
Abstract
Assisted Reproductive Technologies (ARTs) in India intersect with issues of gender, technology, kinship, commerce and politics and therefore have generated considerable public, ethical and academic debate. Sociologists play a significant role in understanding ways in which this technologically-mediated reproduction has been variously interpreted in these debates; whether it represents progress, promise or pressure. The article demonstrates how diverse cultural settings mediate the experiences of those engaging with ART, both as ‘users’ and ‘providers’. In India, ART involves the reconfiguration of individual, familial and social identities: for instance, when the agony of a childless woman gets negotiated through this ‘hope technology’. We look at the development of ART practices and how they encounter its seekers at the local level. The study also looks at ways in which infertile women deal with ART and use it to achieve, potentially, an ‘identity’. The study, focusing on diverse geographic locations in Odisha, is based on theoretical insights gained from extensive field research comprising interviews with users and providers covering a period from 2011–2014.
Context
Hitherto, modern medicine was restricted to preventing and treating disease. However, now it is possible to assist in a human’s creation. So, human beings are now entering into a new era as a result of advances in medicine particularly in the field of human reproduction. It evolved from traditional methods in medical science to rapid technological developments during the late 19th and early 20th centuries. The technology evolved ranged from manual techniques to Caesarean sections and amniocentesis which came with advances in the life sciences. By the middle of the 20th century’s decline in mortality rates, maternal mortality no longer remained the only concern; rather technology was developed in the West to assist in the creation of humans through artificial insemination (AI) 1 and in vitro fertilisation (IVF). 2 Gradually, technology travelled across the developing countries: the impact of technology on such countries was immense, not to mention the patriarchal push for natalism. Edwards first described the technique of IVF and the subsequent birth of Louise Brown in Britain during 1978.
Biological reproduction getting mediated through reproductive technologies is the result of global influences. Certain aspects of globalisation, such as the compression of spaces, convergences, advances in life sciences and market forces (Appadurai, 1996; Hannerz, 1992; Howes, 1996) are significant for the spread of reproductive technologies, particularly assisted reproductive technologies (ARTs). 3 But the aspect of globalisation we are emphasising here is what Donna Dickenson (2005, p. 43) presents as, ‘the process by which capitalism penetrates global markets and audiences with minimal regulation’. Because reproduction in the context of ART is the production in an industrial sense having a capitalist motive. Just as multinational corporations (MNCs) have found it profitable to expand their production to developing countries, both to capitalise on cheap labour power and minimal regulation, so has the ART 4 industry found new markets in these countries. Therefore, reproduction has been denationalised and available to the emerging markets of developing countries.
As Inhorn (2002, p. 280) puts it, the examination of these Western technologies in non-Western locations offers an illuminating case study of local–global intersections and particularly the importance of interrogating what is ‘local’ in an increasingly ‘global’ world. In India, individual doctors 5 , with training in the field of ART at internationally reputed centres, came forward with entrepreneurial objectives and established infertility treatment clinics during post-1990s 6 . Users/seekers also are increasingly well informed about the new developments and applications of ART and demand them from treatment-providers. ART in India is further fuelled by India’s fast-paced economic growth and liberalisation, an ideal convergence of demand/need-supply in a globalised market place. The Indian Council of Medical Research (ICMR) estimates that as of December 2016, there are 385 ART clinics enrolled under the National Registry of ART Clinics and Banks in India (NRACBI). 7
Though a delay is acceptable in the timing of one’s marriage, subsequent childbearing and in the number of children but the normative social biography of an Indian woman ultimately rests on marriage and reproduction. Given this ‘mandate’ of motherhood then, how do married women retain their identities when they find themselves infertile? The article examines the cosmology of infertile women, and how their self-identity is seen through the politics of gender against the backdrop of the existence of new technological options. This piece of research contributes to comparative studies of gender and family, and by inviting women’s voices into the infertility discourse; it provides insights for area studies (for example, Global Studies) and Development Studies as well.
Motherhood Mandate 8
The ideology of motherhood and the stigma of childlessness are deeply rooted in Indian culture as in many other cultures around the world as manifested by numerous ethnographies on the subject (Becker, 2000; Ginsburg & Rapp, 1995; Inhorn & van Balen, 2002). Post-marriage mandates childbearing for an Indian woman. Bearing and rearing children are central to a woman’s power and wellbeing, and reproduction brings in its stead concrete benefits over one’s life. For families with significant property or wealth, sexual reproduction allows for social reproduction—the orderly transfer of privilege through inheritance to the next generation of kin. In India, a married woman’s identity is defined through motherhood and it is by becoming a mother (particularly of a son) that she secures her status within her marital family and her association to her husband’s kin. The notion of motherhood, in other words, serves as a critical cultural class—which are masked by psychological or emotional discourses. Some serious research studies (Dube, 1986; Jeffrey, Jeffrey, & Lyon, 1989; Uberoi, 1993; Stones & James, 1995) inform us that Indian women are quite conscious that their reproductive capacities are an important source of power, especially when they lack it from other sources.
