
Abstract
Dengue fever has emerged as a major public health problem globally in the past three decades. A 13-year national surveillance data analysis was done to describe the epidemiology and its trend of dengue disease in Oman reported between 2001 and 2013. Laboratory-confirmed dengue virus infections reported were studied retrospectively during the study period. A total of 64 laboratory confirmed cases were reported. All the patients contracted the disease during their visit to South-East Asian countries, hence classified as imported cases. The majority of the cases were reported in the year 2012 (23.4%). The most important clinical characteristics were fever (90.6%), myalgia (35.9%) and rash/petechial rash (20.3%). Thrombocytopenia was seen in 31.2% of the study subjects. The mortality was nearly 4.6% and all other patients made a full recovery. The most effective measure for travellers is taking precautions to avoid mosquito bites.
Introduction
Dengue fever has emerged as a major public health problem globally in the past three decades (Figure 1). The Aedes aegypti mosquito-borne infection is predominant in urban and semi-urban areas in tropical and sub-tropical regions worldwide. Infection with any one of four dengue virus serotypes (DENV-1, 2, 3 or 4) can produce a spectrum of illness ranging from a mild non-specific febrile syndrome to classic dengue fever (DF), or severe disease forms such as dengue haemorrhagic fever (DHF) and dengue shock syndrome (DSS) that can be fatal.
1
