
Abstract
Comorbid cannabis use is common among individuals seeking treatment for alcohol and substance use disorders, yet research on cannabis craving within polysubstance using samples remains limited and has largely relied on traditional, unidimensional models of craving. The current study sought to provide support for a relatively novel conceptualization of cannabis craving (i.e., Ambivalence Model of Craving) among those receiving treatment for substance use disorders and reporting polysubstance use. Specifically, adults receiving inpatient treatment (N = 140) for substance use disorders completed a cue-reactivity task rating approach and avoidance inclinations after viewing alcohol and drug-related images, including cannabis. Latent profile analysis identified five groups: approach, avoidance, indifference, high ambivalence, and moderate ambivalence. Approach and high ambivalence groups reported greater cannabis use and more substance use related problems, whereas indifference and avoidance groups reported lower use. The approach and high ambivalence groups also endorsed stronger social (i.e., to facilitate social interactions), enhancement (i.e., to increase positive affect), expansion (i.e., to alter perceptual and cognitive experiences), and coping (i.e., to manage negative affect) motives for cannabis relative to the other groups. Overall, findings support the AMC as a multidimensional model of cannabis craving and highlight clinically meaningful subgroups in a polysubstance inpatient sample, though findings should be considered preliminary and replicated in future research.
Introduction
Cannabis is the third most widely used psychoactive substance worldwide (United Nations Office on Drugs and Crime, 2022), and rates of use continue to rise (Caulkins, 2024). In the United States, over 20% of adults now report cannabis use in the past year, and over 6% meet diagnostic criteria for cannabis use disorder (CUD; SAMHSA, 2024). Chronic, heavy cannabis use is a major public health concern given its associations with adverse cognitive, respiratory, and psychological outcomes (National Institute on Drug Abuse, 2020). Notably, cannabis is the most used illicit substance among those with alcohol use disorder (AUD), and the second most used illicit non-primary substance among those with substance use disorders (SUD) (Falk et al., 2008; SAMHSA, 2024). Its use within these populations remains strongly associated with increased alcohol consumption and broader polysubstance involvement (Hasin et al., 2016; Weinberger et al., 2016), and is associated with poorer AUD treatment outcomes, including a lower likelihood of treatment completion (Shikalgar et al., 2026). These patterns highlight the importance of understanding cannabis use not only in the general population but also within clinical samples diagnosed with AUD/SUD. However, the mechanisms that drive problematic cannabis use remain unclear. One mechanism that has received considerable attention is craving.
Cannabis craving, traditionally defined as the strong desire or urge to use cannabis, is a core clinical feature of CUD and is implicated in the initiation, maintenance, and relapse of substance use (Orleans et al., 1991; Tiffany & Wray, 2012). Despite the clinical significance of craving in SUDs, conceptualizing craving as a unitary desire to use has several limitations, including the failure to capture the ambivalence many individuals who use cannabis experience (Stephens et al., 2004). The Ambivalence Model of Craving (AMC) provides a more nuanced and theoretically grounded approach by distinguishing between approach inclinations (desires to use) and avoidance inclinations (desires to avoid using). Indeed, evidence from alcohol use literature has consistently demonstrated that both approach and avoidance inclinations uniquely contribute to use and other alcohol-related outcomes (Gius & Schlauch, 2021; Klein et al., 2007; Schlauch et al., 2013b, 2015, 2019; Stritzke et al., 2007). The purpose of the current study was to provide preliminary evidence for the AMC in the context of cannabis use in a clinical sample of adults receiving inpatient detoxification and treatment services for SUDs.
Cannabis Craving
Cannabis craving is a robust predictor of continued use, reduced quit attempts, and relapse (Enkema et al., 2020; Loflin & Earleywine, 2017; Serre et al., 2018). Although craving for cannabis is often assumed to parallel craving for other substances, this assumption has not been thoroughly validated (Loflin & Earleywine, 2017; Serre et al., 2018). The majority of empirical work has examined cannabis craving through cue-reactivity paradigms, in which exposure to cannabis-related stimuli elicits craving responses. Such cues activate reward-related neural pathways and increase attentional bias, demand, and physiological responses, particularly among individuals with higher levels of cannabis use (Asmaro, 2017; Cousijn et al., 2011; Metrik et al., 2016). Cue-reactivity not only predicts subsequent cannabis use (Filbey & DeWitt, 2012; Norberg et al., 2016), but may also be heightened during withdrawal, similar to patterns observed for alcohol and tobacco (Budney et al., 2008; Norberg et al., 2016). Self-report measures are also commonly used to assess craving. For example, the Marijuana Craving Questionnaire captures subjective dimensions of compulsivity, emotionality, expectancy, and purposefulness (Heishman et al., 2009). Studies utilizing self-report have found that craving decreases across treatment for CUD and is positively associated with cannabis use (Enkema et al., 2020; Phillips et al., 2015; Roten et al., 2013).
Despite these findings, some studies have failed to find associations between craving and subsequent cannabis use or risk of relapse (e.g., Arendt et al., 2007), similar to findings on other substances (e.g., tobacco) that reflect broader inconsistencies in craving as a predictor of substance use (Wray et al., 2013). One potential explanation for these mixed findings is that previous studies have narrowly conceptualized craving, emphasizing the urge or approach motivation to use. Much less attention has been devoted to the simultaneous desire to avoid use, even though clinical experience and theory suggest that individuals can experience both impulses simultaneously (i.e., motivational ambivalence; Breiner et al., 1999; Cousijn et al., 2011; McEvoy et al., 2004).
The Ambivalence Model of Craving
The Ambivalence Model of Craving (AMC; Breiner et al., 1999) directly addresses this gap by conceptualizing drug craving as the dynamic interplay between competing approach (desires to use) and avoidance (desires not to use) inclinations. Approach inclinations are thought to emerge gradually through repeated drug exposure, shaped by neurological adaptations and learning processes involving positive and negative reinforcement (Breiner et al., 1999; Koob & Volkow, 2010; Robinson & Berridge, 1993). In parallel, avoidance inclinations are believed to develop as individuals accumulate negative consequences associated with substance use (Breiner et al., 1999). According to the AMC, craving is best conceptualized as the evaluative space between approach and avoidance inclinations resulting in four distinct motivational states: approach (high approach, low avoidance), avoidance (low approach, high avoidance), ambivalence (high approach, high avoidance), and indifference (low approach, low avoidance) (Breiner et al., 1999; Skinner & Aubin, 2010).
Measuring approach and avoidance inclinations as distinct dimensions provides important clinical and methodological advantages (Stritzke et al., 2007). Conceptualizing craving solely in terms of approach, without accounting for a concurrent avoidance inclination, risks misrepresenting a motivational state that often reflects the interplay of both processes and thereby reduces the clinical utility of craving assessments (Breiner et al., 1999). Empirical work from the alcohol literature has supported this distinction: studies in both clinical and non-clinical samples demonstrate that avoidance inclinations show incremental validity in predicting alcohol-related outcomes, including drinking behaviors, efforts to initiate change, and relapse (Klein et al., 2007; Schlauch et al., 2013b, 2015, 2019; Stritzke et al., 2007).
These motivational states also correspond to distinct clinical profiles. Studies on alcohol use have found that avoidance-oriented individuals reported less drinking, fewer alcohol-related problems, greater readiness to change, and higher treatment engagement (Gius & Schlauch, 2021; Schlauch et al., 2012, 2015). The indifference profile also corresponds to reduced use and fewer problems, as well as greater behavioral control. Approach-oriented individuals, by contrast, report greater alcohol use and related consequences. Notably, the ambivalence profile, which represents individuals with both high approach and avoidance inclinations, also corresponds with heavier use, more alcohol-related problems, and greater conflict in decision-making (Gius & Schlauch, 2021; Schlauch et al., 2012, 2015). Together, these findings underscore the importance of assessing approach and avoidance inclinations simultaneously rather than focusing exclusively on approach.
Extending the AMC to cannabis use represents a critical next step. With rates of cannabis use increasing and substantial comorbidity across SUDs, extending the AMC to cannabis craving may improve our understanding of under what conditions craving is associated with clinical outcomes, including treatment engagement and relapse risk, and improve long-term recovery outcomes. This may be particularly important given the mixed findings in the cannabis craving literature (Arendt et al., 2007), as well as the high dropout and relapse rates in CUD treatment (Stephens et al., 2020).
