
Abstract
Summary
We investigated the causes, management and outcome of head injuries in paediatric patients admitted to the paediatric surgery unit at King Edward VIII Hospital overa 3-year period, from 1999 to 2001. There were 506 patients (331 male; M:F ratio 2:1) and the mean age was 71.99 +36.8 months (2 weeks to 180 months). The injuries were due to: motor vehicle crashes (324); falls (121); assault (30); inadvertent injury (23); and unknown (11). Forty-nine patients (9%) were admitted with a Glasgow Coma Scale ≤8. The most common intracranial pathology on computed tomography was: intracranial haematoma/haemorrhage (44); contusion (16); and brain oedema (10). Nineteen patients (3.4%) underwent neurosurgical intervention and the rest were managed conservatively. Eighteen died in hospital (3.6%). The mean hospital stay was 5 ± 12 days. Twenty-three patients (4.5%) were discharged with neurological sequelae. Few paediatric patients are admitted with severe head injury: the majority from blunt injury caused by motor vehicle crashes. Management mainly requires simple neurological observation in a general ward with a surprisingly good prognosis. Specific protocols for paediatric head injuries have been proposed based on these findings.
Introduction
Trauma is the second most common cause of death in South Africa and mainly involves children. 1 Head injuries account for the majority of trauma related deaths, being marginally more common than torso trauma.1,2 There is paucity of data on paediatric head injuries emanating from South Africa with little information on long-term outcomes due to poor patient follow up. This begs the question of whether or not the currently available literature can be generalized and applied to our setting.
The purpose of this study was to investigate the management and outcome of head injury in a South African paediatric population and to critically analyse the trends. Such analysis would allow the proposition of relevant and evidence-based protocols for the on-going management of paediatric head injury in our setting.
Patients and methods
Participants in this retrospective review of prospectively collected data were children aged less than 12 years who presented to the King Edward VIII Hospital with head injuries from January 1999 to December 2001.
The general paediatric surgical ward was situated at King Edward VIII Hospital (KEH) and the neurosurgical unit (NSU) at Wentworth Hospital which is 5 km from KEH. Patients requiring neurosurgical intervention were transferred to the NSU after consultation with the neurosurgical medical staff.
The patients were assessed by clinical examination and the data were entered on a prescribed proforma, which included: demographic details; age; cause of injury; Glasgow Coma Scale (GCS); findings on local examination; radiology results; referral; management; outcome; and duration of hospital stay. Investigations included, but were not limited to, skull X-rays, computed tomography (CT) scans and blood tests. Indications for admission to hospital in the Durban Metropolitan Hospital services have been described by Zulu et al. 1 and include: a period of loss of consciousness; presence of neurological deficit; and all patients with a GCS of <15. Indications for an urgent CT scan are GCS <15 after optimization of the patient and the presence of a neurological deficit. Indications for a semi-elective CT scan during hospitalization include: any deterioration in the level of consciousness; development of neurological deficit; or failure of an improvement of the GCS for more than 48 h even in the absence of a fracture or focal neurological signs. Severe head injury was defined as GCS ≤8. Patients with a GCS ≤4 from the time of injury, and those that were hypotensive or hypoxic, were resuscitated and re-evaluated.
Patients were managed in the general paediatric surgical ward with neurological observation. Indications for referral to the NSU, described by Zulu et al., 1 include intracranial pathology requiring surgical intervention or intensive monitoring. Patients with intracranial pathology underwent surgery if they fulfilled one or more of the following criteria: size of the haematoma or contusion of more than 30 cm2; midline shift of more than 10 mm; and effacement of the ipsilateral ventricle. Those with a GCS of 15 with no localizing signs and those with intracranial pathology but no mass effect were managed non-operatively with periodic neurological assessment. An intracranial pressure monitor was inserted in the following circumstances: patients undergoing surgery for evacuation of a space occupying lesion (except for a pure extradural haematoma); and patients with evidence of increased intracranial pressure on CT scan but with no mass lesion. All neurosurgical interventions, as well as operations on the cranium (such as debridement), were performed at the NSU.
The proformas were collected and compiled into an electronic form using Microsoft Excel and were prepared for statistical analysis.
