
Abstract
Rural healthcare communication networks are geographically dispersed, historically layered, and technologically uneven, sustained through evolving interpersonal and improvised ties that resist bounded frameworks like actor-network theory. This study shows how social network mapping, informed by assemblage theory, reveals coverage gaps, fragile hubs, referral chokepoints, and uneven service distribution. These loosely coupled, resource-constrained systems rely on regional patient travel, nonphysician providers, and aging infrastructure amid workforce, demographic, and funding pressures. Using concepts such as emergence and deterritorialization, we interpret these networks as adaptive yet unstable. Mapping indicates low density, centralization, weak reciprocity, and long-distance referrals, supporting artificial intelligence–enabled coordination, telehealth expansion, and improved continuity of care.
Keywords
When researching rural healthcare, the ability to visualize existing and potential communication networks can be a major challenge. Rural healthcare networks tend to involve many overlapping layers that include ad hoc and multilateral connections among healthcare providers, facilities, government agencies, and the patients they serve (Hulme et al., 2022). Rural healthcare networks are also dispersed across large geographic regions and tend to depend on interpersonal relationships that have developed over time (Evans et al., 2022; Weiss et al., 2020). Many of these relationships began as personal interactions among healthcare providers, civic leaders, and patients (Coombs et al., 2022). Then, as the original providers and patients leave the network, the pathways often continue as new healthcare workers replace those who have left. Rural healthcare communication networks are also usually reliant on older technologies, such as legacy phone systems, outdated computers, local area networks, and second- or third-generation (2G/3G) cell towers, which can create unreliable information flows and lead to outages (Pai & Bahalkeh, 2025). Without a clear way to visualize these networks, policymakers, administrators, and researchers sometimes struggle to figure out how rural healthcare networks can be reformed and integrated into larger networks can be difficult. More than likely, this problem will become even more complex as artificial intelligence (AI) is integrated into healthcare communications, because connections will be automated and even less visible.
When studying healthcare communications, researchers have typically used actor-network theory (ANT), developed by Bruno Latour in his books Science in Action (1987) and Reassembling the Social: An Introduction to Actor-Network-Theory (2005). Actor-network theory can be useful for examining how networks of human and nonhuman actors emerge, stabilize, and codify everyday practices. Actor-network theory has been particularly effective for researching bounded settings such as laboratories, clinics, and hospitals, where relationships among people, technologies, protocols, and institutions are more visible and easier to trace (Cresswell et al., 2010; Ryan et al., 2024). However, in rural healthcare contexts, networks are often widely dispersed, layered historically, shaped by social and cultural forces, and sustained through informal or improvised connections. They frequently develop through contingencies, workarounds, and local knowledge, making it difficult to identify stable actors, clear boundaries, or durable inscriptions. As a result, ANT may not be the right approach for studying the fluid, shifting, and partially obscured relations that characterize rural healthcare communication (Nickerson, 2025; Whittle & Spicer, 2008).
Recognizing these limitations, we decided to study rural healthcare networks through assemblage theory, as first described by Deleuze and Guattari (1989) and later elaborated by Manuel DeLanda (2016). As defined by Pellegrini and Johnson-Sheehan (2020), “An assemblage is a multiplicity or unity that is self-organizing and continuously in a process of becoming. As an entity in flux, an assemblage is made up of a heterogeneous whole of humans, machines, objects, and ideas that are themselves emerging, evolving, and growing.” Assemblage theory allows communication researchers to approach rural healthcare networks as self-organizing, contingent, evolving, and ultimately transitory. In assemblage theory, relationships and patterns within a network are viewed as emerging and evolving over time, rather than being intentionally designed. Assemblage theory assumes these networks arise through improvised interactions among people, technologies, practices, and geographies, usually without a central plan or blueprint (Trnka, 2021). As a result, they form through historical contingencies shaped and constrained by local practices, economic limitations, and sociocultural values. Assemblage theory is particularly useful for researching in these contexts because it emphasizes the communication pathways between nodes rather than the nodes themselves, enabling researchers to study how networks emerge, take form, strengthen, and sometimes destabilize (Buchanan, 2021). Therefore, assemblage can be better suited for analyzing evolving and complex systems such as rural healthcare networks.
This article is part of a larger research project on the impacts and potentialities of generative AI in rural healthcare. 1 Specifically, in this article, we will show how social network mapping (SNM), when informed by assemblage theory, can help researchers better visualize rural healthcare networks. We demonstrate how SNM makes visible the layered, contingent connections among clinics, hospitals, libraries, pharmacies, public health offices, first responders, and informal caregivers that can be difficult to see in rural contexts. We will show how SNM can reveal communication gaps, redundancies, and chokepoints that restrict or impede access to care. These maps not only illuminate existing networks but also serve as tools for identifying opportunities to use telehealth and generative AI to improve information flow, strengthen collaboration, and ultimately support healthcare providers while improving patient health in rural communities.
Theory: Rural Healthcare Networks as Assemblages
Let's begin by stating that rural healthcare networks work differently from their urban and suburban counterparts, even though all healthcare networks provide patient care and promote community health. These differences are due to patient demographics, organizational structures, available resources, and modes of delivery (Cyr et al., 2019; van Dis, 2002). Urban and suburban systems are typically organized around central hubs, such as hospitals and government services. In contrast, rural healthcare networks often lack formally integrated hubs. Instead, care is delivered through loosely coupled networks of facilities that often operate independently from others around them and rely on ad hoc coordination (Creel et al., 2024; Matthews et al., 2017). For example, our research area included four family health clinics that function as their own independent network. They are not formally affiliated with regional rural hospitals or urban hospitals. These clinics offer limited services, operate with smaller staff, and are heavily dependent on nonphysician healthcare providers such as nurses, physician assistants, and certified nursing assistants. As a result, basic care and urgent care are usually the main concerns. Patients who need more specialized treatment or emergency care are typically transported by cars, ambulances, or helicopters to urban or suburban hospitals for treatment.
The infrastructure within rural healthcare networks also tends to be less formalized than in urban and suburban systems. In rural areas, there are appointed county health officers who monitor county-level care, but these officers are often employed half-time and, as our surveys showed, sometimes do not even live in the counties they serve. Meanwhile, healthcare services are usually unevenly distributed across geographic regions. One county may have a primary care clinic, while another county has a pharmacy. Nearby counties may have dental practices, a substance use treatment facility, or an assisted living facility. Some rural counties have no healthcare services, except perhaps Emergency Medical Services (EMS) personnel who tend to be operating out of the county seat or the largest town in the county.
This uneven distribution means patients routinely need to cross county lines to access even basic or urgent care. For specialized care, such as OB/GYN services, dialysis, and cancer treatments, patients often need to travel significant distances to the closest suburban or urban hubs. These structural limitations place stress on the networks and the people working inside them. These stresses are made more acute when factoring in provider turnover and shortages, aging patient populations, transportation barriers, declining local budgets, and shifting state and federal policy environments.
Assemblage theory offers a productive way to describe and understand these complex healthcare systems (Woods, 2025; Ivanova et al., 2016) because researchers can view these networks as self-organizing and evolving assemblages of people, technologies, policies, infrastructures, spaces, and relationships. An assemblage, in Deleuze and Guattari's sense, is a multiplicity that emerges and evolves contingently over time, often along communication pathways (Pelligrini & Johnson-Sheehan, 2020). The relationships among the assemblage's elements (humans, machines, objects, facilities) are often self-organizing and mutating in ways that are shaped by local conditions.