Present Study
The present study examined the validity of the AMC in the context of cannabis use in an adult clinical sample reporting polysubstance use and receiving inpatient treatment for SUD. Through latent profile analysis, we hypothesized that a four-class solution consistent with the AMC theory would emerge reflecting approach (high approach, low avoidance), avoidance (low approach, high avoidance), ambivalent (high approach, high avoidance), and indifferent (low approach, low avoidance) profiles. A secondary aim was to evaluate whether these profiles differed in cannabis use, drug-related negative consequences, and motives for cannabis use. We hypothesized that the approach and ambivalence profiles would report greater cannabis use and negative consequences than the avoidance and indifferent profiles, as well as stronger motives for cannabis use.
Methods
Participants
The current study is a secondary data analysis of data collected by Schlauch et al. (2015) of a sample of adults (N = 175) receiving inpatient substance use treatment and detoxification services for SUDs. The original data was collected from 2009–2010 to examine the psychometric properties of the Substance Risk Profile Scale, including its associations with alcohol and substance use craving (i.e., cue-reactivity; see Schlauch et al., 2015 for details).
Eligibility criteria included: a) a SUD diagnosis, b) be considered non-violent and treatment-compliant, c) having used drugs or alcohol at a frequency consistent with severe drug or alcohol dependence, and d) be at risk for withdrawal following cessation of use and have withdrawal symptoms that necessitate 24-h medical services for management. The inclusion and exclusion criteria for the study mirrored that of the admission criteria for the detoxification facility. The study staff did not conduct specific screenings to assess for inclusion and exclusion criteria. The current study did not extract data from clinical charts or assess for specific mental health diagnoses. However, we captured self-report measures related to anxiety and depression.
Due to the interest in examining cannabis craving within this polysubstance using sample, analyses were conducted on a final sample size of 140 individuals who reported lifetime cannabis use. Approximately 60.3% of participants were receiving services voluntarily, with an average of 2.3 days (SD = 1.36) in treatment at the time of participation. The average age was 41.1 years old (SD = 11.0). The sample was primarily male (67.1%), White (56.7%), and low-income (48.9% reported annual income < $20,000). See Table 1 for summary.
Summary of Participant Demographics by Cannabis Use History.
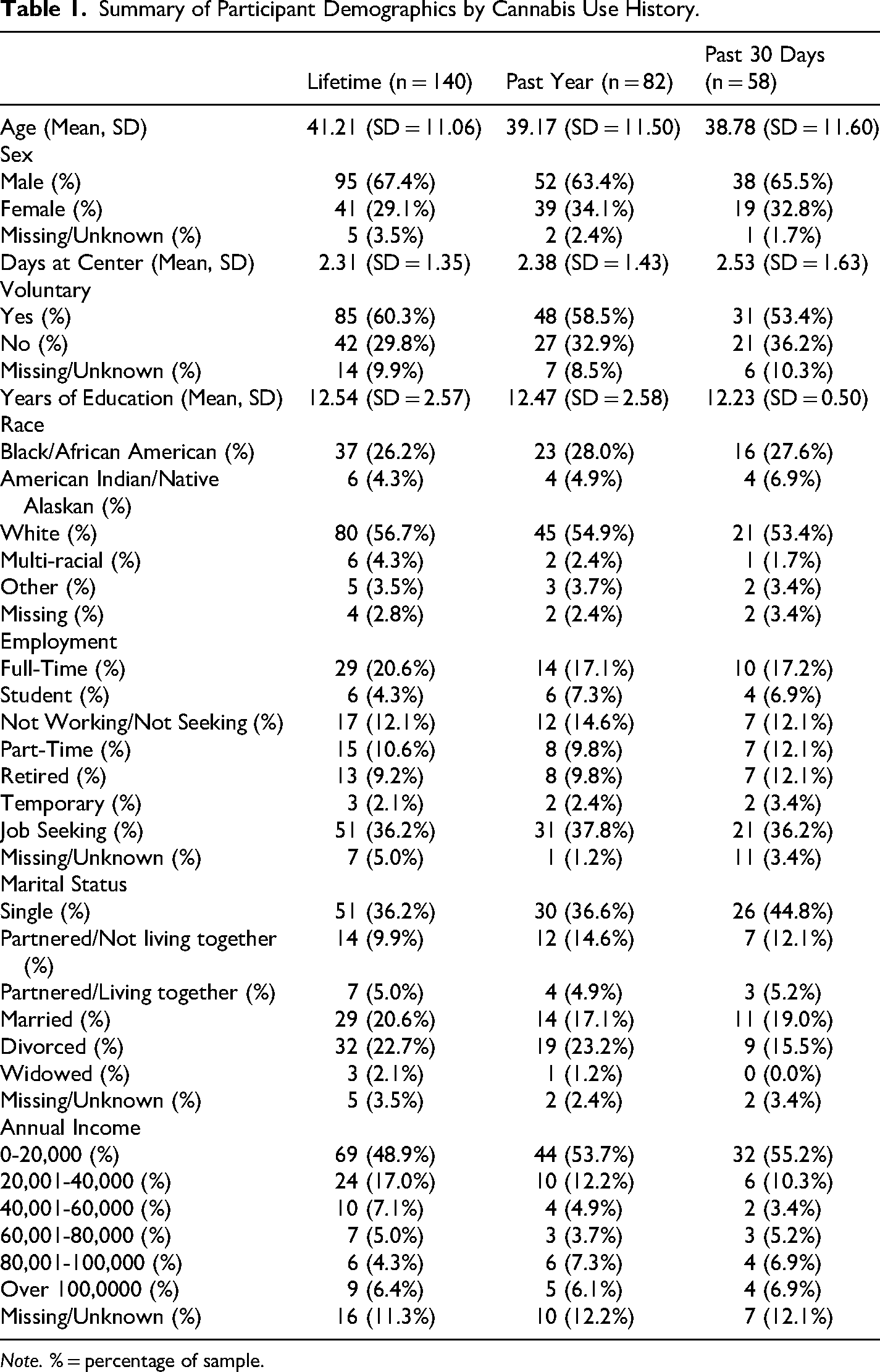
Note. % = percentage of sample.
Procedures
All procedures were approved by an institutional review board, and written informed consent was obtained from all participants. Participants were recruited from an inpatient detoxification unit. This was an observational study that was conducted in a single session with no randomization. The image-rating task lasted approximately 60 min. The image rating task was conducted in this order for each rating: preparatory slide (4 s), substance cue slide (6 s), and a rating period (30 s). Participants received a five-minute break between image sets (three sets of 23 images). Participants then completed a battery of self-report questionnaires which took approximately 60–120 min. Following their participation, participates were debriefed and provided with a psychoeducational group session to discuss craving and triggers to use. Participants received no monetary compensation for their participation. Each image rating session could accommodate up to 12 participants (max number of beds); however, most sessions involved fewer than four participants. This was due to low census, prior participation, or lack of participant interest.
Materials
Image Rating Task
Participants were presented with 69 slides projected onto a white projection screen depicting alcoholic beverages (n = 15), cigarettes (n = 6), food (n = 6), non-alcoholic beverages (n = 6), cannabis (n = 6), stimulant drugs (n = 12), prescription medication (n = 12), and heroin (n = 6) images from the validated Normative Appetitive Picture System (NAPS; Stritzke et al., 2004), previously shown to measure approach and avoidance inclinations (Curtin et al., 2005; Schlauch et al., 2012; Stritzke et al., 2004). Cues varied by setting (e.g., bar, home, neutral) and activity state (e.g., substance untouched, held, or consumed). Brand names and symbols were excluded, and people were generally omitted. Images were presented in six counterbalanced orders with quasi-random distribution.
Measures
Substance Cue Reactivity Ratings
For each cue (image), ratings of “Approach” and “Avoidance” were assessed via self-report. The rating question for approach was: “How much do you want to consume the item right now?”, and the rating question for avoidance was: “How much do you want to avoid consuming the item right now?” Participants responded using a 9-point Likert scale, ranging from 0 “not at all” to 8 “very much.” Participants were instructed to consider the two questions as independent and to rate the images quickly in terms of their “initial reactions.” Ratings for each cue were collected on a separate page, and the order of the rating scales was randomly presented. Similar procedures have been successfully used to collect approach and avoidance inclinations in both non-clinical and clinical populations (Curtin et al., 2005; Schlauch et al., 2012; Stritzke et al., 2004). Internal consistencies for the cannabis approach and avoidance ratings were .94 and .90, respectively.