Social change in postcolonial India has reconfigured family forms, size and patterns. Changing household structures, in turn, are influenced by ideas about marriage including gender relations and continuing obligations to one’s natal kin. The country has witnessed a decline in the total fertility rate (TFR) over the past three decades, for example, the TFR has declined by roughly 1.5 per cent per year from 6 per cent in 1966 to 3.6 per cent in 1992 (Visaria & Visaria, 1994); further to 1.7 per cent per year during 1992–2008, with TFR reaching 2.6 per cent births per woman by 2008 (Office of the Registrar General of India, 2009). The average household size has also declined over this period. Concurrently, there has been a sharp increase in the proportion of women entering the labour force. Family formation patterns are also changing. Within the neoliberal discourse of ‘choice’, women are positioned while choosing to ‘delay motherhood’, often for reasons related to their career. Hence, the age of mothers when they have their first child has risen as also the probability of having fewer children than previous generations: Some women also remain voluntarily childless.
Married women who remain childless in India are invisible in social science research, but they are highly visible in their families and communities. Traditionally, childlessness has been labelled as being ‘barren’, an act of God, a curse of the family fertility Gods (Neff, 1994); a field where seeds do not germinate (Dube, 2001); the interpretation of witchcraft as an explanation for misfortune (Evans-Pritchard, 1937); alakshmi (inauspicious) (Pattnaik, 2006); a sin, particularly a sexual sin, unfortunate and unbearably desolate (Patel, 1994). This has been further strengthened by the existence of ART. Beating childlessness through ART at infertility clinics in big cities like Delhi, Mumbai, Hyderabad (Joshi, 2008; SAMA, 2007; Widge, 2001) takes away the choice simply to accept infertility. The presence of ART can be projected as a greater desire to have children than existed before (Franklin, 1998).
Theoretical Insights
We may turn to a paradigm that has a common man’s knowledge of the world as its subject matter, namely the phenomenology of Erving Goffman. In the context of infertility, Goffman’s ideas about what he calls ‘stigma’ is of interest to us. In Goffman’s (1963) analysis, an infertile individual carries a discreditable attribute and is reduced in the eyes of others ‘from a whole and usual person to a tainted, discounted one’. The barren woman has always been frowned upon by every social group in terms of an object of ridicule, excluded from ceremonies and rituals, avoided, disallowed or looked upon with suspicion and considered dangerous as being ‘deviant’ (Miall, 1986) to the expected ‘norms of reproduction’. After a long somatophobia which left the notion of ‘body’ to the natural sciences, social theorists now discuss the implications of materiality for subjectivity and discourse (Grosz, 1994). There is no uniform framework for studying bodies yet (Hockey, 2009, pp. 477–478) as we see three overarching approaches within the realm of sociology health, gender and work are used most frequently: social constructivism, structuration theory and phenomenology. Social constructivism has latterly been heavily influenced by Foucault (1973), relying on positioning of the body within a power network. Alternatively, the structuration theory, advanced by Bourdieu (1977, 1984) and Giddens (1991), charts the body somewhere between social structure and human agency. Finally, a much smaller and emergent field of studies, phenomenology, led by theorists such as Merleau-Ponty (1962) and with which this article is primarily concerned, maps the experience of embodiment. The distinction between existence and being is essential to the thought of Merleau-Ponty and, in general, to phenomenology and existential psychology. In anthropological terms, it can be roughly translated as the distinction between intentional action and constituted culture.
Data and Methods
The analysis presented in this article is based on theoretical insights and empirical qualitative research comprising interviews 9 with treatment-seekers (infertile women) and treatment providers (fertility specialists and gynaecologists). Empirical evidences were gathered from the extensive fieldwork (2011–2014) conducted in the state of Odisha. The design of the research was essentially exploratory. A sample of 40 women was interviewed who attended ART treatment sites at Bhubaneswar, Cuttack, Bhadrak and Rourkela. The sample size is relatively small and geographically specific as the respondents were extremely resistant to efforts of the researcher(s) who interviewed them about infertility, an issue that was both intensely personal and sensitive. (For example, the initial attitude towards infertility was, ‘Don’t tell anyone’.) However, the results certainly present predicaments of infertility in many parts of India. The multi-sited field visits (Marcus, 1995) used relay sampling to get in touch with respondents, rapping networks of ART clinics, and those of intended ART users.