We have found four core concepts from assemblage theory especially helpful when studying communication pathways in rural healthcare networks: emergence, exteriority, territorialization, and deterritorialization.
Emergence and Exteriority
Following DeLanda's understanding of assemblage theory, emergence occurs because “the properties of a whole [are] caused by the interactions between its parts” (2016, p. 9). In rural healthcare, emergence happens because the parts, which we will call “elements” in this article, are always in flux in relation to each other. The assemblage adapts, changes, grows, and devolves as elements change (e.g., key clinicians arrive or leave, clinics or hospitals open or close, computers are upgraded or become obsolete, and government and insurance reimbursement guidelines change). When this happens, other elements respond to these changes (DeLanda, 2016).
Exteriority reveals how elements within the network retain their own autonomy, helping explain how assemblages can be impacted and shaped by forces outside the system, such as state funding decisions, broadband availability, cultural attitudes toward health and healthcare institutions, and changes in regional labor markets. As Pelligrini and Johnson-Sheehan write, “an economy of affect is created as elements within an assemblage emerge and put external pressure on other elements” (p. 192). Exteriority also allows researchers to identify assemblages within assemblages, such as smaller networks of clinics, pharmacies, or libraries that operate independently of each other.
Territorializing and Deterritorializing
Territorializing is helpful for describing how an assemblage stabilizes and extends its capacities. When an assemblage is growing, as described by Deleuze and Guattari (1989), it collectively territorializes new spaces by formalizing habits and traditions, establishing or adapting their communication infrastructures, and codifying standard operating procedures (see also Slack & Wise, 2005). Territorialization draws attention to the intersecting and evolving communication pathways within a network, rather than to individual actors or institutional nodes. In rural healthcare contexts, communication often functions through personal relationships and improvised workarounds that have become normalized over time within the assemblage. These informal relationships are sometimes the most practical and reliable channels because referral pathways can be contingent, health records are inconsistent across systems, and patients face physical, cognitive, and technological limitations. As Nail (2017) describes territorializing, elements “can be added, subtracted, and recombined with one another ad infinitum without ever creating or destroying an organic unity” (p. 23).
Changes within the assemblage ripple outward: a head nurse retires, telehealth becomes available, or a factory that offered health insurance coverage shuts down. When an assemblage is functioning normally, territorialization allows elements to stretch, adjust, pull apart, reform, renegotiate, and reconstitute themselves over time. These shifts may require healthcare providers to take on additional or redefined roles. Clinics or hospitals may begin offering new services, such as adding an in-house pharmacy or using telehealth to provide psychological services. Referral pathways adapt, mutate, or newly form to stabilize these changes. As DeLanda (2016) notes, the term “lines of flight” describes situations in which new relationships, innovations, crises, or ideas compel reconfigurations of existing communication pathways, even prompting new assemblages to form. In other words, changes in communication pathways typically emerge from ongoing interactions among multiple elements rather than from the deliberate decisions of any single actor or coordinated group.
According to DeLanda's understanding of assemblage theory, deterritorialization refers to situations in which an assemblage becomes destabilized (e.g., when routines, roles, or institutional boundaries lose their coherence). This creates pressure on elements of the assemblage to reconfigure or reform. Not surprisingly, deterritorializing has become the norm in today's strained rural healthcare networks. Established routines or procedures don’t seem to function as well as they did before. Key elements in the assemblage withdraw or change their roles. Institutional boundaries shift or become more porous. In most cases, deterritorialization is natural and even necessary, causing assemblages to contract, adjust, and respond. For example, in some cases, policies or funding are changed or cut. A physician or dentist retires. Disruptive technologies like AI emerge. Communication pathways become frayed or shut down. Right now, for example, rural healthcare facilities are being mandated to update their health records, transitioning from paper records to EHRs. These upgrades will ultimately enhance communications, but right now they require significant resources and labor. Meanwhile, cybercriminals have been targeting clinics and hospitals, which is also compelling upgrades to computer systems and cybersecurity practices. These destabilizing shifts can temporarily weaken an assemblage's existing relationships, but reconfigurations and reterritorializations may ultimately lead to new forms of stability.
Demographic changes in rural areas are also deterritorializing healthcare communication practices. Younger and college-educated people have been gravitating toward urban and suburban areas as factories, professional jobs, and government funding decline in rural regions. Meanwhile, healthcare, agricultural, and construction jobs are being filled by immigrants from Central America, South America, and Africa. These demographic shifts have created social and cultural tensions in which older rural patients (often White or Black) are increasingly cared for by immigrant healthcare workers, who speak English as a second language, are resource-limited, and sometimes undocumented.
Deterritorializing can also result from exterior financial jolts that test rural healthcare resilience. Cuts to government funding, including cuts to Medicaid and the Affordable Care Act, have sent shockwaves through rural networks. For example, during one of our site visits to a clinic in early 2025, the clinic's administrators were acting quickly to transfer funds into new accounts because the so-called Department of Government Efficiency was clawing back funding.
The Resilience and Fragility of Assemblages
Assemblage theory's four concepts, emergence, exteriority, territorialization, and deterritorialization, allow researchers to explore how rural healthcare networks stabilize or extend care through referral routines, shared records, and long-standing relationships. At the same time, these concepts help explain why rural healthcare networks can be simultaneously resilient and fragile. Personnel turnover, obsolete technologies, unplanned policy shifts, or the loss of key providers, facilities, and funding can degrade and put pressure on rural healthcare assemblages. They can also prompt adaptation and reform through new technologies such as EHRs, telemedicine, and increasingly AI. Like any assemblage, rural healthcare networks have a collective agency, and they are capable of mutating, recombining, and reforming under pressure (Deleuze & Parnet, 1987). Yet, they remain susceptible to both exterior and interior shocks when larger elements in the assemblage change, leave, or shut down. This tension helps explain why healthcare researchers regularly describe rural healthcare in the United States as existing in a persistent “state of crisis.”
Methodology: SNM
As part of a larger project funded by the North Central Regional Center for Rural Development, our team used SNM to identify and describe healthcare communication networks in the rural counties surrounding Tippecanoe County in northcentral Indiana. Social network mapping is a method derived from social network theory and analysis (SNA or SNTA), which “emerged over the past 100 years from a niche discipline to applications spanning many fields of the social, physical, and biological sciences” (Valente et al., 2015). Social network mapping examines how communication networks operate within physical spaces by mapping relationships among people, institutions, technologies, and locations (Borgatti et al., 2009; Goodchild, 2007). Rather than focusing on individual actors, it emphasizes connectivity and the movement of information across distance and infrastructure, making it especially valuable for community planning in settings where communication pathways may be uneven, contingent, or informally maintained.
As described by Valente et al. (2015), SNM allows researchers to consider several “measures,” which form a vocabulary for analyzing network maps, including the following:
Component—sets of human and nonhuman elements (people, facilities, technologies, ideas, policies) that can communicate with other nodes in the assemblage Density—the proportion of ties in a network in proportion to all connections in the network Centrality—the prominence of a specific element (human or nonhuman) relative to the total possible ties in the network Centralization—situations in which clusters of links and nodes form around a few elements in the network Reciprocity—happens when communications between elements occur in both directions Transitivity—the tendency for two nodes that are connected to a third node to also be connected to each other.
These components and measures help define what is being observed and how each element (human and nonhuman) is situated within the network.