Demographic Information
Demographic characteristics were collected via self-report survey. Information was gathered regarding participants’ age, gender, height, weight, place of birth, race, ethnicity, marital status, political affiliation, religious affiliation, and annual income. Treatment-specific information was also collected, including treatment-seeking status (i.e., “Are you actively trying to reduce or quit your use of alcohol or drugs?”), length of time spent at the facility, and voluntary admission status (i.e., “Did you check yourself in voluntarily?”).
Substance Use History & Substance use Frequency
The Survey of Alcohol and Drug Use (SADU; Johnston et al., 2010) was used to assess the type and frequency of drug use. The SADU contains questions regarding history and frequency of use across a broad range of drugs. The SADU captures substance use, and frequency history for amphetamines, barbiturates, cannabis, cocaine, crack-cocaine, heroin, inhalants, narcotics, tranquilizers, psychedelics, lysergic acid diethylamide (LSD), alcohol, and cigarettes. Participants report on the number of occasions for which they used a variety of substances in their lifetime, during the past 12 months, and during the past 30 days. The response options for the intervals were: 0 (0 occasions), 1 (1–2 occasions), 2 (3–5 occasions), 3 (6–9 occasions), 4 (10–19 occasions), 5 (20–39 occasions), or 6 (40 + occasions). The SADU is based on items from the Monitoring the Future Survey (National Institutes on Drug Abuse [NIDA]) that has been administered annually since 1975 and has been found to be a reliable and valid measure of substance use (Miech et al., 2026).
Substance Use Related Consequences
The Drug Abuse Screening Test (DAST-28; Skinner, 1982) is a 28-item True/False self-report scale designed to assess various negative consequences related to drug use including interpersonal, occupational, legal, medical, and psychological problems. Example items include: “Have you ever neglected your family or missed work because of your use of drugs?” and “Have you ever been arrested for driving while under the influence of drugs?”. Prior research has demonstrated that the DAST-28 has strong reliability and validity as an index of SUDs (Gavin et al., 1989; Johnson et al., 2025; Skinner, 1982).
Cannabis Motives
The Marijuana Motives Measure (MMM; Simons et al., 1998) is a 25-item questionnaire assessing five motives for using cannabis. The MMM was adapted from the Drinking Motives Questionnaire (DMQ) and was designed to parallel motives captured for alcohol use in cannabis use (Cooper, 1994). Each item on the MMM has a 5-point response option ranging from 1 “almost never/never” to 5 “almost always/always.” The five motives, each consisting of five items, are: 1) enhancement (e.g., “It makes me feel good”), 2) coping (e.g., “To forget about my problems”), 3) conformity (e.g., “To fit in with the group I like”), 4) social (e.g., “To be sociable”), and 5) expansion (e.g., “To know myself better”). The MMM has significantly predicted future cannabis use and cannabis-related problems (Simons et al., 1998). Factor analysis has consistently shown support for a five-factor solution, and the internal consistency of the subscales ranged from 0.70–0.91 (Simons et al., 1998; Zvolensky et al., 2007). In the current sample, internal consistencies were 0.95 for enhancement, 0.94 for coping, 0.79 for conformity, 0.94 for social, and 0.91 for expansion.
Data Analytic Plan
Latent profile analysis (LPA) was conducted to test our primary aim that a four-profile solution would best represent the data. LPA is a person-centered data analytic approach that identifies subgroups of individuals based on similar responding patterns (latent classes). Identification of the best-fitting model required both theoretical and statistical considerations. Several fit indices were examined to identify the best-fitting solution, including the Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), adjusted BIC, entropy, and the Lo-Mendell-Rubin likelihood ratio test (LMR-LRT). Class size, theoretical justification, and interpretability of the findings were also considered, and solutions that produced very small classes (i.e., <5% of the sample) were considered unstable and not retained. Upon identification of the best-fitting model, conditional probabilities for each class were examined to evaluate classification precision (i.e., average probabilities of falling into the identified class compared to alternative classes).
To test our secondary aim, the resulting profiles from the best-fitting LPA solution were examined for differences on several cannabis-related measures (i.e., lifetime, past-year, and past-30-day cannabis use, drug use problems, and motives for cannabis use). Group differences on outcomes were evaluated using the BCH method (Asparouhov & Muthén, 2014), a three-step approach that accounts for classification error when testing profile differences on external variables.
All analyses were conducted in Mplus Version 8.11 (Muthén & Muthén, 2023) using maximum likelihood estimation with robust standard errors (MLR). Missing data was handled using full information maximum likelihood (FIML).
Results
Descriptives
Participants reported on average 6.92 drinking occasions per week (SD = 7.23), with an average of 7.33 (SD = 4.14) standard drinks per occasion. The mean score on the SMAST was 7.66 (SD = 4.27), and 13.43 (SD = 8.08) on the DAST. Approximately 58% of participants reported using cannabis in the past year, and approximately 41% in the past 30 days (see Table 2 for more detailed use patterns). The most commonly endorsed other substances used in the past 30 days were cigarettes (86.86%), tranquilizers (30.15%), crack-cocaine (29.41%), cocaine (25.56%), and barbiturates (18.05%). See Table 3 for more information on other substance use.
Cannabis Use Frequency by Timeframe.
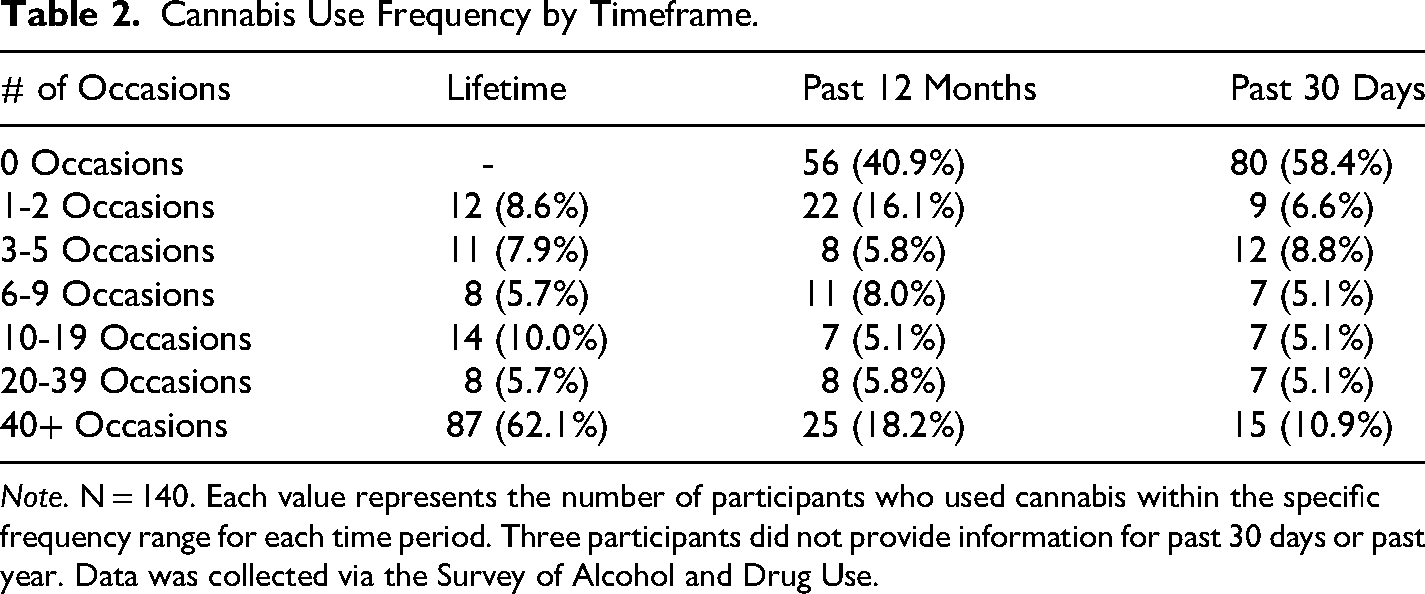
Note. N = 140. Each value represents the number of participants who used cannabis within the specific frequency range for each time period. Three participants did not provide information for past 30 days or past year. Data was collected via the Survey of Alcohol and Drug Use.
Substance Use History & Frequency.