A heightened consideration and presentation of women’s experiences comes only through in the documentation of women’s voices. Family pressures graphically come through these voices. In the waiting rooms of treatment-providers, the researcher encountered several women/couples from different parts of Odisha who had travelled to avail themselves of infertility treatments which did not available in their own places. Each interview, lasting one to two hours, was conducted in a separate room within the clinic to maintain privacy of the respondents and to encourage them to talk freely. During interviews, the women were encouraged to offer extended accounts of their situations, including the reactions of others—their husbands, their husband’s family, their family and the neighbours. The conversational nature of interviews yielded lengthy accounts of meaning and action, and several women shared that they felt ‘relieved to be able to talk’.
The data gathered from the interviews were used as a primary dataset. The interviews were audio-recorded, and then transcribed to extract themes and content. To achieve this, the study used words/phrases/metaphors of the respondents to illustrate these themes. The metaphor of ‘travel’ (Clifford, 1997) conveys the efforts we made, and those our participants made, to converse across borders of class and culture. Secondary source of materials on infertility treatment used in this article are drawn from scholarly texts and media reports. The study adopted a medicalised definition of infertility (in terms of a failure to achieve a successful pregnancy after a year or more of regular, unprotected intercourse) rather than looking at women who were explicitly childless by choice. If being infertile denotes ‘intent to conceive’, one must recognise that there are various degrees of intent and that the line between fertile and infertile is not as sharp as is usually imagined. Therefore, the voluntary childless mother proved rather difficult to identify/locate in Odisha.
Findings and Analysis
Demographic and Socio-Economic Characteristics
The marital life of 40 women (ages ranging from 19–43 years) was between 3–12 years; for the majority (67.5 per cent) it was between three to four years of married life. In our sample, each woman had visited one to five clinics. With the number of married years increasing, the aspiration to have a child also increased: for example, only one clinic was visited per woman, aged between 19–23 years; this went up to three clinics per woman aged between 24–28 years and four clinics per woman aged between 29–33 years and four to six clinics per woman aged between 34–43 years. About 55 per cent women have been undergoing infertility treatments for the last three years, 30 per cent women since four years, and a little more than 10 per cent women for the last five years. Information about the type of family was gathered to understand the family dynamics in the context of infertility in case of a nuclear or joint family. 10 Eighty per cent infertile women live in joint families and the rest live in nuclear families. Responses include illiterates, high-school educated, graduates and post-graduates. The majority women accessing ART in the sample were graduates (30 per cent) and high-school educated (35 per cent). However, ART is accessed by seekers from diverse educational backgrounds.
Though the study was keen to include diverse religious denominations including Muslims, 11 seeking infertility treatment, the absence of data (from the health establishments/any governmental sources) relating to this information restricted its pursual. Hence, a single religious denomination (that is, Hindu) among the seekers interviewed should in no way be interpreted to mean, a lower incidence of infertility among Muslims and Christian communities, or poor access to treatment among these communities. Women with many castes were represented: Brahmins and Karanas (advantaged castes), Telis and Gudias (backward caste), Dhoba and Kewat (Scheduled Caste). The incomes of the treatment-seekers varied widely between ₹5,000 to ₹100,000 12 per month. Nearly 58 per cent were between ₹10,001 and ₹50,000 per month. Regarding their work status, responses included public sector employees (regular and contractual), non-governmental organisations and housewives.