SNM has broad applications in healthcare. It is most often used for descriptive analysis, such as identifying patterns, relationships, and gaps in coverage. It can also support interventions designed to improve collaboration or accessibility. As Saatchi et al. (2023) note, “the majority of the papers used SNA for descriptive purposes only,” with relatively few studies measuring outcomes tied to SNA-based interventions. In healthcare systems research, network mapping has been used to examine physician collaboration networks, showing how provider relationships influence hospital outcomes, such as length of stay, cost, and patient satisfaction (Uddin, Hamra & Hossain, 2013). The SNA can also be used to visualize shared care patterns that support quality improvement and accountable care initiatives (Flemming et al., 2022). As a methodological tool, it quantifies relationships, assesses network structure, and defines boundaries, helping researchers identify nodes, communication gaps, and bottlenecks. Metrics such as centrality and density reveal opportunities for collaboration and coordination within the network (Monaghan, Lavelle & Gunnigle, 2017). The SNA has also been used to study communication among public health agencies during crises; for example, a North Carolina pilot study analyzed information-sharing patterns during the H1N1 outbreak (Bevc et al., 2011).
One advantage of using SNM in rural healthcare research is its common interest with assemblage theory in studying communication pathways, evolving relationships, and uneven geographical and political landscapes. SNM enables researchers to create snapshots of an assemblage, revealing existing connections among heterogeneous elements. Over time, these snapshots can be used longitudinally to understand how a rural healthcare assemblage evolves as it territorializes and deterritorializes, and how relationships among elements stretch, adjust, expand, contract, and reconstitute.
SNM is similar to but differs in important ways from geographic information systems (GIS). SNM emphasizes relational structures and interaction patterns among elements in a network, whereas GIS emphasizes spatial relationships and layered geospatial data. SNM is more relational and selective, suited to studying logistics, community planning, resource management, and communication practices, while GIS is more comprehensive and fine-grained, because it incorporates satellite imagery, demographic data, and multiple geospatial layers. For our study, SNM allowed us to create maps that capture moments in the evolution of the assemblage without requiring the broader interpretive scope of GIS. At the same time, GIS-based network mapping could be used to evaluate travel time, infrastructure gaps, and access to facilities, helping identify underserved regions and inform facility placement (Abd Jalil et al., 2018). GIS can also identify disparities due to factors such as insurance, cost, aging populations, and facility distribution (Svynarenko et al., 2025). In contrast, SNM enables the study of interactions among entities to identify, visualize, and analyze relationships within a network (Bevc et al., 2011). These social networks include “functional entities (roles) and the way in which entities are connected” (McCurdie et al., 2018), and SNA includes measures such as “the number of links each individual has” and network-level measures like density (Valente et al., 2015). We decided to use SNM over GIS because it supports whole-network analysis and visualization of heterogeneous actors across institutional and geographic boundaries. This is an approach well suited to rural healthcare contexts, where coordination often depends on informal relationships, improvised communication pathways, and legacy infrastructures rather than centralized systems.
Valente et al. describe four stages for developing and using SMNs: (1) exploration or needs assessment, (2) adoption or program design, (3) program implementation, and (4) sustainment and monitoring. Because our study focused on needs assessment, we completed Stage 1 of this four-stage process. Here were the steps in our methodology:
Step 1: Assess Community Needs, Priorities, and Readiness
In our ongoing larger study (Johnson-Sheehan et al., 2026), we conducted surveys and semistructured video interviews with rural healthcare providers to assess community healthcare needs, shared priorities, readiness for change, and local capacities. We used this data to document perceived constraints, coordination challenges, and opportunities for improving communication practices. We grounded subsequent network mapping in practitioners’ lived experiences and local understandings of healthcare.
Step 2: Define the Study Area and Network Boundaries
We used county-level boundaries to establish a recognizable framework for data collection and visualization. Our research area included the rural counties surrounding Tippecanoe County in northcentral Indiana (Benton, White, Carroll, Clinton, Montgomery, Fountain, and Warren). The Greater Lafayette Area in Tippecanoe County was defined as an urban hub, where larger and more advanced healthcare facilities are available. We treated county borders as convenient analytic boundaries rather than fixed limits, recognizing that rural healthcare communication and referral pathways routinely extend beyond county lines. Accordingly, we conceptualized the network as a whole component that includes all identifiable healthcare-related entities operating within and across the target region.
Step 3: Identify Unit Types, Network Layers, and Key Actors
We classified healthcare facilities into categories, which included physician offices, clinics and hospitals, dental offices, pharmacies, mental health providers, assisted living facilities, emergency medical services (EMS) and ambulance services, libraries, and university extension offices. Within these categories, we identified key organizational actors involved in care delivery, coordination, and information exchange.
Step 4: Collect and Geocode Network Data
We compiled facility data from public sources such as state health departments, federal registries, and regional directories, and we cross-referenced these data with our interview findings to improve accuracy. We also used ChatGPT 5.0 to locate facilities that were not identifiable in government sources or regional directories. We geocoded facility locations, using Google Maps to generate latitude and longitude coordinates.
Step 5: Examine Relationships, Communication Pathways, and Gaps
We analyzed relationships within and across overlapping professional and institutional networks to document referral pathways, information-sharing practices, and coordination mechanisms. We identified points of communication breakdown and gaps in coverage caused by behavioral, organizational, technological, or ecological barriers. We treated connections as contingent and situational rather than permanent and continuous.
Step 6: Develop and Analyze Network Maps
We used our network maps to identify nodes, connections, and geographic factors. We studied network connections among facilities, transportation routes, broadband availability, and cellular coverage to contextualize how physical and digital infrastructure constrain or enable care coordination.
Methodological Limitations
A few methodological limitations should be acknowledged. First, our network maps offer only snapshots of this one rural healthcare assemblage. All assemblages are unique, and they are continually being reconfigured through workforce turnover, changing referral practices, evolving technologies, and shifting institutional affiliations. Second, connections among nodes were inferred from documented relationships, geographic proximity, and observable linkages rather than directly observed. Third, we acknowledge that no rural healthcare facility, even the most remote, is functioning in isolation. Informal coordinating among these rural facilities can and does happen over the phone, e-mail, texting, and videoconferencing, as needed. Finally, we recognize that the boundaries of our study area are porous, meaning that patients, healthcare providers, and communications will travel outside the study area and communicate with people and institutions outside of our study's boundaries. For example, patients regularly drive to hospitals in Indianapolis or Chicago for advanced treatments, when needed. In special cases, they also drive or fly to visit specialized hospitals such as the Mayo Clinic or the Cleveland Clinic.
Social Network Maps
The results of our data collection and visualizations allowed us to develop a set of eight SNMs that illustrated the layers of the assemblage. These maps were created by inserting icons that represent facilities and organizations. Then, lines are drawn among these icons to show connections and relationships. The icons differ in size and color, which demonstrate the individual or organization's role in the specific network. If icons are clustered together, they can be classified as a “node” or “community” (McCurdie et al., 2018). The Greater Lafayette area, the urban county in the center of the region, was classified as a hub that offers specialized and emergency care. This hub does not control most of the rural facilities, aside from three branch hospitals in rural towns; however, the rural facilities do rely on the hub for anything above basic or urgent care.
Due to space limitations, we cannot publish all eight of our maps, so we have included six maps here that best illustrate the relationships among a select group of medical and healthcare facilities. These maps include physicians’ offices, hospitals and health clinics, pharmacies, mental health facilities, EMS and ambulance services, and libraries. We have placed the full set of our maps online at https://drive.google.com/drive/folders/1O6VmeohGpjoxp2RezYVs1Em2wo7xOPC2?usp=sharing. Upon request, we can supply a password-protected Excel file that includes these facilities geocoded locations. These maps and locations will evolve over time, and we plan to update these maps and data every five years to create a longitudinal study.