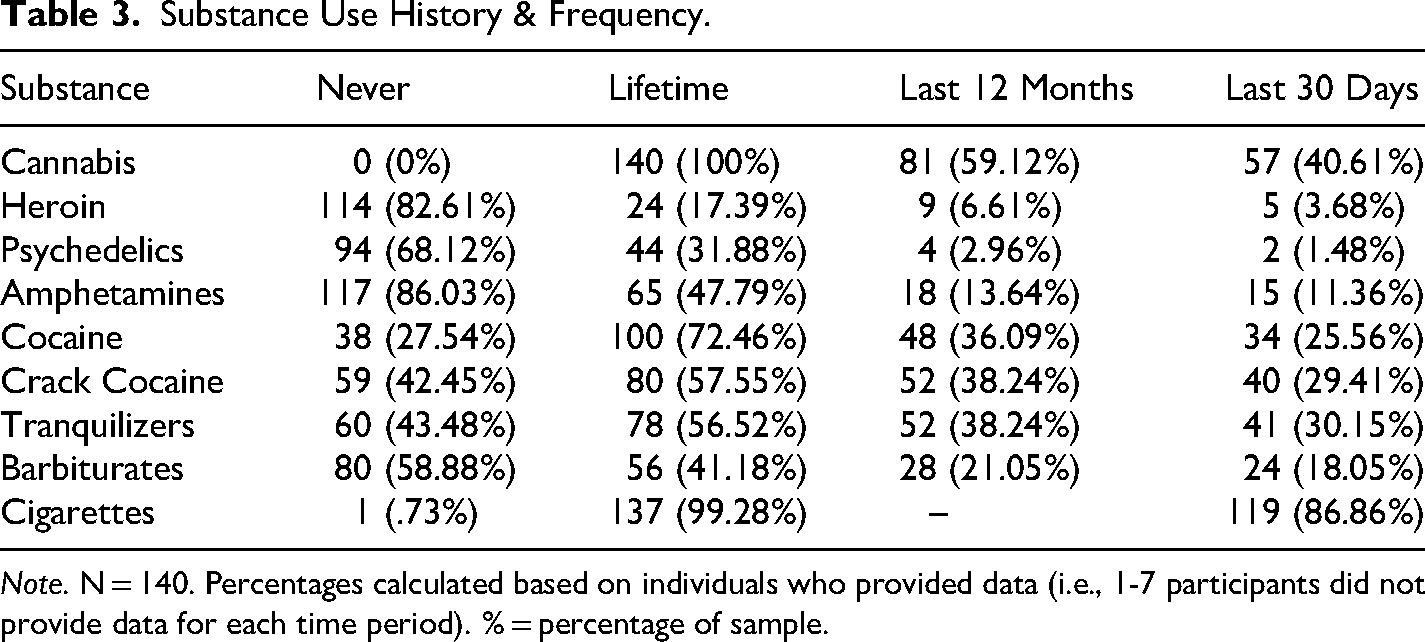
Note. N = 140. Percentages calculated based on individuals who provided data (i.e., 1-7 participants did not provide data for each time period). % = percentage of sample.
Specificity of Cannabis Craving
Given the polysubstance using nature of our sample, we also examined correlations between cannabis approach inclinations and frequency of individual substance use in the past 30 days (see Table 4). Results indicated that cannabis approach inclinations were strongly related to frequency of cannabis use in the past 30 days (r = .65, p < .001) but were minimally-to-moderately associated with frequency of other substance use in the past 30 days (i.e., correlations ranged from .05 for heroin to .40 for cocaine), representing a consistent pattern based on comorbid substance use patterns and providing some evidence of specificity to cannabis.
Correlates of Approach and Avoidance Tendencies by Substance and Duration of Use.
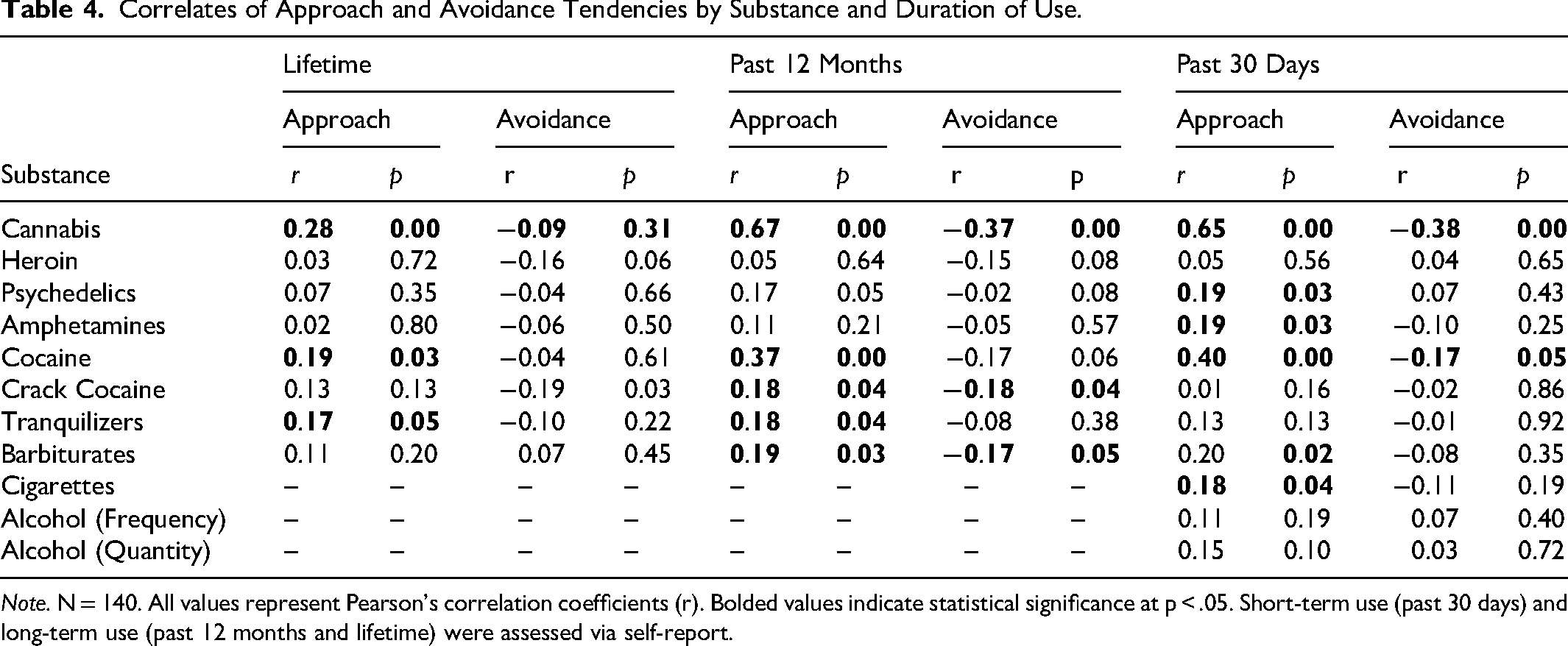
Note. N = 140. All values represent Pearson's correlation coefficients (r). Bolded values indicate statistical significance at p < .05. Short-term use (past 30 days) and long-term use (past 12 months and lifetime) were assessed via self-report.
Latent Profile Analysis
Fit indices supported a five-class solution (Table 5). The five-class model yielded the lowest BIC (1227.417), with minimal improvements in AIC and adjusted BIC beyond this point. Entropy was highest for the five-class solution (S = 0.946), indicating excellent classification accuracy. The LMR-LRT favored the five-class model over the four-class model (p = .035; four-class vs. three-class, p = .0497).
Latent Profile Analysis: Fit Indices.