Reflections on Private Healthcare and the ART Industry in Odisha
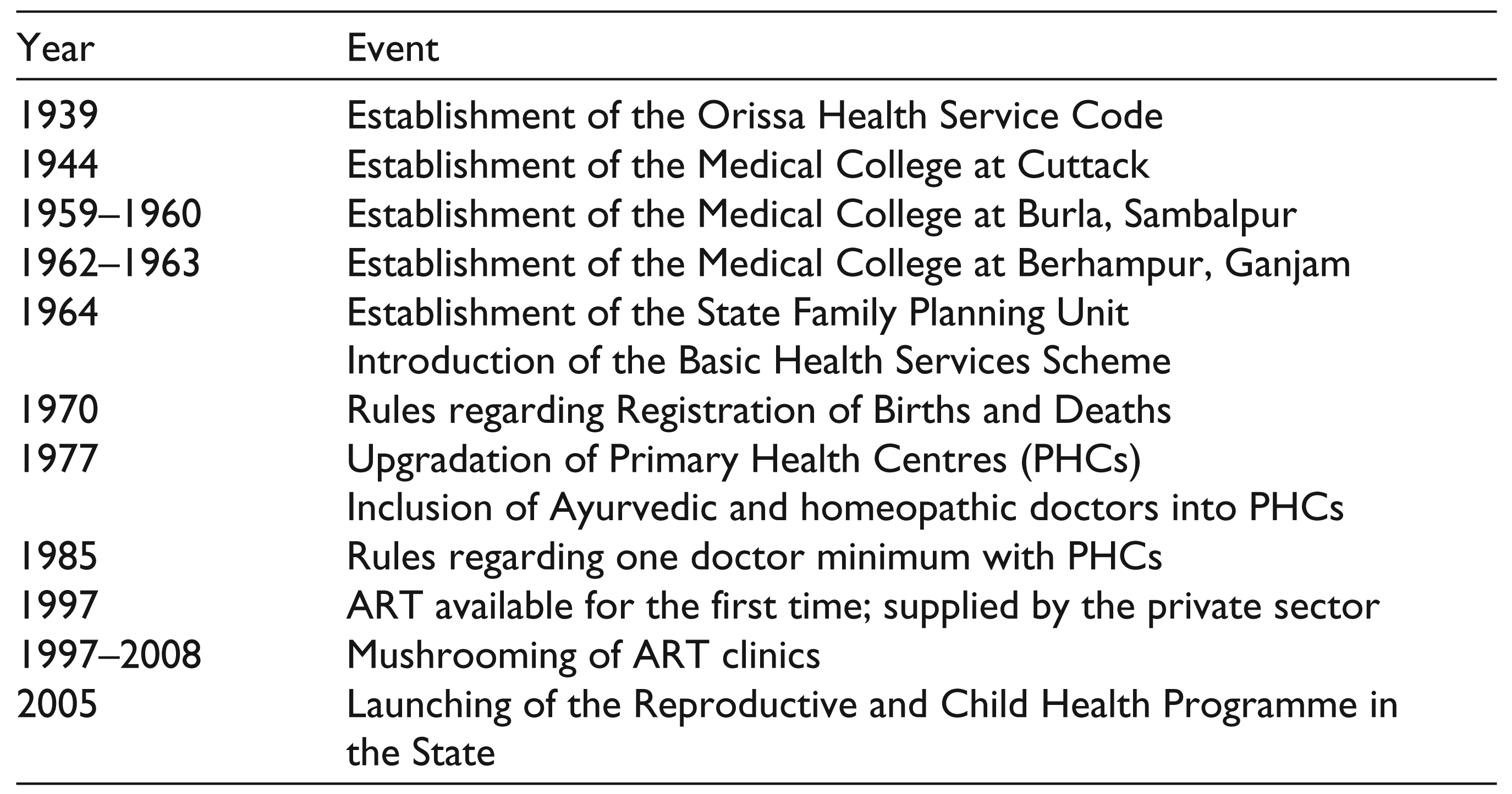
Odisha (Orissa) 13 was created as a state on 1 April 1936. The major landmarks in the development of health services in Odisha since its formation are highlighted in Table 1. Before proceeding further, let us see some basic statistics of Odisha. According to the 2011 Census, the literacy rate (72.87 per cent) of Odisha is a little lower than the national average (74 per cent). The literacy rate of women stands at 64.36 per cent, as compared to the national average of 65.46 per cent (GoI, 2011). The literacy rate among the rural population in Odisha stands at 70 per cent as compared to urban rate of 86 per cent. The male rural literacy rate is 80 per cent
whereas the female literacy rate in rural area is 61 per cent. The gender ratio (females per 1,000 males) of the state encouragingly stands at 978 in 2011 against the national ratio of 940. However, the urban gender ratio of Odisha remains lower at 934 as against the rural sex ratio of 988. The total decadal growth in 2011 is 14 per cent as compared to 16 per cent in the 2001 census. As per GoI, the infant mortality rate (IMR) of 65 is much higher as compared to the national average of 53. With a TFR of 2.2 per cent, infertility afflicts one-fifth of all couples in Odisha. In Odisha, the infertility figures (2.5 per cent) are above the national average of 2.3 per cent (Syamala, 2012). In Odisha, infertility may become a predicament eventually because the data shows a little above the national average which could be alarming 14 in the near future.
Landmark in the Development of Health Services in Odisha
The private health sector began offering infertility treatment services during the late 1990s. The growth of the private health sector in Odisha has been characterised by a heterogeneous structure consisting of institutions of varying sizes and patterns of ownership. The bulk of the private sector still consists of doctors (both trained and non-trained), who essentially provide primary level, outpatient care and are located in both rural and urban areas. The secondary level of care in the private sector is provided by nursing homes with a bed strength ranging from 5 to 50 and promoted by single owners or partners. The concept of a ‘nursing home’ is largely an urban phenomenon in Odisha. Most nursing homes offer generic and maternity services. Within this category, there is a further division between small and large nursing homes, which differ widely in terms of investments, equipment and facilities, range of services offered and quality of care. The tertiary level of care consists of multi-specialty hospitals that are promoted by capitalistic enterprises. These are mostly located in the cities of Odisha.