Map 1: Independent Primary Care Provider Offices
In Figure 1, our map of independent physician offices illustrates a key structural weakness in rural healthcare networks: low node density and minimal horizontal connectivity. Most counties in the research area have two or fewer physician offices where patients can access a primary care provider. These offices mostly function as solitary nodes rather than as part of a coordinated or formally integrated network. Three counties (Warren, Carroll, and Clinton) contained no physician offices at all, creating clear gaps in access to local primary care. We also found it noteworthy that no independent physician offices are located in the rural areas of the Tippecanoe County, even though several smaller towns in the county could likely support offices. Instead, primary care in our research area is highly centralized within the Greater Lafayette metropolitan area, which contains numerous physician offices, most of which are affiliated with one of three large healthcare networks: IU Health Arnett, Franciscan Health, and Unity Healthcare. Because the estimated number of principal care providers in the Lafayette/West Lafayette area is approximately 200, we chose not to represent them in the map to avoid overwhelming the visualization and obscuring the contrast between dense, centralized networks and sparsely connected rural areas.
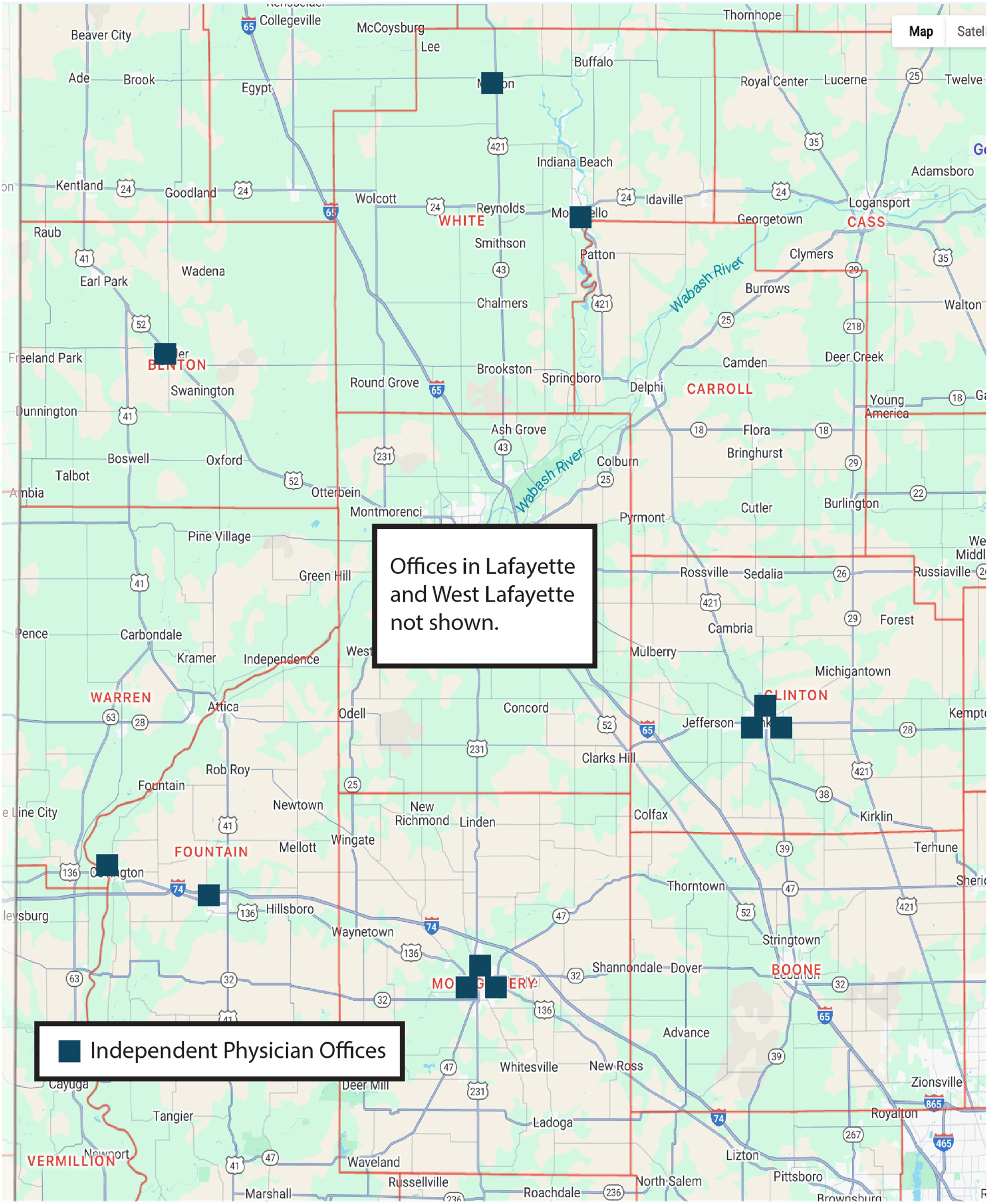
Independent primary care provider offices.
Map 2: Rural Hospitals and Clinics
Figure 2 maps all hospitals and clinics in the region and highlights the role these facilities play as anchoring nodes within otherwise sparse rural healthcare networks. Even in the larger towns outside of Tippecanoe County, hospital services are limited. The IU Health hospitals in Monticello and Frankfort are designated as critical access hospitals with only 25 inpatient beds each, and Franciscan Health Crawfordsville in Montgomery County has 103 inpatient beds. While these hospitals offer a full range of basic services (emergency care, surgery, maternity, labs, and rehabilitation), patients who require specialized treatment or higher levels of care are regularly transferred by ambulance or helicopter to hospitals in Lafayette or Indianapolis. In time-sensitive emergencies, obstetric transfers, and multisystem trauma cases, patients are often airlifted directly to Indianapolis hospitals.