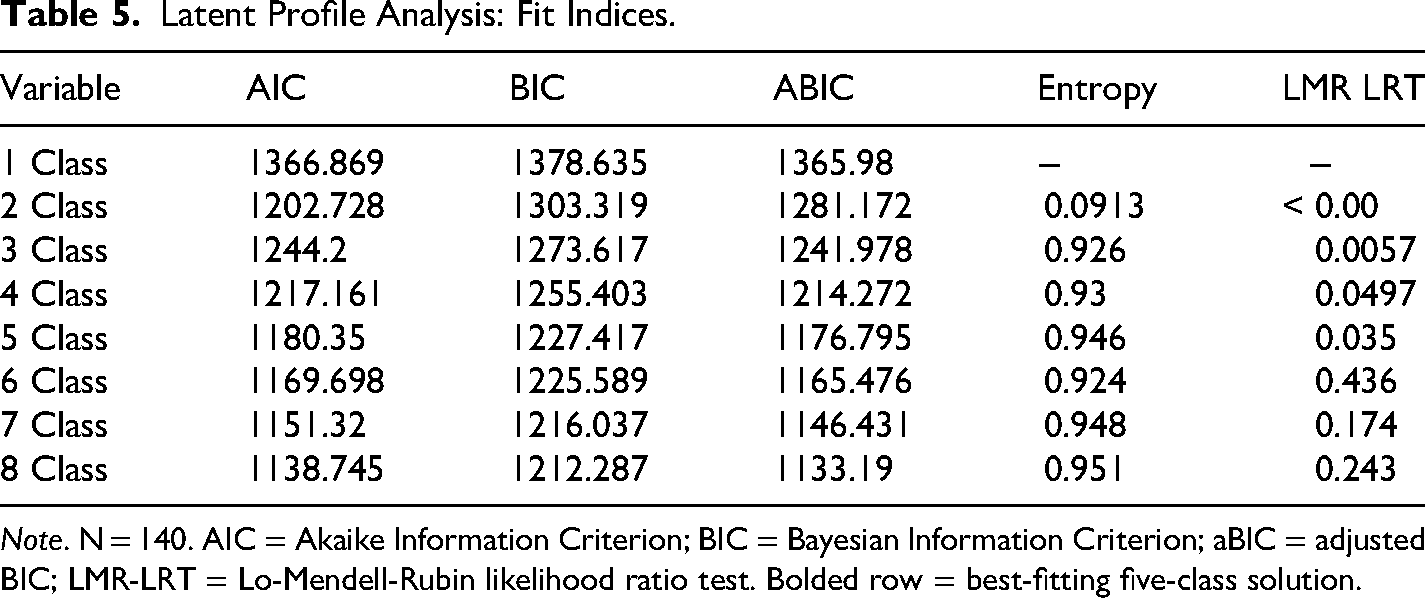
Note. N = 140. AIC = Akaike Information Criterion; BIC = Bayesian Information Criterion; aBIC = adjusted BIC; LMR-LRT = Lo-Mendell-Rubin likelihood ratio test. Bolded row = best-fitting five-class solution.
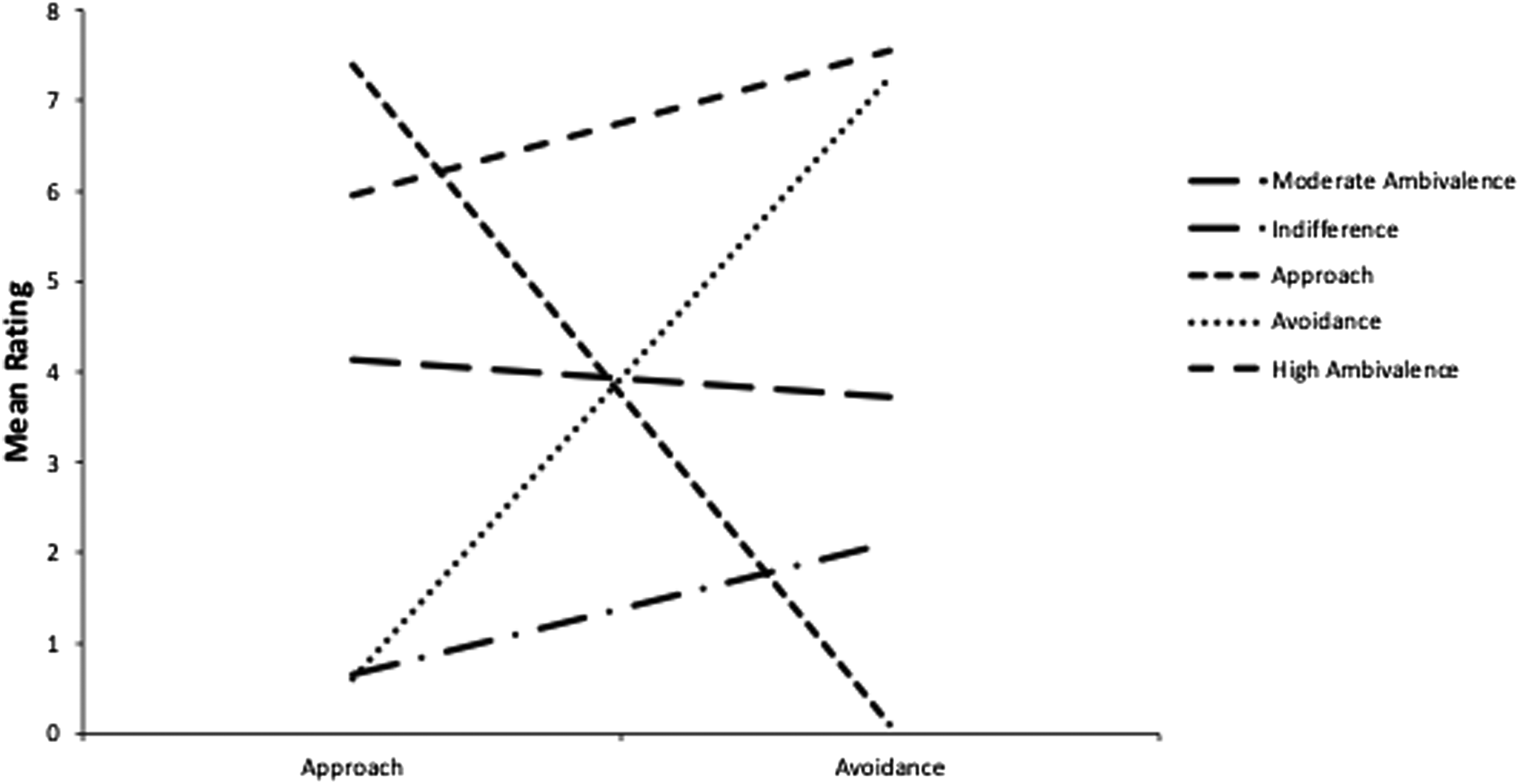
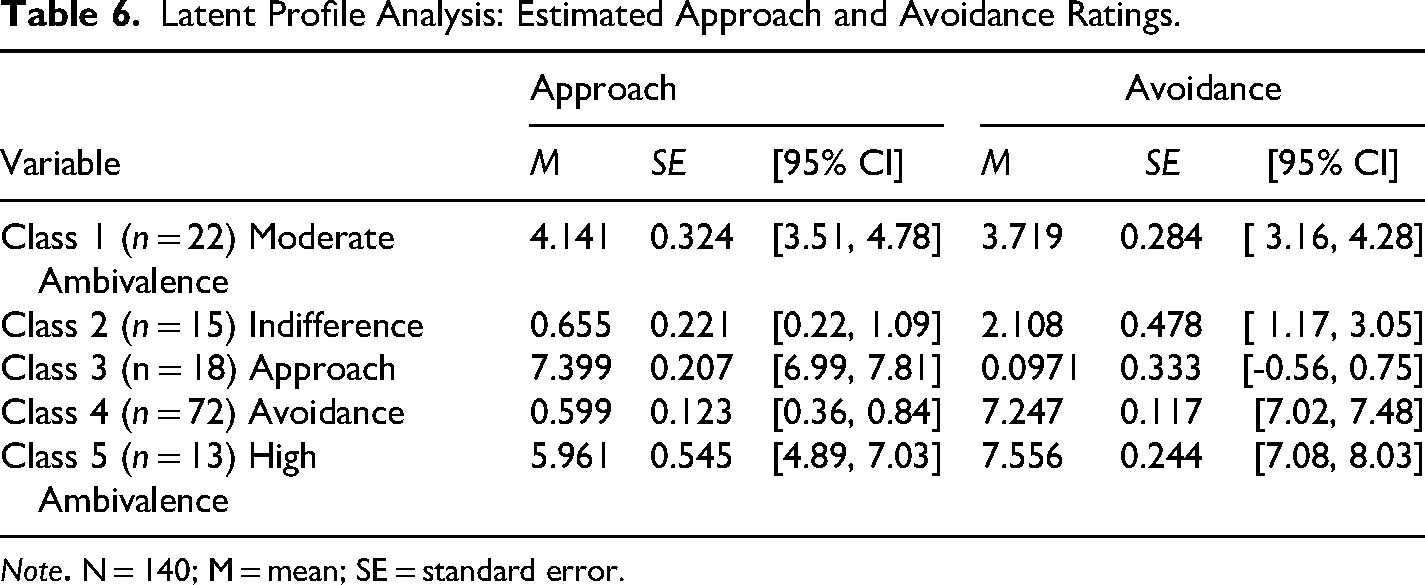
The final solution comprised five groups (see Table 6 and Figure 1): approach (Class 3; n = 18), indifferent (Class 2; n = 15), avoidance (Class 4; n = 72), moderate ambivalence (Class 1; n = 22), and high ambivalence (Class 5; n = 13). Conditional probabilities indicated strong classification precision: approach=0.965 (Class 1 = 0.033), indifferent=0.941 (Class 1 = 0.033), avoidance=0.984 (Class 5 = 0.024), moderate ambivalence=0.957 (Class 2 = 0.023), and high ambivalence=0.935 (Class 1 = 0.045). All classes except Class 5 (9.3%) exceeded the recommended 10% minimum for stability (Nylund-Gibson & Choi, 2018), supporting the interpretability of the five-class model.