In 1998, there were just about a dozen private health centres providing infertility treatment services; in 2011, this increased to 50. 15 The private health centres, particularly the corporate medical sector, emerged to cater ART services in Odisha—this resulted from policy decisions taken at the national level. The proliferation of centres providing ART services in Odisha can be attributed to the formation of the Odisha chapter of the Indian Society for Assisted Reproduction (ISAR) in 2010 and a subsequent rise in the membership of ISAR. 16 Essentially, ART has gone from big cities to smaller cities to exploit the local market there.
Rationalisation 17 of ART
All women respondents rationalised ART as a benefit made available by scientific advances. A 32-year-old woman said, ‘has propelled us towards having a baby’. Women wanted to fulfil their wishes and to have at least a child in their families. For them, staying infertile implies receiving taunts from family members, neighbourhoods and being ostracised from various life-cycle events. ART offers a way out for infertile women. Infertile women rationalised ART by using the language of pro-choice feminism, saying that women should have the right to choose the treatment (IVF). About 15 per cent women in the sample asserted: ‘We [women] should have the right to go for anything [read technology] because it balances the [family and society] to get pregnant and produce a child within a few years after marriage’.
Respondents viewed ART as a status-enhancing tool for women in the study. In the West, ART has divided feminists, so that it is difficult to formulate effective common feminist strategies of resistance to medicalisation of women’s bodies and the adverse effects of ART (for example, the use of fertility drugs) on the health of women and their offspring.
As Becker (2000, p. 28) pointed out, technology can be seen both as a means to perpetuate cultural ideologies and to be used performatively by individuals as a vehicle for living out their goals. ART treatment-providers rationalised this through their consolidated views:
We tell them [infertile women] what we can offer and what we can’t. We, also say we cannot preform miracles. If we are lucky then they may hold their child soon enough but for that we have to go through numerous attempts, if necessary.
Treatment-providers know that some particular concept or cultural more will encourage every infertile woman who travels hundreds of kilometres in order to fulfill her desire for a child. However, the medical profession looks at ART as a ‘miracle cure’ that ‘treats’ infertility successfully. In this sense, the clinic soon develops a special relationship between different people and the new equation between treatment-providers and treatment-seekers comes into existence. A 28-year-old woman agreed: ‘[IVF] treatment can do miracles but we should trust it. Through trust a dependency is created. Women do what treatment-providers suggest and they happily listen to every instruction of the treatment-providers, undergoing tests and treatments’.
This brings about a dichotomy: on the one hand, couples trust the providers doing miracles for them, as a result they can conceive a child; on the other hand, modern medicine, 18 as a profession, is very concerned about misleading information being spread among the public. For most respondents, childbearing represents a major power base through which they negotiate the terms of their existence. Thus, not only is gender identity reaffirmed through the use of technology, but particular cultural dialogues about gender are also maintained and expanded. As we know, gender is a key organising principle of Indian society.
Resorting to ART
Resorting to ART was acknowledged by many respondents as not always their ‘choice’, but sometimes their ‘compulsion’ too. The women in the sample had arranged marriages. They are often threatened with desertion or forced to tolerate a husband’s second marriage while the husband may remain medically unexamined and unquestioned]. Surendra, a 30-year-old woman revealed:
Till now we have already spent ₹50,000. Still the pressures from the family have increased. We have already sold off our land for continuing the [ART] treatment. And, my husband’s second wife and the reason for his remarriage was childlessness from his first wife. I fear he will reject me, too.
First, women/couples are desperate enough to raise the money even if it means selling their valuable assets or borrowing money for infertility treatment. Second, historically not giving birth to a child has been attributed to a biological shortcoming of women only. Third, the decision to opt for ART was not straightforward for most respondents. They were pressed by family members to choose ART as a tool for increasing human fertility; procreation is determined, to large extent, by the family. Respondents learn about ART and their availability usually from others (for example, friends and close acquaintances) and by word of mouth. Fourth, improved means of communication technologies also played a role: success stories appearing on the internet, television and newspapers; mushrooming of advertising hoardings displaying ART treatment and the media publicity of successful cases achieved by infertility treatment clinics, are key sources of information.