Average number of DF/DHF cases reported to WHO and average annual number of countries reporting dengue.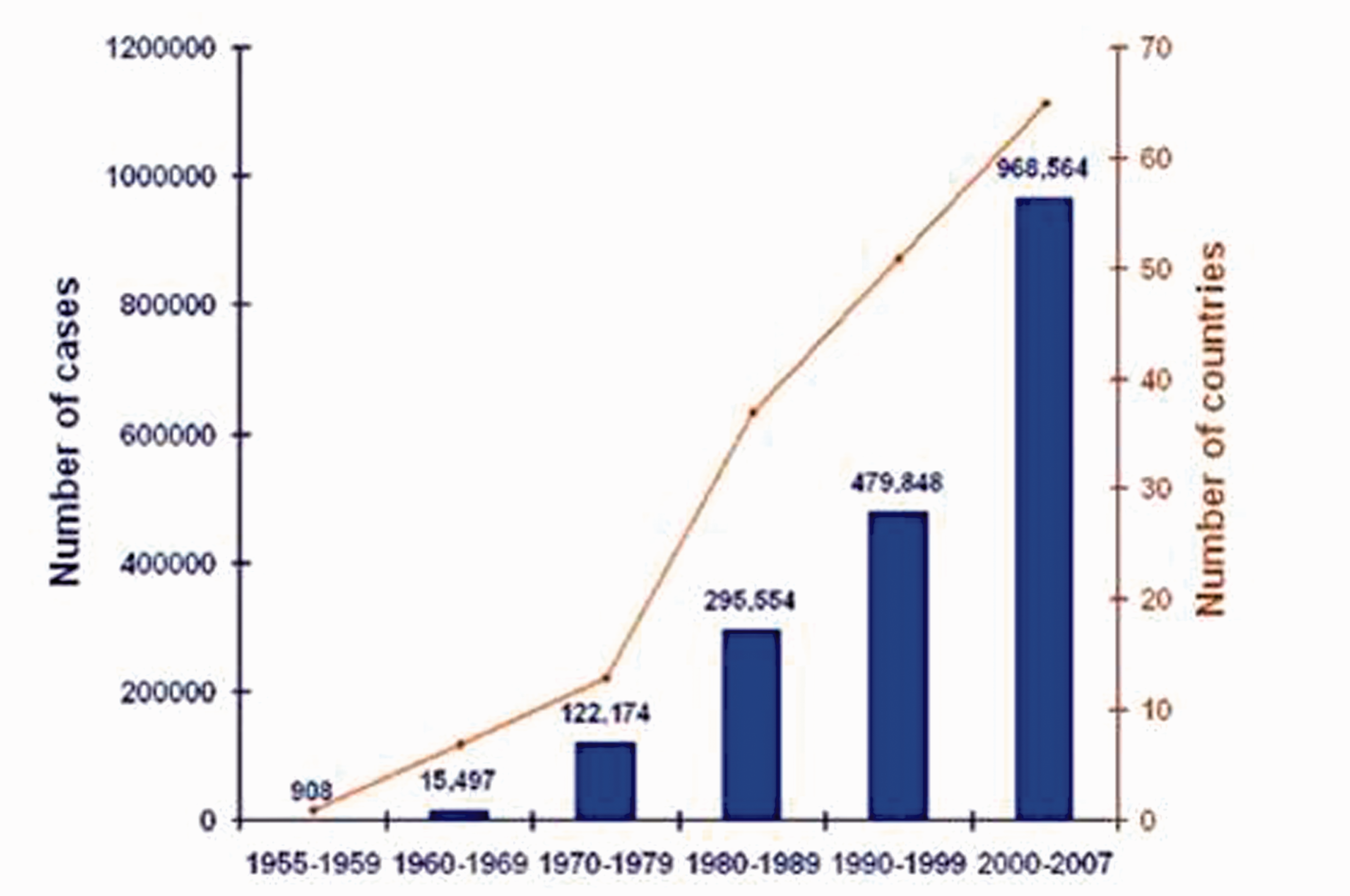
It is now endemic in more than 100 countries (Figure 2) with about 2.5 billion (40%) of the world’s population at risk and 90% of them are children. An estimated 500,000 people with severe disease require hospitalisation each year, and nearly about 2.5% of those affected die. Without proper treatment, DHF fatality rates can exceed 20%. During epidemics of dengue, infection rates among those who have not been previously exposed to the virus are often 40–50%, but can reach up to 80–90%.2–5
Countries or areas where dengue has been reported.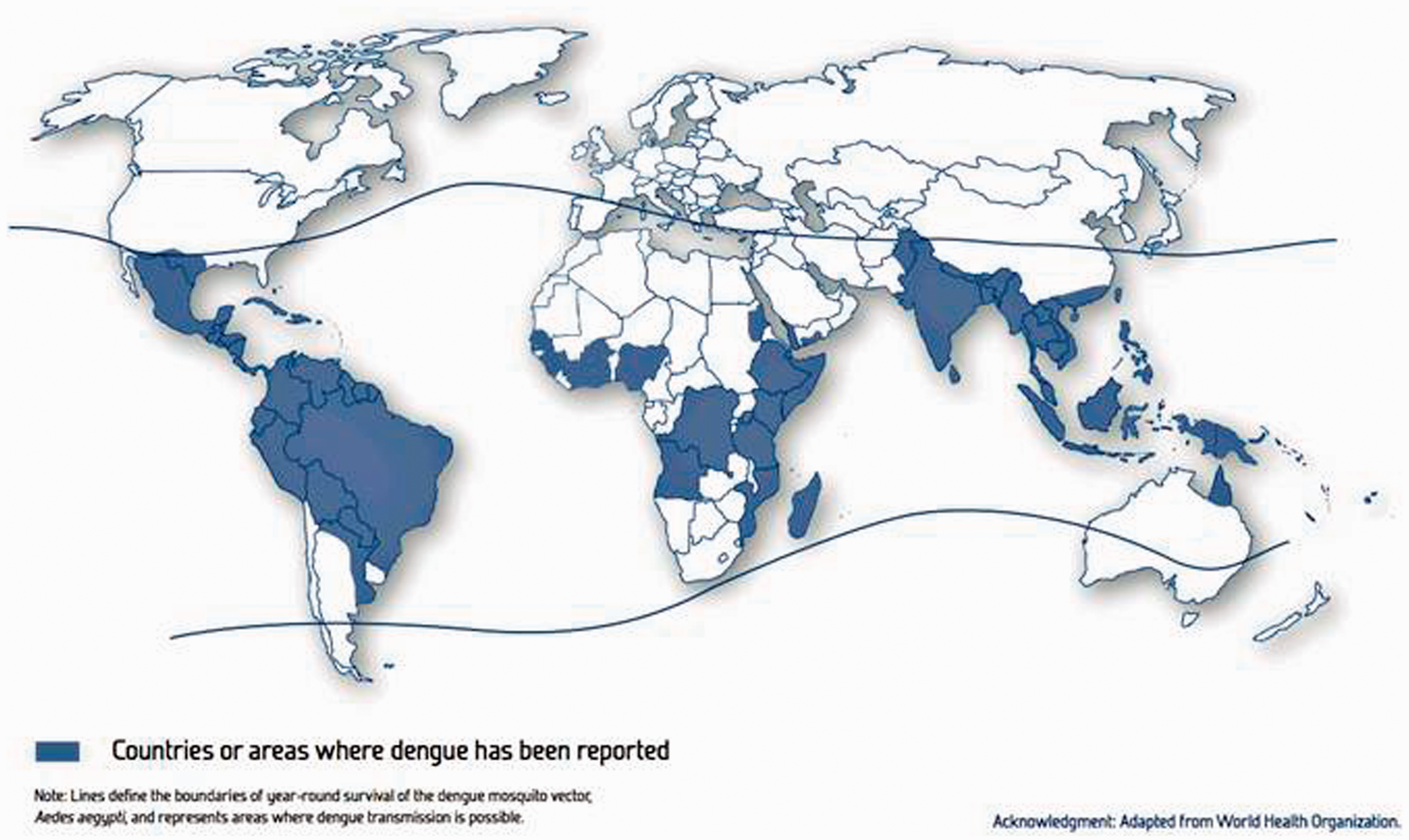
In the Eastern Mediterranean Region (EMR), dengue is re-emerging after a decline in the 1940s due to widespread use of dichloro-diphenyl-trichloroethane (DDT) against the vector. It is now endemic in Yemen, Saudi Arabia and Pakistan (Group A). Aedes aegypti as the main vector mosquito has been recorded in 13 of the 22 countries of the EMR including Oman. Aedes Albopictus is a lesser vector and has been only recorded in Pakistan. 6
Dengue is a notifiable disease in Oman. Oman has been classified as Group C: where imported cases have been reported but there is no evidence of endemicity or local transmission of the disease. 7
This report summarises surveillance data on dengue fever collected in Oman from 2001 to 2013 with the objective to depict the epidemiological trend and strategic implications of imported cases and recommendations to prevent future indigenous transmission in Oman.