Latent Profile Analysis: Estimated approach and avoidance ratings.
Latent Profile Analysis: Estimated Approach and Avoidance Ratings.
Note
Frequency of Cannabis Use
Lifetime use
Significant differences emerged across classes (χ2=60.94, p < .001). Participants in the approach group reported greater lifetime use than those in the moderate ambivalence (χ2=13.60, p < .001), avoidance (χ2=38.725, p < .001), and indifferent groups (χ2=7.18, p = .007). The high ambivalence group also reported greater lifetime use compared to moderate ambivalence (χ2=4.324, p = .038) and avoidance groups (χ2=7.843, p = .005; see Figure 2).
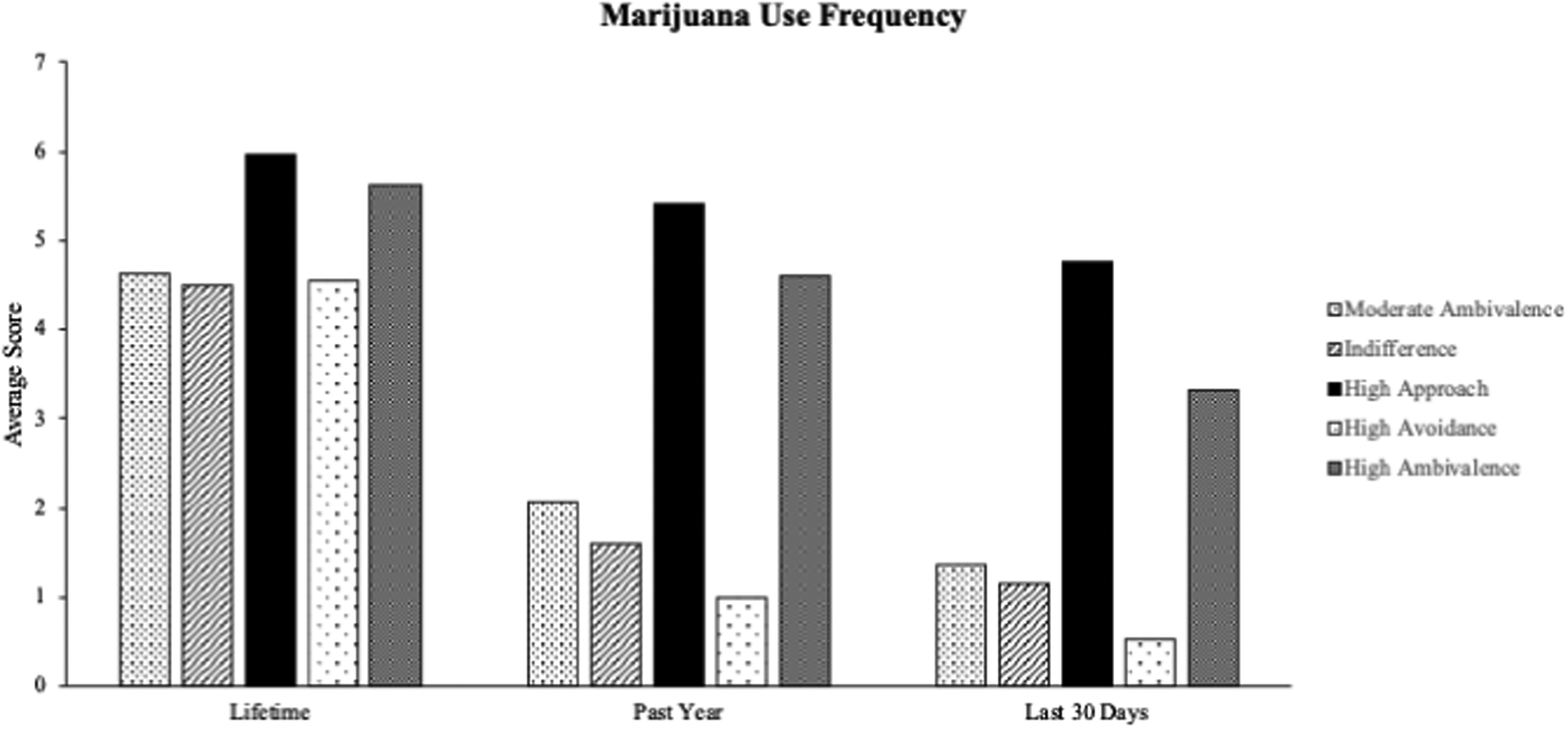
Cannabis Use Frequency by Class Membership. Note. Bars represent cannabis use frequency across the five classes. Cannabis use frequency.
Past 12-Month Use
Significant differences emerged across classes (χ2=147.277, p < .001; see Figure 2). The approach group reported greater past-year use than the moderate ambivalence (χ2=35.172, p < .001), avoidance (χ2=104.503, p < .001), and indifferent groups (χ2=31.460, p < .001). The high ambivalence group reported higher past-year use than the moderate ambivalence (χ2=11.091, p = .001), indifferent (χ2=13.183, p < .001), and avoidance groups (χ2=30.591, p < .001). The moderate ambivalence group reported greater use than the avoidance group (χ2=5.884, p = .015).
Past 30-Day Use
Significant differences emerged across classes (χ2=114.98, p < .001; see Figure 2). The approach group reported greater past-month use than the moderate ambivalence (χ2=38.813, p < .001), indifferent (χ2=37.186, p < .001), and avoidance groups (χ2=92.598, p < .001). The high ambivalence group reported higher past-month use than the moderate ambivalence (χ2=5.577, p = .018), indifferent (χ2=6.709, p = .010), and avoidance groups (χ2=13.905, p < .001). The moderate ambivalence group reported higher use than the avoidance group (χ2=4.397, p = .036).
Drug Use Problems
Results revealed significant differences across profiles (χ2=44.225, p < .001; see Figure 3). The approach group reported more drug-related problems than the avoidance group (χ2=4.56, p = .033). The high ambivalence group reported more problems than the approach (χ2=5.475, p = .019), moderate ambivalence group (χ2=26.045, p < .001), and avoidance groups (χ2=45.505, p < .001). The moderate-ambivalence group reported more problems than the indifferent group (χ2=3.870, p = .049), and the indifferent group reported more problems than the avoidance group (χ2=4.705, p = .030; see Figure 3).