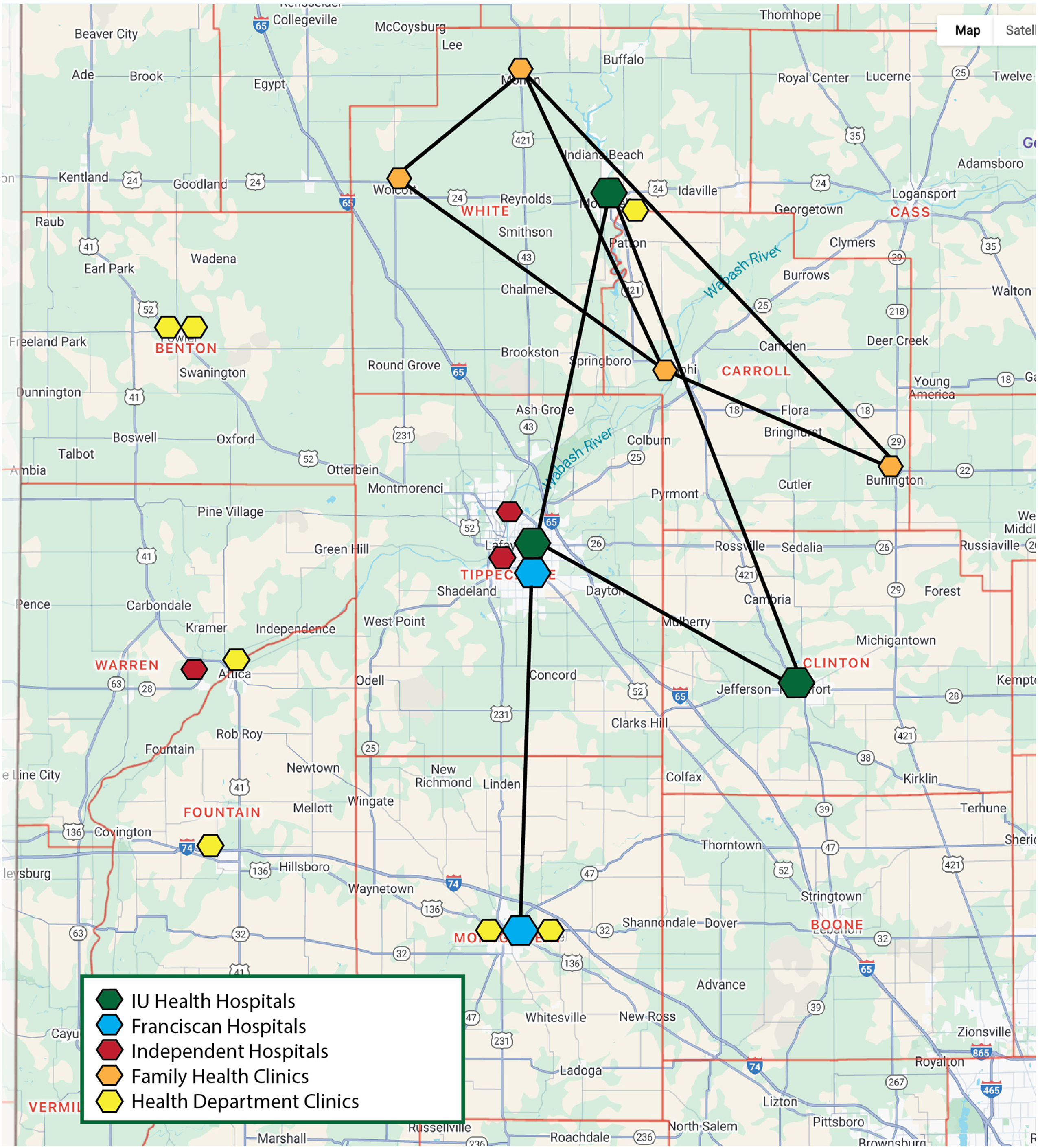
Rural hospital and health clinics.
A few rural hospitals in our research area are vertically integrated into larger healthcare systems centered in Tippecanoe County, including IU Health Arnett, Franciscan Health, and Unity Healthcare, while a couple of rural hospitals operate as independent nodes with fewer formal linkages. A small number of clinics are similarly affiliated within larger networks, but most are either part of the Family Health Clinic network in White and Carroll Counties or function independently. Staffing patterns further reinforce network centralization. Our surveys and interviews show that physicians working in rural hospitals and clinics tend to commute from Lafayette or West Lafayette, creating daily flows of professional expertise into rural sites rather than positioning physicians in the communities themselves. Some nurses reported living in the communities where they work or in nearby towns, positioning them as more locally anchored actors within these networks.
Map 3: Pharmacies
In Figure 3, we debated whether to include pharmacies located in the Lafayette/West Lafayette urban area in our map, as their number visually overwhelms the handful of pharmacies in the surrounding rural counties. We ultimately decided not to include the urban pharmacies, even though the map illustrated the highly centralized and corporate nature of pharmaceutical distribution networks in the region. Most stand-alone pharmacies in the eight-county area are affiliated with national chains, primarily Walgreens and CVS, creating a network characterized by strong brand-based integration and limited local ownership. Only a few of the region's smaller towns maintain an independent pharmacy. Several medium-sized towns (including Monticello, Frankfort, Crawfordsville, and Attica) have a Walgreens and/or CVS, reinforcing the role of these chains as dominant nodes controlling access to medications and supplies. In a few cases, clinics have established in-house pharmacies, effectively creating tighter coupling between prescribing and dispensing functions. Most rural hospitals had one or more pharmacies located nearby, often within a few blocks, adding to the density of healthcare services. Nevertheless, three counties in our research area were served by only a single pharmacy, representing potential points of vulnerability in the network.
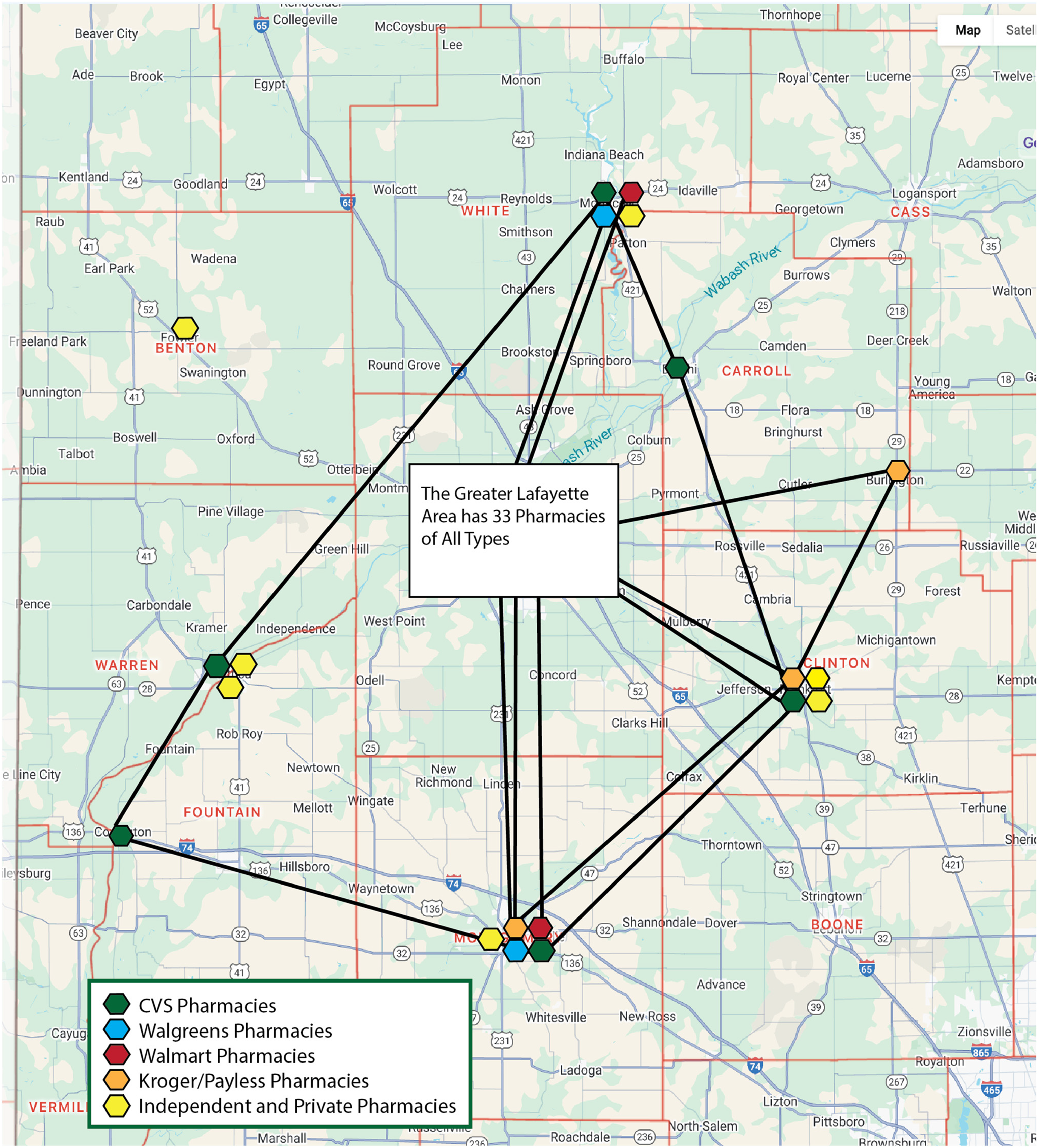
Pharmacies.