About 17–20 per cent women feared that if the treatment did not succeed then their desire to get a child would be lost. The unsuccessful attempt does not lead to ‘pause’, but conversely to ‘action’. Usually women tend to continue the treatment while visiting one or the other clinic regardless of the high risks and uncertainties associated with the treatment as Saraswati, a 28-year-old housewife, for the last 10 years undergoing a series of injections and tests to hyperstimulate the ovary, says. In her own words: ‘The primary concern was pain and discomfort. Instead of understanding my situation my in-laws keep on taunting me. It’s been a constant worry for me’. Bridula, a 30-year-old female worker, in Government of India’s Integrated Child Development Services (ICDS) project, has been married for eight years, but admits frankly: ‘A child strengthens a wife’s often fragile bond with a spouse in a marriage and improves her status in the joint family and larger community’.
In fact, ART could be a ‘choice’ for some and ‘compulsion’ for others. Choice, for those who want a child, and compulsion, for those who have already undergone IVF procedures, but had no result. As a 33-year-old woman puts it: ‘If you were successful, you call it a ‘choice’, but if you weren’t, then you would say that one would have been better off without it as IVF treatments are very expensive and a painful process’.
Most treatment-seekers (70 per cent) are between 22 and 28 years. Increasingly, very young women (in their early twenties who do not want to wait too long to prove their fertility and fear rejection by their husbands and in-laws in case they fail to reproduce) and older women 35 or above, (ten per cent) are going to infertility treatment clinics, as revealed during interviews with both seekers and providers. Women who are 35 years or above, missed out on these treatments when they were younger, or because they did not know about them. At that point of time, ART was an alien concept. Gradually, people started talking about it. While some village women often do not know their true age, some older women try to conceal their true age. According to treatment-providers, women sometimes do not reveal their true age because they know that treatment providers often display a reluctant attitude in helping older women to avoid medical and social complications. Treatment-providers argue that women attempt to deal with these predicaments through a technological ‘fix’. They often try to dissuade such women, who are often very adamant about going through IVF procedures. The treatment-providers also hesitate partly because it brings down their success rates. Therefore, it has not been easy to see choice and compulsion working exclusively in Odia society rather they are overlapping, often simultaneously, by seekers to achieve their desire for a child.
Stigmatised Identity
The epidemiology of infertility within Odisha itself is different. Cultural factors account for the fact that Odia women are investigated completely before one can think of a simple basic investigations of their male partners. Among males fertility is often implied with potency and there is a deep sense of ‘shame’ felt by [Odia] men once investigations ascertain that the problem lies with them. The issue of male infertility, in most cases is swept under the carpet in Odia families as it is still considered a ‘taboo’ and brings disrepute to the man. Men, for whom it is the matter of virility and masculinity, decline to accept their condition and thus do not seek therapies. So, men can be responsible for infertility. However, as fertility manifests itself within a woman’s body, women undergo much of the accusation and social stigma of childlessness, even when the problem lies with the male partner.
In stratified societies, shared deviant identity, may constitute the basis of stigmatised social categories whose members are denied full realisation of their humanity through segregation, derogation, and disadvantage, including impaired access to valued goods, services and opportunities. Such despised or disvalued characteristics are the bases for categorical relegation of persons to some kind of lower status (Goffman, 1963). Such characteristics therefore constitute criteria for an institutionalisation of inequality in the sociological sense, as infertile women in Odisha who, if not concealed by the families, are often relegated, irrespective of their natal castes, to a caste-like lower status where they can consort freely only with another infertile woman.
Writers like Fakir Mohan Senapati (1902 [2006]) and Kanhu Charan Mohanty (1955) described infertile identities in a ‘spoiled fashion’ for the first time in Odia society through their novels that not being fertile was socially unacceptable and a completing female gender role (emphasis added). Damayanti, a 35-year-old woman from a lower-middle class stratum said:
… there was no family pressure as such after six years of my marriage, yet I feel the guilt for not being able to conceive because it’s very difficult to defend the position before others while saying the choice is to remain childfree. But, such a thing is quite uncommon here [Odisha]; it may be possible in foreign countries. Here society won’t let you feel like a complete woman if you don’t have a child.
Damayanti’s illustrative evidence shows that how society paints childbearing as the essential role of a particular gender. One reason for this may be that a woman becomes a full member of the family in which she is married only after the birth of a child by whose name she is addressed. A more theoretical rendering of the idea could be found in Goffman’s (1963) words: ‘ …a spoiled identity can occur when a discrepancy exists between an individual’s actual identity and an ideal, or what he calls as “virtual identity”…’
Women of an appropriate age without children are constantly asked: when will you have a ‘little one’? ‘When is the good news?’ ‘Can we see the baby bump this year, please’. Kanakalata, a 30-year-old housewife explains: ‘Without children staying in a village appears to be difficult and every morning I prepare myself to face enquiries from neighbours, particularly old women’.