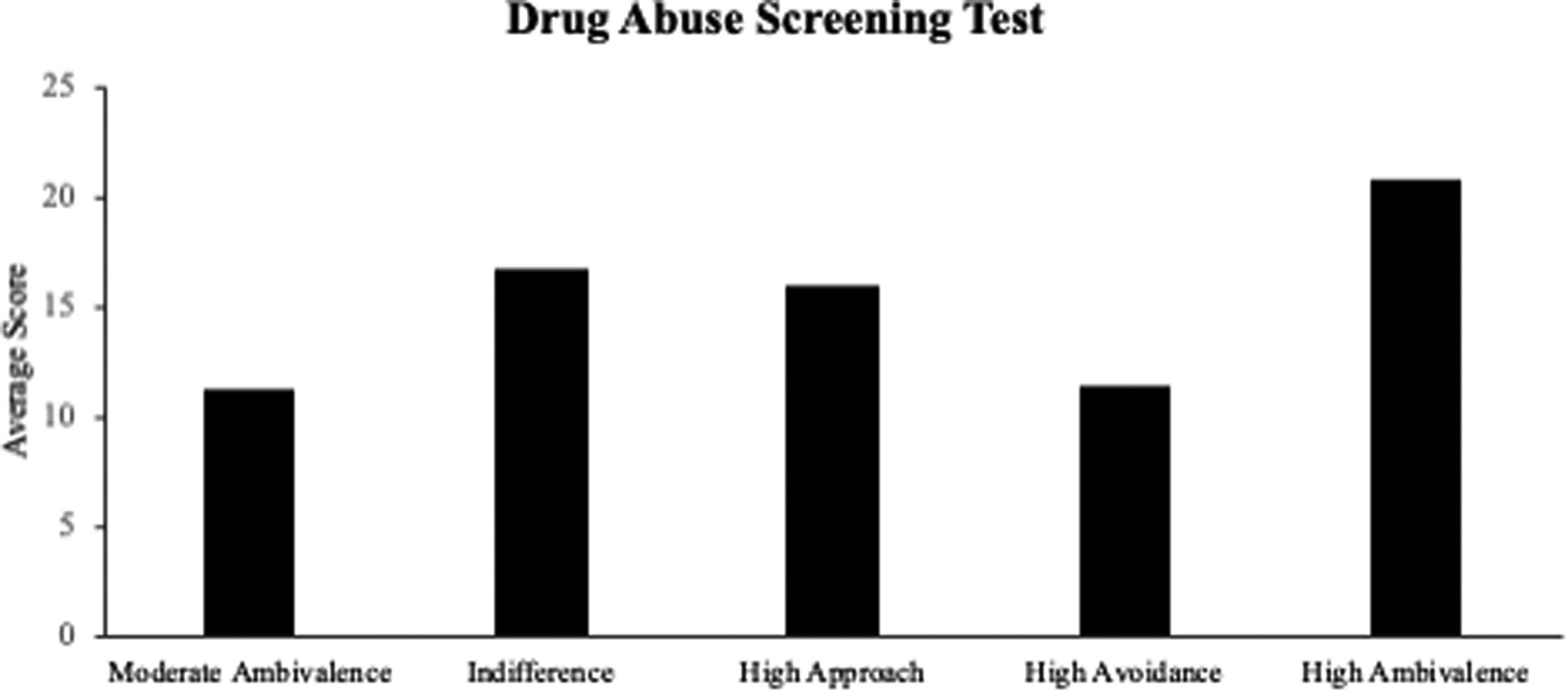
Drug Use Problems by Class Membership. Note. Bars represent mean Drug Abuse Screening Test (DAST) scores across the five-class solution. Scores range from 0-28 with higher scores indicating greater severity of drug-related problems.
Cannabis Use Motives
Significant differences were found between profiles for social (χ2=85.954, p < .001), coping (χ2=68.701, p < .001), expansion (χ2=28.348, p < .001), enhancement (χ2=184.54, p < .001), and conformity motives (χ2=9.905, p = .042; see Figure 4).
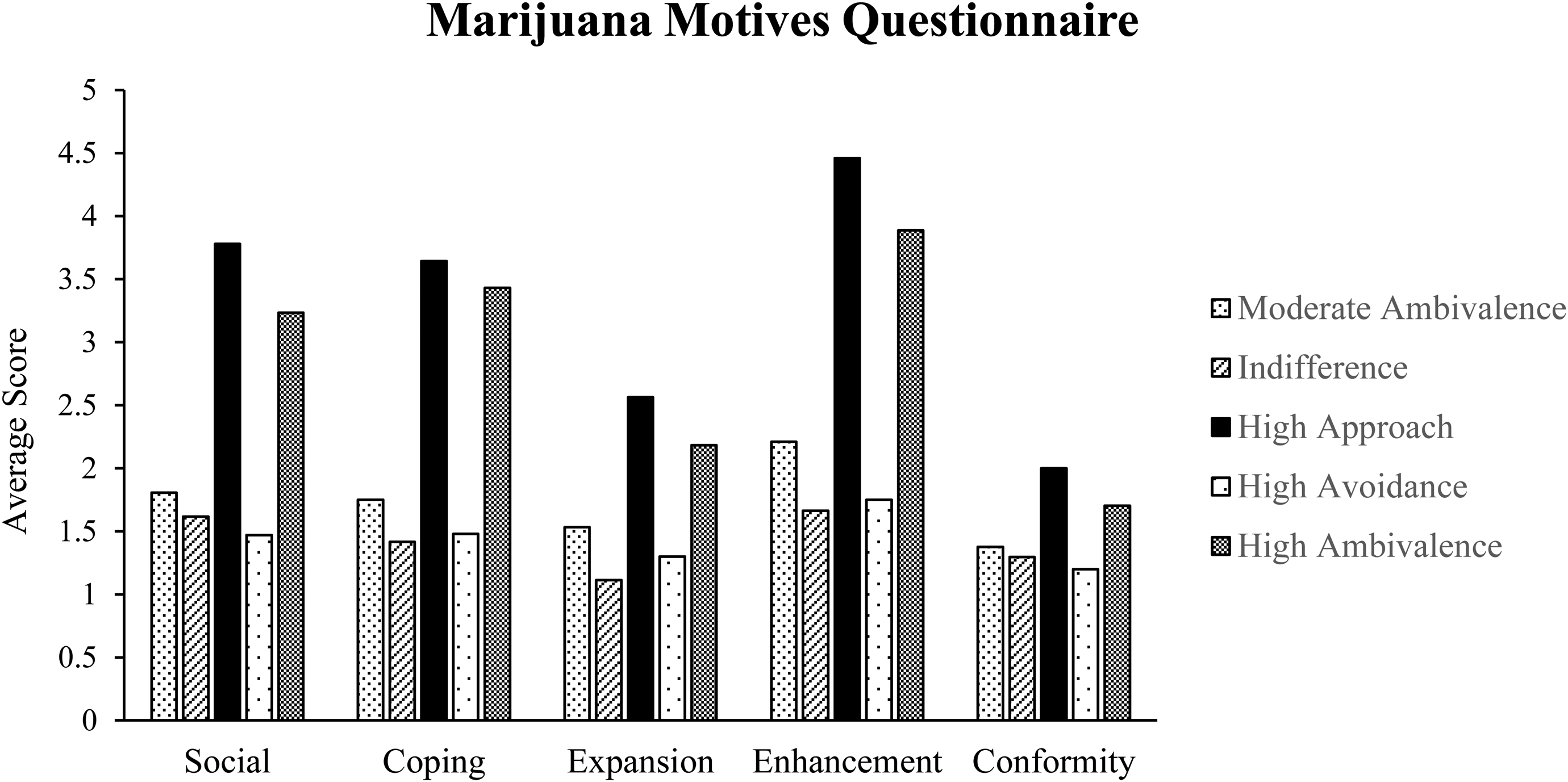
Marijuana Motives Questionnaire Endorsement by Class Membership. Note. Bars represent mean Marijuana Motives Questionnaire (MMQ) subscale scores across the five-class solution. Motives include Social, Coping, Expansion, Enhancement, and Conformity. Scores range from 1 (almost never/never) to 5 (almost always/always).
Social Motives
The approach group endorsed stronger social motives than the moderate ambivalence (χ2=26.307, p < .001), indifferent (χ2=25.751, p < .001), and avoidance groups (χ2=23.996, p < .001). The high ambivalence group endorsed higher social motives than the moderate ambivalence (χ2=10.632, p = .001), indifferent (χ2=25.751, p = .001), and avoidance groups (χ2=23.996, p < .001).
Coping Motives
The approach group reported greater coping motives than the moderate ambivalence (χ2=22.038, p < .001), indifferent (χ2=25.109, p < .001), and avoidance groups (χ2=29.829, p < .001). The high ambivalence group endorsed higher coping motives than the moderate ambivalence (χ2=15.678, p < .001), indifferent (χ2=19.466, p < .001), and avoidance groups (χ2=29.829, p < .001).
Expansion Motives
The approach group reported greater expansion motives than the indifferent (χ2=16.978, p < .001) and avoidance groups (χ2=12.709, p < .001). The high ambivalence group reported greater expansion motives than the indifferent (χ2=12.211, p < .001) and avoidance groups (χ2=8.230, p = .004).
Enhancement Motives
The approach group reported stronger enhancement motives than the moderate ambivalence (χ2=40.061, p < .001), indifferent (χ2=57.801, p < .001), avoidance (χ2=130.470, p < .001), and high ambivalence groups (χ2=4.611, p = .032). The high ambivalence group endorsed stronger enhancement motives than the moderate ambivalence (χ2=21.433, p < .001), indifferent (χ2=35.122, p < .001), and avoidance groups (χ2=74.804, p < .001).
Conformity Motives
The approach group endorsed greater conformity motives than the indifferent (χ2=3.829, p = .050) and avoidance groups (χ2=6.686, p = .010).
