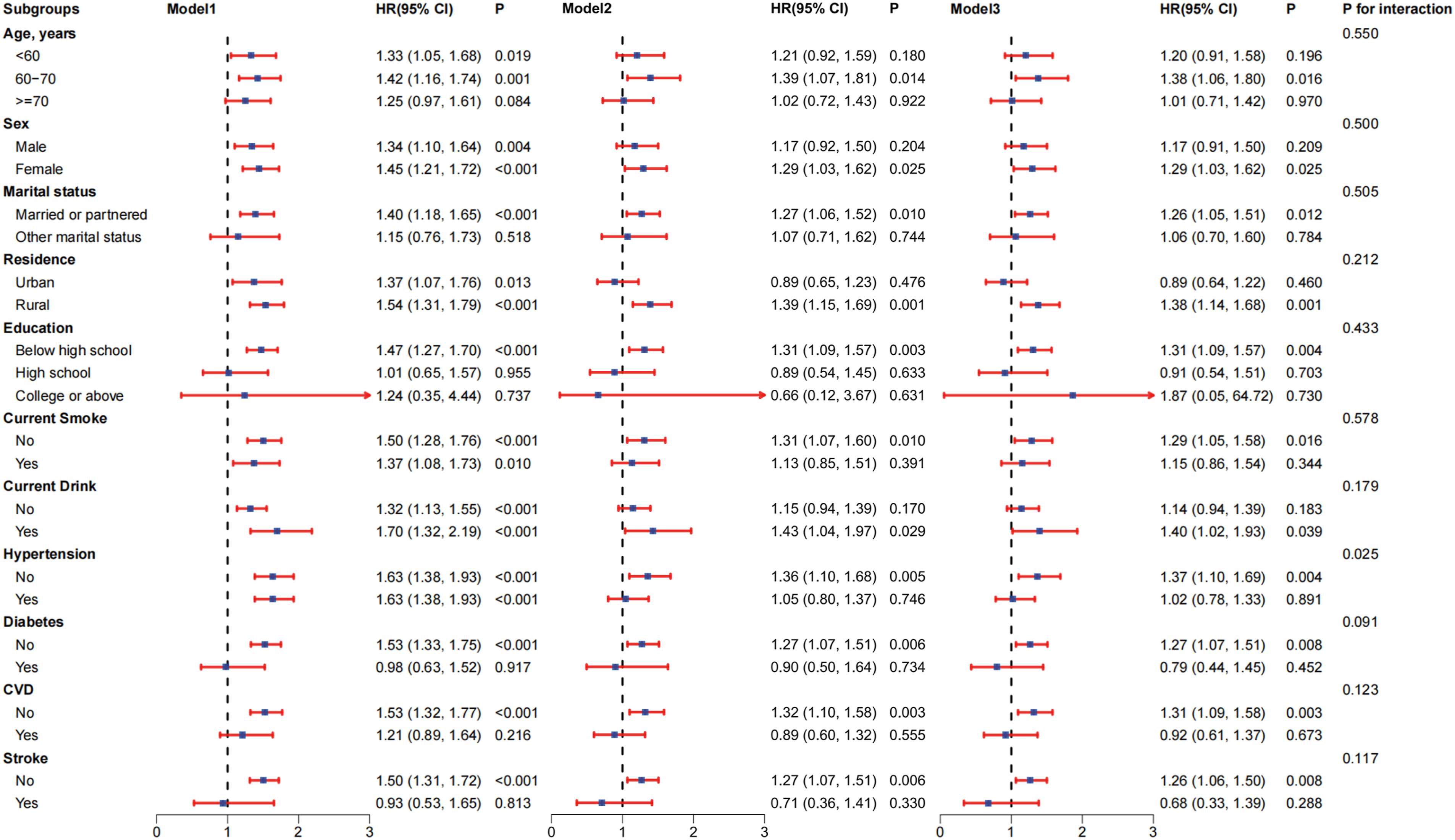
In the fully adjusted model (Model 3), no significant interactions were observed across demographic characteristics. The association was statistically significant among individuals aged 60–70 years (HR = 1.38, 95% CI: 1.06–1.80, P = 0.016).