Map 4: Mental Health Facilities
Figure 4 represents the mental health facilities available across the rural portions of the research region and reveals a markedly different network topology than primary or acute care. Notably, there are no mental health facilities located outside the Lafayette/West Lafayette urban area within Tippecanoe County, indicating an absence of rural nodes for mental health services within the county itself. In the counties surrounding Tippecanoe, we identified eight mental health facilities that serve individuals with substance use disorders, inpatient mental health needs, and outpatient counseling and therapy needs. Five of these facilities are affiliated with the Valley Oaks Health network, forming a relatively cohesive regional subsystem. Valley Oaks also maintains multiple sites within Lafayette and West Lafayette. The remaining three facilities are operated by independent nonprofit organizations: Community Howard Regional Health, 4C Health, and Cummins Behavioral Health Systems. Community Howard and 4C Health is networked with facilities in regional or statewide networks. Cummins is wholly independent.
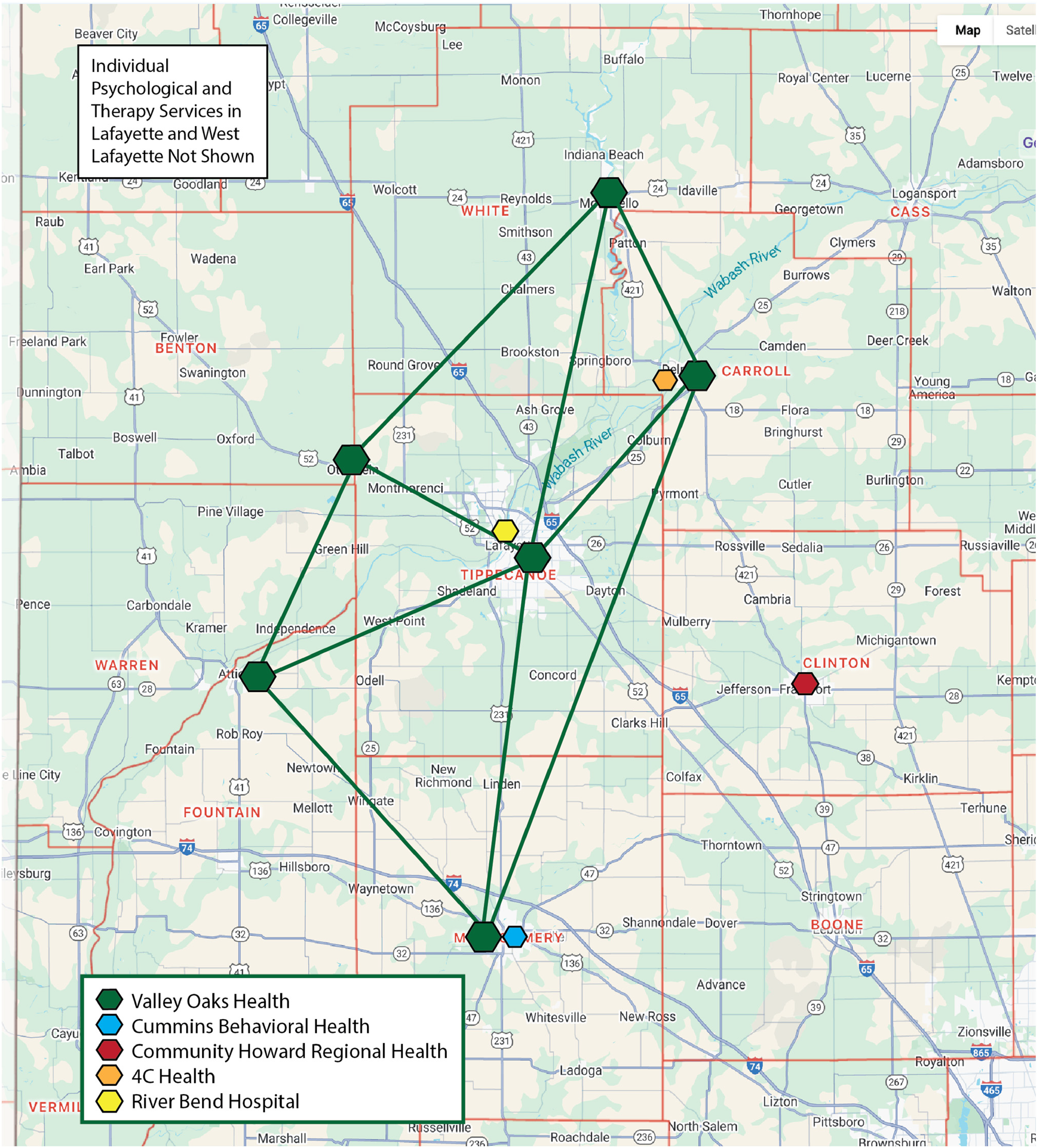
Mental health facilities.
Map 5: EMSs and Ambulance Services
Our map of EMS and ambulance services located in rural areas, shown in Figure 5, was especially telling. Most of the counties outside of Tippecanoe County had 1–3 EMS and ambulance services. These services were usually located in the middle of the county, often in the county seat. Counties in Indiana tend to be about 19–22 square miles. This means the response times from the county seat to the edge of the county range from 25 to 40 min. Then, depending on a patient's issue, transporting the patient to a hospital could range from minutes (by helicopter) to an hour (by ambulance). Most EMS units in our research area are government services, with a couple being volunteer services. Only two private ambulance services are located outside the Greater Lafayette urban area.