Discussion
Latent profile analysis (LPA) revealed five distinct cannabis-craving motivational profiles among adults reporting polysubstance use and receiving inpatient treatment for AUD/SUD. Consistent with the AMC, motivational profiles reflecting indifference, approach, avoidance, and ambivalence were identified. Further, these profiles demonstrated theoretically important differences on both frequency of use and problems associated with drug use. Specifically, approach (i.e., high approach, low avoidance) and high ambivalence (i.e., high approach, high avoidance) reported the highest rates of cannabis use (i.e., lifetime, past-year, past-month) and greater drug-related problems. In contrast, indifference (i.e., low approach, low avoidance) and avoidance (i.e., high avoidance, low approach) were characterized by less overall cannabis use frequency, with avoidance demonstrating the lowest frequency of past-month use.
Although a four-class solution was predicted, results revealed a fifth class characterized by moderate ambivalence. The emergence of this moderate ambivalent profile is not unique, as a previous LPA study (i.e., Schlauch et al., 2015) examining craving for alcohol in this same sample found a similar five-class solution. The moderate ambivalence group may be reflective of more recreational use with the potential of developing problematic use. Although the moderate ambivalence group demonstrated similar levels of use as those in the indifferent profile, descriptively they were higher on cannabis use motives compared to those in the indifferent group, and lower when compared to high ambivalence, suggesting a pattern of underlying motivational processes that may be predictive of future heavy use and problems (Bresin & Mekawi, 2019). Future research examining how these dimensions of craving change over time will be important for understanding potential transitions from moderate to high ambivalence, including the influence on patterns of use among samples where cannabis use is primary.
The AMC predicts that expectancies, or the anticipated effects of alcohol or drugs, serve as an important contributory factor in the development of both approach and avoidance inclinations (e.g., Breiner et al., 1999). Indeed, motivational theories of AUD (e.g., Cox & Klinger, 2004) posit that expectancies combine to influence (consciously or unconsciously) the decision to use a substance in a given situation (i.e., motives). Consistent with these theories and the AMC, findings indicated stronger motives to use among those with higher approach inclinations (i.e., approach and high ambivalence profiles), particularly with respect to motives to enhance social experiences, reduce negative affect, and enhance positive affect, suggesting that the positive and negative reinforcement of cannabis use are associated with more developed approach inclinations. Prospective research will be needed to better understand how these processes unfold over time, including how expectancies/motives influence approach/avoidance inclinations.
Theoretical, Methodological, and Clinical Implications
Theoretically, findings provide support for cannabis craving as a multidimensional phenomenon characterized by the competing desires to approach a substance and to avoid a substance. In this sample, the concurrent assessment of both approach and avoidance inclinations was uniquely associated with cannabis-related variables, suggesting that considering both dimensions may offer additional insight into patterns of use. Indeed, previous studies have demonstrated that avoidance inclinations predict unique variance in substance use related variables (e.g., Schlauch et al., 2013a, 2013b). In addition, consistent with the alcohol use literature (e.g., Schlauch et al., 2015), results show that among those reporting polysubstance use, cannabis craving can be mapped onto an “evaluative space” within the dimensions of approach and avoidance inclinations and be differentially associated with patterns of use. The consideration of a separate, yet concurrent, dimension of avoidance may help to explain why some individuals may be able to restrain themselves from using substances despite relatively strong approach inclinations, as use is likely determined by the relative strength, with avoidance playing an important role in decision-making (e.g., Stritzke et al., 2007).
Methodologically, craving conceptualized as an approach-avoidance conflict has the potential to explain additional variance in treatment outcomes. Without consideration of avoidance inclinations, traditional craving ratings (those measuring approach only) may represent attenuated scores, as participant responses may be the summation of both desires. Indeed, within the cannabis use literature, neurophysiological indices of cue-induced craving often elicit greater responses from baseline when compared to self-report indices (Norberg et al., 2016), suggesting that unidimensional self-reports may be under-reporting true levels of craving intensity.
Support for the AMC in cannabis use may offer novel approaches to treatment, including mechanisms of behavior change. Historically, treatments targeting craving (both pharmacological and psychological) have focused primarily on approach inclinations (e.g., CBT - Urge Surfing module). Approach inclinations are clearly important in the prediction of patterns of use; however, it has been posited that fluctuations in avoidance inclinations may be a stronger predictor among those seeking to change substance use patterns (e.g., Stritzke et al., 2007), which has empirical support in the alcohol literature (e.g., Schlauch et al., 2019). Assuming such findings hold for those seeking to reduce their cannabis use, targeting avoidance inclinations in treatment may prove beneficial. For example, enhancing positive affect may result in both lower approach and higher avoidance inclinations (see Schlauch et al., 2013c) and enhance self-regulation (Shmueli & Prochaska, 2012; Tice et al., 2007). Thus, it is not surprising that behavioral activation and “positive addictions” such as exercise and meditation that can enhance positive affect are encouraged in most contemporary addiction treatment programs (Marlatt & Witkiewitz, 2005). Indeed, aerobic exercise training has been shown to reduce cannabis craving and use in cannabis-dependent adults (Buchowski et al., 2011). Future research will be needed to see if such strategies have similar effects on avoidance inclinations.
Limitations
Several limitations should be considered. First, data were collected from 2009–2010, and the cannabis landscape has changed substantially since that time, including increases in product potency, new cannabis products, shifts in legalization, and changing cultural norms surrounding cannabis use. As such, the present findings should be interpreted within the context of a substantially different cannabis environment. Although the underlying mechanisms proposed by the AMC, namely the development of approach and avoidance inclinations based on the positive and negative consequences of use, are not expected to fundamentally differ across time periods, these broader contextual changes may influence the relative strength or development of these inclinations within individuals. Future research should examine whether similar motivational profiles emerge within more contemporary samples of participants who use cannabis. Additionally, some cannabis cues used in the cue-reactivity paradigm may now be outdated or not reflective of current recreational use or packaging.
Second, LPA is sensitive to class sizes. There were several classes with smaller n's, representing 9.3%, 10.7%, and 12.9% of the total sample. Given that cannabis was not the primary reason for many participants receiving SUD treatment (most were receiving detox for alcohol), it was unsurprising that fewer participants fell into the approach and high ambivalence classes. These smaller n's are partially mitigated by recommendations suggesting that classes should not contain less than 10% of the total sample size (Jung & Wickrama, 2008), and some may be expected to have approximately 10%. However, the relatively small and uneven class sizes likely limited statistical power, reduced the stability of some class-specific estimates, and, coupled with the number of BCH comparisons conducted, mean that some marginal differences may reflect Type I error and should be interpreted cautiously, particularly for the smallest classes. Given the relatively small and uneven class sizes, findings should be interpreted as preliminary and in need of replication in larger samples.
Third, many participants used multiple substances and were presented with several alcohol and drug cues as part of the cue-reactivity, making it difficult to fully disentangle cannabis-specific craving from broader substance-related motivational processes. Although previous work has established the validity of the current methodology (Schlauch et al., 2013a; Stritzke et al., 2004) and follow-up analyses suggested that cannabis approach inclinations were more strongly associated with cannabis use than with other substance use, these findings do not conclusively establish specificity. It remains possible that observed craving responses reflect, in part, generalized approach tendencies or cross-substance cue reactivity. Future research replicating findings in samples reporting primary cannabis use is warranted.
Lastly, participants were also in acute detoxification (typically for alcohol), and withdrawal status may have affected responses. For example, acute withdrawal and the use of medications to control such withdrawal symptoms may affect general arousal ratings and subsequent craving responses. However, such concerns may be mitigated by several factors. There is literature suggesting that those in withdrawal and receiving detoxification medication (i.e., chlordiazepoxide) do not differ on cue-elicited approach craving compared with those not requiring detoxification (Monti et al., 1993). In fact, findings from Monti and colleagues suggest that the greatest reactivity to cues occurs early in treatment and that such effects are not moderated by withdrawal status. Thus, it is possible that early on in the detoxification process (i.e., 2.3 days on average in the current sample), reactivity ratings would be enhanced rather than attenuated. However, it is unknown how withdrawal from alcohol or other substances may impact craving for another substance. Future research exploring alcohol and drug withdrawal on craving responses will be important for understanding risk of lapses and relapses among those reporting polysubstance use.
Conclusion
The current study provides empirical support for the AMC related to cannabis use among an inpatient treatment sample reporting polysubstance use. While preliminary, findings demonstrate that cannabis craving is multidimensional, with distinct profiles of approach and avoidance inclinations that differentially relate to patterns of cannabis use, motives, and drug-related problems. Assessing both approach and avoidance provides a more nuanced understanding of craving and may inform targeted interventions, particularly those aimed at enhancing avoidance inclinations to support reductions in use.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.