Results
There were a total of 506 patients with 507 episodes of head injury and 508 hospital admissions (one patient had two separate episodes of head injury and another had two admissions for the same injury). Their mean age was 72 ± 36.8 months (range 2 weeks to 180 months). There were 331 males with a male: female ratio of 2:1. Apart from one penetrating firearm injury, all the injuries sustained were of blunt origin and a motor vehicle crash (MVC) was the most common offender (63%), followed by falls (23%) and assaults (5%) (Table 1). Inadvertent injury was due to various household and non-household objects falling on children.
Mechanisms of injury in 506 patients with 507 head injuries
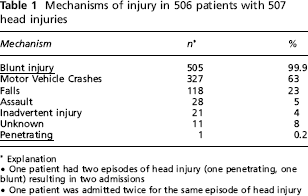
Explanation
One patient had two episodes of head injury (one penetrating, one blunt) resulting in two admissions One patient was admitted twice for the same episode of head injury
The mean GCS on admission was 13.1 ± 2.9 and 49 patients were admitted with a GCS ≤8. Intracranial pathology was detected in 78 of 152 patients in whom CT scans were performed. The most common intracranial pathology was subdural haematoma followed by cerebral contusion, intra-cerebral haematoma and cerebral oedema in that order. In-driven bone fragments were the only form of skull fracture which was managed surgically at the NSU (Table 2).
Intracranial pathology in 78 patients with head injury
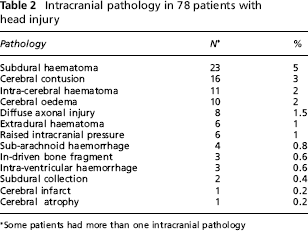
Some patients had more than one intracranial pathology
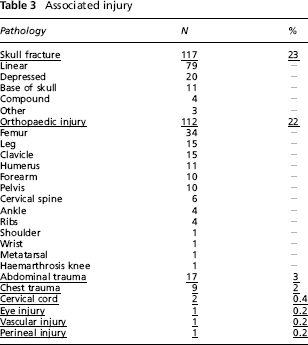
There were a large amount of associated injuries (Table 3). Apart from head injuries, orthopaedic injuries were the most frequently encountered associated injuries. Femoral fractures (34), tibial and/or fibular fractures (15) and clavicular fractures (15) were the most common forms of orthopaedic injury not involving the head. Abdominal and chest trauma were also commonly seen.
Associated injury
Four hundred and eighty-six patients (96%) were managed conservatively in the form of head elevation and neurological observation. Nineteen (3.8%) were referred for neurosurgical intervention namely: eight haematoma evacuations [extradural haematoma (3), subdural haematoma (3) and intracranial haematoma (2)]; seven skull debridements; two insertion of an intracranial pressure monitoring device in two patients; and two evacuation of the contusion (Table 4).
Management of patients with head injuries
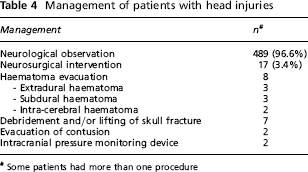
Some patients had more than one procedure
Eighteen patients died in hospital, giving an overall mortality rate of 3.6%. Seventeen of 49 patients with a GCS ≤8 died (34%) compared to one of 459 patients (0.2%) with a GCS >8 (P < 0.0001). The mean hospital stay was 5 ± 12 days. Twenty-three patients (4.5%) were discharged with neurological sequelae (Table 5).
Neurological sequelae at discharge
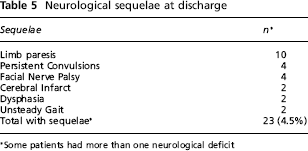
Some patients had more than one neurological deficit
Discussion
The regional NSU which is currently situated in Inkosi Albert Luthuli Central Hospital was previously situated in Wentworth Hospital before 2002. 1 The unit serves the whole of the KwaZulu-Natal Province and part of the Eastern Cape Province. 1 Therefore, that paediatric head injuries are managed, at least initially, in the setting of a general paediatric surgical ward before referral to the regional neurosurgical unit where necessary.
Traumatic head injury has an approximate prevalence of 180–300 per 100,000 paediatric patients per year. 3 In Spain, 5% of all the paediatric age group patients treated in emergency wards have suffered a head injury. 4 Penetrating head injuries are rare and even more so amongst the paediatric age group but, when they do occur, they are very severe.4,5 This is despite the greater risk of penetration of the skull and dura after minimal force in children under 2 years of age because of incomplete ossification of the calvaria. 3 Penetrating head injuries are fatal in 40% of cases 4 with late complications manifesting in the form of infection and secondary haemorrhage. 5
As in all developing countries, interpersonal violence and vehicular crashes are commonplace in our setting. 1 In this study, the vast majority of head injuries resulting from blunt trauma were caused by motor vehicle crashes.