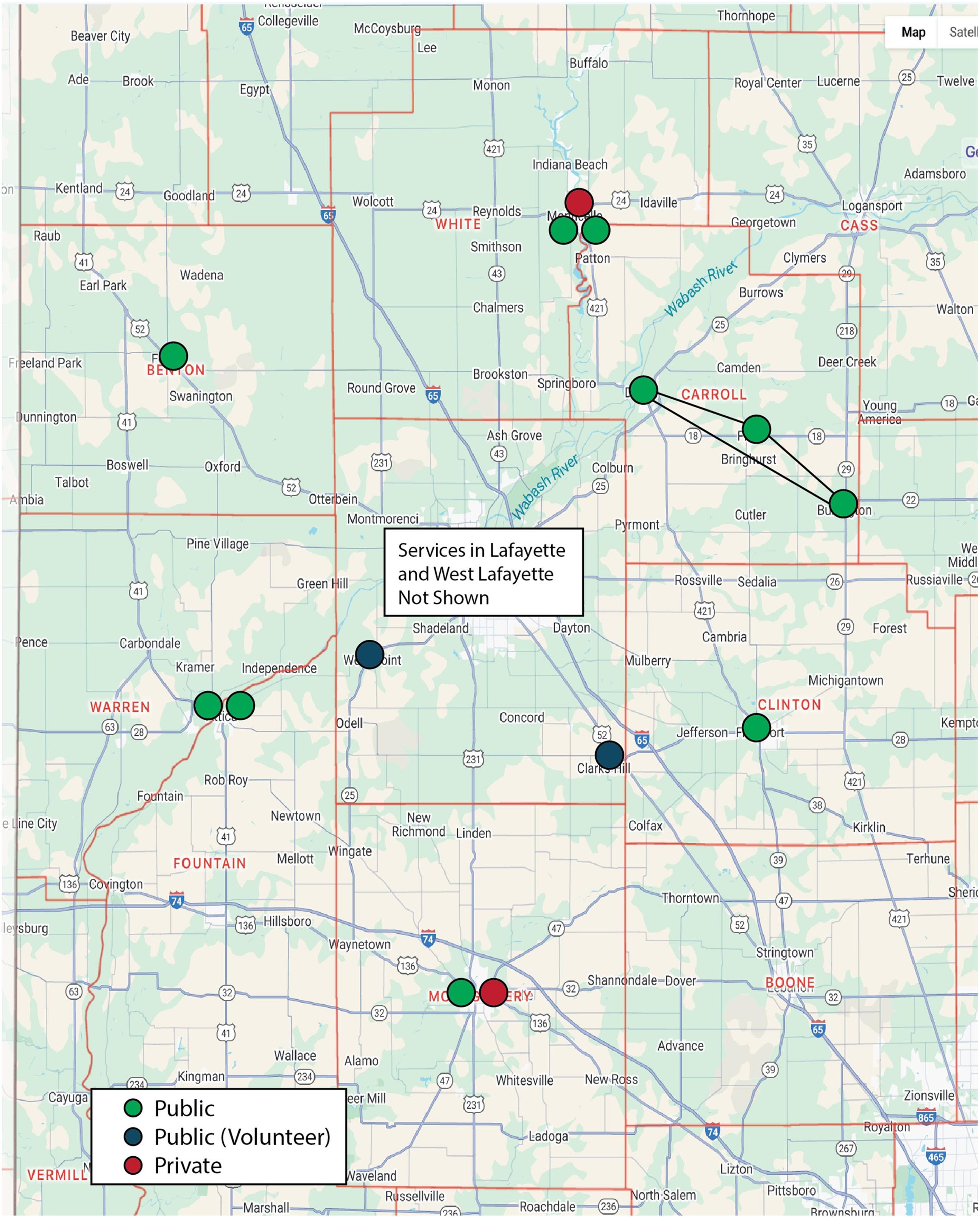
Emergency medical services and ambulance services.
Map 6: Libraries
As shown in Figure 5, Libraries may seem like an unconventional inclusion alongside hospitals and clinics, yet prior research indicates that libraries increasingly function as key intermediary nodes within rural healthcare communication networks. For many rural residents, libraries serve as accessible entry points for health-related information, particularly in communities with few or no healthcare facilities. Libraries also provide reliable internet access, enabling residents to participate in telehealth consultations and connect with geographically distant providers. Published studies and our interviews suggest that librarians increasingly view themselves as frontline healthcare information providers (Asikin-Garmager et al., 2025; Genova & LaPreze, 2024). Librarians regularly respond to health-related questions at service desks, directing patrons to print and digital healthcare resources. They also frequently assist individuals in navigating internet connections to regional hospitals, clinics, and national online teletherapy platforms, such as Better Help. In this sense, libraries form the connective tissue that helps bridge gaps between rural residents and healthcare networks (Figure 6).
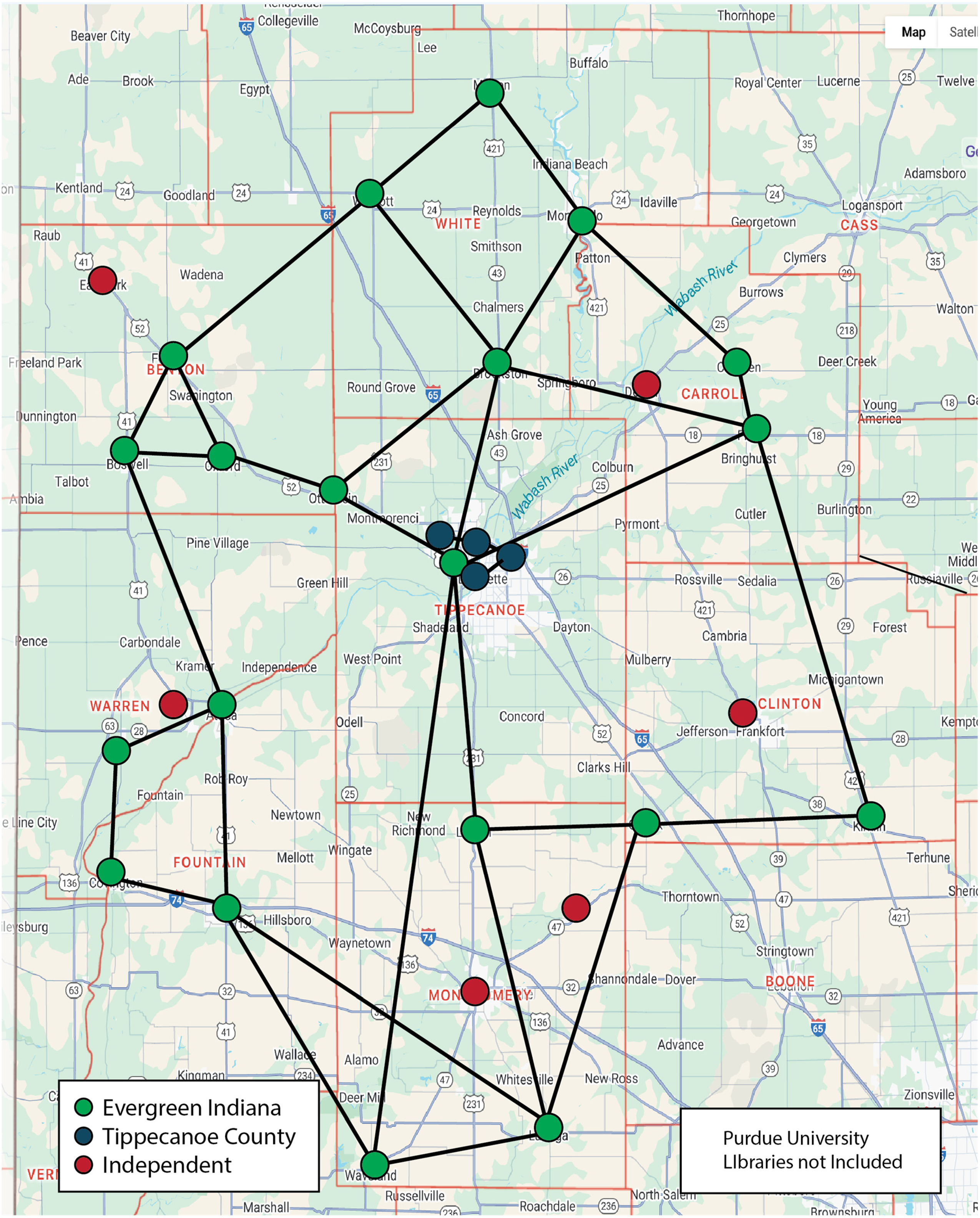
Libraries.