Regarding lifestyle factors, the association remained significant among non-smokers (HR = 1.29, 95% CI: 1.05–1.58, P = 0.016), whereas no significant association was observed among current smokers. Similarly, a significant association was observed among alcohol consumers (HR = 1.40, 95% CI: 1.02–1.93, P = 0.039), but not among non-drinkers.
A significant interaction was observed for hypertension status (P for interaction = 0.025). Specifically, the association was significant among individuals without hypertension (HR = 1.37, 95% CI: 1.10–1.69, P = 0.004), whereas no significant association was observed among those with hypertension (HR = 1.02, 95% CI: 0.78–1.33, P = 0.891). In contrast, no significant interactions were found for diabetes, cardiovascular disease (CVD), or stroke; however, the association was primarily observed among individuals without these conditions (e.g., without diabetes: HR = 1.27, 95% CI: 1.07–1.51, P = 0.008).
In sensitivity analyses, after excluding participants who developed dementia at the first follow-up wave, the results did not change substantially (Supplementary Table 7 - Supplementary Table 8). In addition, after applying multiple imputation, the results remained consistent with the primary analysis, suggesting that bias due to missing data was minimal (Supplementary Table 9 - Supplementary Table 10). These sensitivity analyses further support the consistency of the main findings and the robustness of the study results.
4. Discussion
In this study, we focused on the impact of social frailty on dementia risk and cognitive decline. By comprehensively assessing four key indicators of social frailty, we found that, compared with individuals without social frailty, individuals with social pre-frailty and social frailty had significantly lower cognitive function at baseline and experienced more accelerated cognitive decline than their healthy counterparts. By applying a multidimensional framework in a longitudinal cohort, our findings provide new evidence on the association between social frailty and both incident dementia and domain-specific cognitive decline. These findings highlight the role of social participation in the process of cognitive aging and suggest that enhancing social support and connections may help slow cognitive decline in this vulnerable population.
Our findings demonstrate that both social pre-frailty and social frailty were associated with lower cognitive function at baseline and an accelerated rate of cognitive decline over time. These findings are generally consistent with previous studies showing that adverse social conditions, including social isolation, limited social participation, and reduced social support, are linked to poorer cognitive outcomes and increased dementia risk.9,32,33 However, unlike prior studies that typically focused on single social factors, our study extends the existing literature by applying a multidimensional framework of social frailty, integrating social behaviors, social resources, general resources, and basic social needs. This comprehensive approach may better capture the complexity of social vulnerability and its cumulative impact on cognitive function. Notably, while some studies have reported inconsistent associations after adjustment for socioeconomic or psychosocial factors, 34 our results remained robust for overall social frailty in adjusted models, suggesting that the combined effect of multiple social deficits may be more important than individual components alone. Furthermore, in contrast to previous findings that highlighted only pre-social frailty as a risk factor, 35 our study demonstrates that both pre-frailty and frailty stages are associated with cognitive outcomes, supporting a graded relationship between social vulnerability and cognitive decline.
Taken together, these findings highlight the importance of assessing social frailty as a multidimensional construct rather than relying on isolated indicators. By using a large-scale, long-term, population-based cohort, our study provides stronger evidence for the longitudinal association between social frailty and cognitive decline. Compared with previous studies with smaller samples or shorter follow-up periods, our results offer improved generalizability and support the use of comprehensive social assessments in identifying individuals at risk of cognitive impairment. Importantly, our findings suggest that early-stage social vulnerability (i.e., social pre-frailty) may already be associated with adverse cognitive outcomes, indicating a potential window for early intervention. This extends previous research by emphasizing not only the presence of social frailty but also its progression as a dynamic risk factor in cognitive aging.
The mechanisms underlying the association between social frailty and cognitive decline are likely multifactorial. One plausible pathway involves chronic inflammation. Previous studies have shown that social isolation and poor social integration are associated with elevated levels of inflammatory markers, such as C-reactive protein (CRP) and interleukin-6 (IL-6).36-38 These inflammatory processes have, in turn, been linked to cognitive decline, dementia risk, and adverse brain health outcomes.39-41 Our findings are consistent with this biological pathway, suggesting that individuals with higher levels of social frailty may experience cumulative physiological stress that accelerates cognitive deterioration. In addition, social frailty may indirectly influence cognitive function through intermediate factors such as depressive symptoms and physical decline. For example, previous studies have demonstrated that social frailty is associated with depression and muscle weakness,16,42, both of which are established risk factors for cognitive impairment.43,44. Taken together, these findings suggest that social frailty may affect cognitive health through both direct biological pathways (e.g., inflammation) and indirect psychosocial and behavioral pathways, highlighting the need for integrated interventions targeting social, psychological, and physical domains.