The treatment of minor head injuries in children has been debated for years. 6 Children with a normal neurological examination and normal brain CT scan are not at risk of significant neurological complications and can be discharged home with parental supervision thus avoiding unnecessary and costly hospitalization. Such patients are able to return to their previous activities with no significant neurological sequelae.6,7
Early response time improves outcome in patients requiring surgery. 6 The small proportion of patients requiring neurosurgical intervention, 4% in this series, demonstrates the effectiveness of non-surgical management in the majority of patients. Generally, only 2.6% of patients with a GCS of 15 will require neurosurgical intervention following head injury. 6 However, these patients all have obvious findings on admission and a CT scan that warrants neurosurgical intervention and, as such, are hard to miss. 6 Neurological observation in the general paediatric ward has been the mainstay of management for patients with mild to moderate head injury and has been found to be safe and effective in the vast majority of cases in this, as well as in other, series. 1 The rate of neurosurgical intervention is very low and those that do require it are able to be identified as early as possible.
The mortality rate of 4% was less than the 10%-40% reported in the published literature in both adults and children. 1,8 The mortality rate of 34% following severe head injury was favourable compared to the reported 44%-67% in other studies1,9 This demonstrates that in this study, as in others,1,8–10 the GCS on admission is a good predictor of mortality. Furthermore, the findings are in agreement with other findings that children have a generally more favourable outcome than adults.8,9
The number of patients with a residual neurological fall-out was very low (5%) and much lower than the 17% noted by Zulu et al. 1 from the same institution in 2007. The low mortality rate and the low neurological sequelae seen in this study suggest that the current management of paediatric head injuries in KwaZulu-Natal is largely successful and that there is little disadvantage associated with the management of the majority of head injuries at a peripheral hospital level in a general paediatric surgical ward.
Patients with severe head injury will retain a high mortality rate regardless of the management approach as the outcome is predicted by the GCS on admission and, thus, no additional intervention is likely to influence outcome in this group.
There is evidence that neuropsychological performance, such as school performance, may deteriorate after head injury even if there are no residual physical deficits.11,12 Although neuropsychological testing was not routinely available, and subtle morbidities may be under-represented in this experience, the number of patients with gross neurological fall-out was very low.
Figure 1 details the management protocol that we adopted for the management of head injuries. We have demonstrated that this protocol is safe for the management of all head injuries in adults and children. We believe that this protocol should be applied countrywide.
Suggested management protocol for head injuries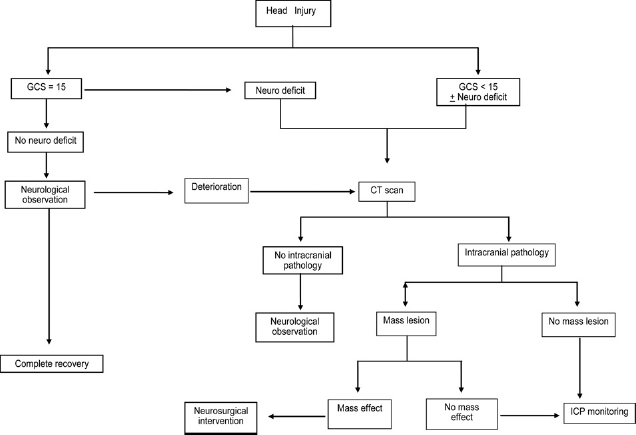
Conclusion
Motor vehicle crashes are the greatest cause of paediatric head injury in our setting and are the reason for the high associated orthopaedic injury rate. Few paediatric patients are admitted with severe head injury. The GCS on admission remains a reliable predictor of mortality. Management, in most cases, requires simple neurological observation in a general ward with a surprisingly good prognosis. The management protocol espoused in this series should be considered for use in the rest of South Africa as well as in other developing countries. Patients requiring neurological observation and referred to NSU must be carefully selected and referred early for intervention. Further studies to validate this management protocol in children are warranted.
This study provides a suggested management protocol for paediatric head injuries which we feel should be used as a guide for the management of paediatric head injuries in developing countries.
Footnotes
Acknowledgements
We are grateful to Ms E Conner for maintaining the database.