A stigmatised status may entail segregation into enclaves, or banishment to other forms of shared social isolation. Respondents had suffered from ‘social isolation’ in terms of not being welcome at marriages, birth ceremonies and family rituals. They confirmed that childlessness denied them ‘complete membership’ to large kin-group (biradari, khandaan, a clan). They expressed that it is the woman who was often viewed as the ‘guilty party’ as Pinky Virani (2016) puts it, women live through the trauma of ‘infertility’ – cruelly attributed as their fault’ – to undergo the tribulations of ART.
Jasdeep, a 24-year-old woman, a postgraduate degree holder from Rourkela, an industrial region of Odisha admitted: ‘[The] pressure is built within us; I was equally anxious and felt awkward at social gatherings especially when people inquired about whether there was any ‘good news’. I felt ‘crushed’ being reminded of my childlessness.
Infertile women were concerned about confidentiality about their treatment: about 40 per cent women attempted to hide their infertility and its treatment from immediate family members as well as friends. However, the high cost of ART treatment may require women/couple to borrow money from family thus making privacy more difficult. None of the respondents gave information about their ‘issue’ (infertility) to those outside their immediate family and a little more than two-thirds (80 per cent) made a ‘selective disclosure’.
ART, Body and Belief
The anxiety 18 and pressure that go along with ART entrap women into a medical ‘machine’ for a time that often seems to go on forever. Medical machines portray themselves as possessing agentic capacities to discipline bodies and inevitably entail a missed identification between the individual and social bodies; and a tendency to transform the social into biological. With the development and expanded use of ART, the last decade of the 20th century and the early decade of the 21st century witnessed this increase to cover reproductive body elements, such as sperm, eggs and embryo-entities which have been turned into ‘commodities’. The woman’s body is now not only dispensable as a ‘field’ but seen as deficient, needing to be modified. Meenu, a 33-year-old woman from Cuttack, a business area of Odisha, explains: ‘In the clinic, the treatment-provider speaks to you in a certain way, as if something is being [re]framed for performance’. So, ART in a globalised market creates a reproductivised image to sell to consumers/seekers especially true for women, making their [fertile] bodies. The product [child] obviously plays a part in constructing the image of the self, resulting in an objectified body. Women (65 per cent) perceive ART as God’s active engagement with them, just as God intervened in a woman’s body what Nina Majhi, a 30-year-old woman, married for nine years narrated: ‘I took this treatment which cost ₹1,00,000. The procedure was very painful. The first time, it did not work. After a gap of three months, I took the treatment again which finally showed a [positive] result’.
Nina’s story is the production and modification of body through ART. It can be reasoned that pregnancy is an embodied form of work. Brandth and Haugen (2005, p. 91) write, ‘The body [is] reduced to matter, something that has to be controlled and managed’. Women like Meenu and Nina represent a pattern in which women anxious of their fertility undergo ART interventions. The point is that social actors have the capacity to affect biology and centre the body within a social context. However, it is the body that is being acted upon, resulting in a modified product.
Uma, a 30-year-old woman, in her sixth month of an IVF-induced pregnancy averred:’ Without a child one has no status, whether inside or outside a family’. Sudhir Kakar (1978) goes a big step further in The Inner World, his psychoanalytic study of Indian childhood, when he writes that even the unborn child while still in the womb wins for its mother the love, respect and acceptance of the community. Users like Uma believe that treatment-providers are, ‘God sent’ creatures and can assure a child once they begin treatment. There are other treatment-seekers who have complete trust in this technology and its providers and are disappointed when it doesn’t work for them. In those cases, they appear irrational and blame their own body. They even try to console themselves by saying, ‘God has not given us what we want, why pine for it?’
The social construction of infertility is based on everyday routines, interaction and events. These are the source of individual experiences through which meaning gets established. When a person attempts to establish a link between the duration of marriage and childlessness and such linkages play a critical role where a woman finds reality. It is important to understand the ways in which women experience everyday life and imbue their activities with meaning. Women encounter with this already constituted, meaningful, inter-subjective life-world, which is the ‘paramount reality’ for women and the way in which they experience this everyday life-world.
Concluding Observations
Cultural change 19 through the existence of new technological options is expanding possibilities for women in Odia society in general, and in families in Odisha in particular, but women continue to be constrained by the idea of pronatalism and patriarchy. 20 In this context, married women are finding ways to sustain their marriages with a technologically-induced baby—constructing families in which they seek to position themselves; a facet quite evident in contemporary Odisha. A focus on local articulations and attitudes to childbearing and the related response to the existence of technological options enables us to understand the concerns of childbearing (fertility) and cannot be understood apart from that of childlessness (infertility), what Inhorn (1994) calls the fertility–infertility dialect.