Results
Initially, we intended to create a master social network map that included all eight layers of the maps that we made. Unfortunately, the resulting map with all its elements and intersecting lines was unreadable and, frankly, confusing. That said, our separate maps demonstrate that key facilities in rural medical and healthcare networks tend to cluster in the same areas. Not surprisingly, these facilities are usually found in the largest town in each county, usually the county seat. In other words, physicians’ offices, clinics and hospitals, pharmacies, EMS and ambulance services, and dental offices tend to be located in clusters near each other in larger towns. Mental health services and assisted living/hospice care are sometimes located outside these larger towns. Libraries are more dispersed throughout counties because they are located in both smaller and larger towns. They could be found near medical and healthcare services, but they also appeared in towns that had no healthcare facilities. Based on our surveys, interviews, and SNM, these are the major results that emerged from our mapping:
Healthcare Facilities and Services are Unevenly Distributed Among Rural Counties
The maps reveal significant differences in the density of healthcare infrastructure across the region. Healthcare facilities and services tend to cluster in a limited number of towns or counties, creating localized nodes (i.e., subsets of the network in which entities are internally connected but only weakly linked to other areas). Significantly, most rural towns contain few or no facilities, representing low-density zones where patients are forced to travel significant distances to access in-person care. Our maps can be used to identify service voids where access barriers are most pronounced.
Nodes Exist in Larger Towns, but They Seem Structurally Fragile
Our mapping shows that some towns function as centralized nodes, meaning a disproportionate number of connections converge on a small number of facilities. Also, these nodes act as points of convergence across multiple maps. For example, rural hospitals are often colocated with clinics, pharmacies, and assisted living services. This pattern of network centralization increases systemic vulnerability. When a large share of the healthcare facilities and services are concentrated in a few locations, disruptions at one healthcare facility, such as the closing of a rural hospital, will significantly impact on surrounding components and increase travel burdens for patients.
Patients who Require Specialized Services Travel Long Distances
Comparing facility layers reveals limited transitivity among related services, which means patients often need to travel farther for comprehensive care. As a result, patients and caregivers end up responsible for connecting various healthcare providers within the assemblage. For example, a patient's primary care physician may be located in the urban hub, but the patient needs to travel to another county to get medications, and the patient then needs to travel to a rural hospital for dialysis. This lack of transitivity can contribute to problems with continuity of care. Referral flows also exhibit low reciprocity, as care frequently moves in one direction, from rural sites to urban hubs, without equivalent return linkages.
Informal and Relational Nodes Maintain Connectivity
The assemblage maintains connectivity through informal relationships and improvised communication pathways. These informal ties can act as bridging connections that connect healthcare providers and patients with otherwise weakly linked elements. Cross-county collaborations, informal referrals, and interpersonal communication among providers can function as pathways that hold healthcare in rural areas together despite the lack of a formal overall infrastructure.
Nonclinical Facilities, Such as Libraries, Serve as Boundary-Spanning Nodes
Mapping libraries and university extension offices alongside healthcare facilities reveals that nonclinical institutions often occupy important positions within underserved areas. These sites can function as communication nodes, linking components and increasing local connectivity. Their role highlights how healthcare communication infrastructure extends beyond formal medical settings.
Technological Advancements Represent Potential Network Improvements
Layering maps allows researchers to identify facilities and locations that occupy key positions within multiple layers of the network. These high-leverage nodes include hubs, multiservice facilities like clinics, and nonclinical institutions like libraries. From an SNM perspective, interventions such as telehealth, mobile clinics, AI-enhanced EHRs, and AI-enabled coordination tools could provide opportunities for increasing network density, improving transitivity, and reducing overreliance on highly centralized nodes. These emerging technologies, especially AI, may be a way to strengthen connectivity without requiring expansion of physical infrastructure.
Discussion
Taken together, the results show that rural healthcare in this region operates as a low-density, highly centralized, and somewhat fragile assemblage. Outside of urban areas, healthcare tends to be concentrated in a small number of towns where services have formed into loosely connected nodes. Meanwhile, many patients remain dependent on care delivered across long distances. As a result, healthcare in these rural areas can be viewed as both resilient and fragile at the same time.
Resilience across the assemblage is created by informal referrals, personal relationships, and improvised communication pathways. These informal practices act as territorializing forces within the assemblage, partially compensating for the sparse infrastructure. Nonclinical institutions such as libraries and university extension offices are able to serve as nodes, providing accessible sites for meeting with healthcare providers through telehealth networks. That said, rising financial pressures and provider shortages contribute to the deterritorialization of the assemblage, increasing travel distances and fraying local connections. As the assemblage stretches and thins out, the humans in the assemblage (providers, EMS units, patients, and caregivers) must expend more time and resources to provide/receive treatment and maintain continuity of care.
The maps also identify potential places for interventions where the assemblage could be stabilized or even strengthened. Emerging technologies such as telehealth, AI-enhanced EHRs, mobile clinics, and AI-enhanced communication tools cannot be full replacements for local, hands-on care, but they may be able to increase density in the network, strengthen transitivity, and support reciprocity across elements that are increasingly distant physically from each other. Strategic interventions could better distribute resources and time to hold the assemblage together.
Ultimately, when viewed through a combination of SNM and assemblage theory, the rural healthcare assemblage in our research area is not a failing system but rather an evolving and thinning assemblage that is continuously changing to address medical and healthcare shortages. Effective interventions, especially with emerging technologies, may be able to strengthen nodes, improve connectivity among those nodes, and take advantage of the informal communication practices that already exist.
Conclusion
At this point, we are not able to offer specific intervention recommendations for rural healthcare assemblages like the one we studied. Our data show that emerging technologies such as telehealth, EHRs, and AI are extending the reach of rural healthcare networks, but care in rural areas remains fundamentally constrained by material realities. Many healthcare necessities, such as physical exams, laboratory testing, vaccinations, dialysis, injury treatment, and emergency transport, need to happen in person at physical facilities. Emerging technologies cannot replace these physical aspects of medical practice.
A central takeaway from this study is that SNM, in concert with assemblage theory, can help identify coverage gaps, fragile nodes, and strained referral pathways. It may also reveal where emerging technologies can level up providers and patients. At the same time, these methods make visible the limits of these technological solutions. Rural healthcare networks depend on physical facilities, human labor, and proximity, all of which are under increasing strain from financial pressures and government policy shifts.
Our SNMs illuminate the healthcare disparities in this region of northcentral Indiana. Many rural patients lack convenient access to hospitals, clinics, pharmacies, or mental health providers. Even in counties with healthcare facilities, services tend to be concentrated in a single larger town. Meanwhile, pharmacies, specialists, and mental health providers cluster in urban centers such as Lafayette and West Lafayette, requiring rural residents to travel long distances for care.
Our maps also identify rural libraries and university extension offices as important healthcare-adjacent services. Many rural towns maintain libraries that offer free internet access and a safe public space to discuss healthcare issues. This positions libraries and extension offices as potential nodes for telehealth and healthcare communication. Further research should examine the role librarians already play in supporting health information and virtual care access.
Finally, SNM supports our project's broader research into using AI and machine learning to enhance and streamline communication practices in rural healthcare. Our maps illuminate healthcare deserts, potential referral bottlenecks, and communication gaps. These are situations in which AI and machine learning tools may have meaningful impacts. Social network mapping can reveal how communications actually flow within rural healthcare assemblages, especially when maps are being updated longitudinally over time. In the future, this may enable the development of scalable and ethically responsive solutions using emerging technologies.
IRB Approval
Purdue IRB-2024-215
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Project funded by a grant from North Central Regional Center for Rural Development (NCRCRD) and a Breakthrough Award from the John Martinson Honors College at Purdue.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
8 maps will be available online, as well as an Excel file with location coordinates used to create the maps.