Building on these mechanisms, our findings further suggest that social frailty may represent a potentially modifiable risk factor for cognitive decline. Interventions aimed at enhancing social participation, strengthening social support networks, and improving access to social and material resources may help mitigate the adverse cognitive effects associated with social vulnerability. In particular, targeting early-stage social vulnerability (i.e., social pre-frailty) may be especially important, as our results indicate that cognitive decline may already be evident at this stage. Therefore, promoting social engagement and strengthening social support systems may serve as practical approaches for preserving cognitive function in middle-aged and older adults.
This study has several notable strengths. First, it employed a population-based prospective cohort study design with a relatively long follow-up period and a large sample size, thereby substantially enhancing the robustness, representativeness, and generalizability of the findings. Second, social frailty was assessed using five concise items, making the approach simple and practical, with good feasibility for large-scale population surveys as well as applicability in clinical practice.
However, this study also has several limitations. First, information on social frailty, dementia, and cognitive function was obtained through self-report, which may be subject to recall bias and reporting bias, thereby introducing a certain degree of misclassification. Nevertheless, previous studies have shown that self-reported information on chronic physical diseases has relatively high validity, 45 which to some extent supports the reliability of the data in this study. Second, social frailty and related covariates were assessed only at baseline, and their dynamic changes during the follow-up period were not captured. In addition, the covariates included in this study were relatively limited, and potential residual confounding may not have been fully controlled, which may have influenced the results. Third, the assessment of social frailty in this study was based on an operational definition derived from available survey items, rather than a standardized or universally accepted measurement. Given that approaches to measuring social frailty vary across studies, this may introduce heterogeneity and requires cautious interpretation of the findings, particularly when comparing results across different populations and study settings. Furthermore, as this was an observational study, its inherent design limitations preclude the establishment of a causal relationship between social frailty and cognitive function. Finally, the study population was derived from China, and the applicability of the findings to populations with different socioeconomic and cultural backgrounds requires further validation.
5. Conclusions
In summary, this study found that social frailty was significantly associated with accelerated cognitive decline among middle-aged and older adults, primarily manifested as continuous reductions in overall cognitive function and memory. At the same time, social frailty showed a trend toward an increased risk of incident dementia. These findings suggest that social frailty may serve as an important risk marker for cognitive deterioration and may play a key role in the progression of cognitive function in middle-aged and older adults. Based on these results, strengthening social support systems and promoting social participation among middle-aged and older adults may have important public health significance and potential intervention value for delaying cognitive decline and reducing the risk of dementia.
Supplemental Material
Supplemental material - Association of Social Frailty With Incident Dementia and Cognitive Decline in Middle-Aged and Older Adults: A Prospective Cohort Study
Supplemental material for Association of Social Frailty With Incident Dementia and Cognitive Decline in Middle-Aged and Older Adults: A Prospective Cohort Study by Qian Chen, Nian Tang in INQUIRY: The Journal of Health Care Organization, Provision, and Financing.
Footnotes
Acknowledgments
We are grateful to the CHARLS study, which provided data for this research. We also thank all the workers, volunteers, and respondents devoted to the CHARLS project.
Ethical Considerations
We utilized de-identifed data from public databases. The ethical approval was covered by the original surveys.
Consent to Participate
Informed consent was obtained from all individual participants by the China Health and Retirement Longitudinal Study (CHARLS) team during the primary data collection. Because this study involved the secondary analysis of a publicly available, fully de-identified dataset, additional informed consent from the participants was not required.
Author Contributions
Qian Chen conceived and designed the study, curated the data, performed the statistical analysis, developed the methodology, and drafted the manuscript. Nian Tang supervised the study and critically revised the manuscript. Both authors read and approved the final manuscript.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
AI Statement
The authors confirm that no artificial intelligence (AI) tools were used in the writing, editing, analysis, or preparation of this manuscript.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.