Women in the study carried multiple identities with them: wife, daughter, daughter-in-law and of course, as a woman. One of those behavioural expectations for these identities is often to become a mother. Recognising ART as a ‘supreme saviour’ of the distresses faced by infertile women and may enact the potential mother identity. Dr Monu Pattanaik, a leading infertility treatment specialist in Rourkela, cites ‘cultural reasons’; that childless couples here [in Odia society] view producing progeny as an almost sacred duty, and articulate Hindu teachings about being rewarded in the next life for such deeds performed in this one. The analysis suggests that women’s reasons for resorting to ART are rather complex (for example, family pressures and cultural expectations. The family plays a critical role in determining the extent of stigma and exclusion faced by women, deciding a woman’s access to healthcare, and in providing much-needed emotional and financial support. Negotiations around childbearing are perceived as a benefit made available by the existence of new technological options. So, the existence of new technological options through ART brings encouragement from concepts which are deeply embedded in the culture of Odisha. Respondents agreed that there was a lack of opportunity earlier to explore other options; now that’s not the case. If anyone is given privacy and anonymity, he or she will engage in ART. As this article finds, reproductive choices through ART are valued highly by infertile women and accepted without qualms.
In Odisha, ART has not only brought some ‘hope’ into the lives of the infertile but also enabled an expansion in the baby-manufacturing industry. Once the technology exists to manufacture the child, ignoring it means being deprived of technological advancements. While many treatment-providers, seeker groups and media believe that medical innovation opens up human bodies to longer, better life spans and a wider variety of sensations and experiences, other constituents worry about how new medical technologies (for instance, ART) perpetuate patterns of unequal access to medical care.
New medical technologies often challenge and remake frameworks for evaluating ethics of biomedical procedures. What happens when new medical tools come up against existing ethical sensibilities? For instance, ART provides normative challenges as they widen the scope of reproductive choices and contest the traditional notions of motherhood, pregnancy and childbirth. The people who are not educated, for them, changing childbirth practices is part of the complex imagery of modernity alongside transformations of conjugality.
The larger question that arises is: should necessity trump ethics? In one sense, technologies in the field of assisted reproduction fulfil individual needs. Ideally, as also demanded by the women’s movement, besides contraceptive provision, reproductive healthcare should also include measures and services for the infertile and the norms governing them. In another sense, globalisation-driven ART services are offered by private fertility clinics, seemingly a capitalistic enterprise. Even though women rationalised ART, women too had concerns in terms of safety and health risks. Sometimes, the desperation and ignorance of infertile women puts them at a possible health risk, especially for those whose general health condition because of a low socio-economic background, makes them more vulnerable to mortality associated with pregnancy. According to treatment-providers, ART still has some safety problems and risks that need to be described and evaluated so that current clinical policies and laboratory procedures can be revised, if necessary’ (Malhotra et al., Shah, 2013).
What is at stake when bodies reframed by ART encounter established ethical norms in a clinic/hospital? In the larger scenario, the state’s acceptance of ART in its health policies reflects how it is caught between attempts to regulate private fertility clinics which provide access to technological options on the one hand and the state-led ‘development’ agenda to control fertility in the provision of reproductive technologies (where couples/women in India are expected to produce not more than one or two children) on the other. The pressing need to regulate private fertility clinics, seen recently by state legislation has invoked amendments in the ART Bill (Government of India [GoI], 2015) to deliver safe and ethical practice of ART services while enforcing checks on clinics. Time will tell whether the state has gone far enough to succeed.
The limited sample size might not represent all women in the state of Odisha but the study argues how ART has been responsible for the new reproductive consciousness of infertile women/couples which will grow further in Odisha. There has been a major shift in reproductive practices in Odia society, which is related to the culture of state planning and the different ways the private fertility clinics and the Odisha government approach, and use ART.
Footnotes
Acknowledgements
Support from the Indian Council of Social Science Research, New Delhi made this research possible. Earlier versions of the article were presented at Jawaharlal Nehru University (JNU) New Delhi (2011); Hyderabad Central University (2012) and Ravenshaw University, Cuttack (2013). Thanks are due to our anonymous reviewers for making us think harder and improve the argument. The (late) Aneeta A. Minocha, Delhi School of Economics, University of Delhi; Binay Kumar Pattnaik, Indian Institute of Technology Kanpur; Madhav Govind, Centre for Studies in Science Policy, JNU and Prachinkumar Rajeshrao, Centre for Social Medicine and Community Health, JNU; gave us some thoughtful advice and constructive criticism. Any errors are the responsibility of the authors and do not reflect the thoughts of their respective institutions.