Methods
Background information
Oman has a hot climate with temperatures reaching around 50℃ (122.0°F) (peak) in the hot season, from May to September. It receives very little rainfall, the annual rainfall in Muscat averaging 100 mm (3.9 in), falling mostly in January. The Dhofar Mountainous area receives seasonal rainfall (from late June to late September) as a result of the monsoon winds from the Indian Ocean. Oman has a population of nearly 2.8 million, of whom 30% are expatriates. Nearly 90% of the population lives in the northern parts of the country with over 50% living in the capital, Muscat.8,9
Study design
Record review of surveillance data retrospective study
Study population
All cases reported under viral acute haemorrhagic syndrome and later confirmed as dengue fever by laboratory testing.
Study period
Cases reported between the years 2001 to 2013.
Case definition and data collection
Acute onset of fever of less than 3 weeks duration in a severely ill patient and any two of the following: haemorrhagic or purpuric rash, epistaxis, haematemesis, haemoptysis, blood in the stools, other haemorrhagic symptoms and no known predisposing host factors for haemorrhagic manifestations based on the World Health Organization (WHO) case definitions. 2
Communicable diseases case notification form (PR-14) was used to collect the data by the governorates communicable diseases units and compiled centrally by the Department of Communicable Disease Surveillance and Control (DCDSC). The following data were recorded for each patient: age, sex, clinical presentation, travel history and laboratory results. 10
Disease surveillance
Substantial progress has been made in the control of several of the priority diseases in the last three decades since the communicable disease surveillance system was launched in Oman in March 1991. National surveillance of dengue was established in 1995 and involved reporting of clinically diagnosed cases as a Group A syndrome under acute viral haemorrhagic fever (VHF) along with virological surveillance. 10
Laboratory testing
Serological diagnostic facilities are available in the Central Public Health Laboratory (CPHL) for Dengue/Dengue Haemorrhagic Fever (DF/DHF), Crimean Congo Haemorrhagic Fever (CCHF) and Rift Valley Fever (RVF). All blood samples from acute haemorrhagic fever syndrome cases as a routine would be subjected to all three of these tests. The paired serum specimens are tested using an immunoglobulin M (IgM) antibody capture enzyme-linked immunosorbent assay (ELISA) and a haemagglutination inhibition assay. The first sample is tested for viral ribonucleic acid using a modified version of the reverse-transcriptase polymerase chain reaction (RT-PCR) procedure. Serum samples should also be taken for serology after 14 days of onset during the follow-up visit. 10
The kit used is a Panbio Dengue IgM Capture ELISA for the qualitative presumptive detection of elevated IgM antibodies to dengue virus. A positive result (>11 Panbio Units) is indicative of either an active primary or secondary dengue infection. 11
Vector control interventions
There were no specific vector control measures taken against dengue vector because there were no indigenous cases reported and the absence of vector in Oman. 10
Data analysis
The data were entered into a computerised database using statistical software (Epi Info 2000 version 3.3.1, Centers for Disease Control and Prevention, Atlanta, GA, USA). The data were analysed statistically using the Statistical Package for the Social Sciences (SPSS) version 19 software. Results were expressed in means for age, onset of illness, admission and report. Other parameters were expressed in proportions.
Results
Between 2001 and 2013, a total of 336 suspect cases of acute VHF were reported. The laboratory evidence on record showed 72 cases as IgM positive for dengue disease, out of these eight cases were discarded after a second test was negative. The remaining 64 cases (study subjects) were all travel-related of which 37 cases (nearly 57%) had a history of travel to India. Epidemiological investigation revealed no evidence of indigenous transmission; hence, all are classified as imported cases. Seventeen (26.5%) cases among nationals had a history of returning from dengue endemic countries (six from India, two each from Pakistan and Malaysia, four from Yemen and one each from Tanzania, Thailand and Saudi Arabia, respectively).
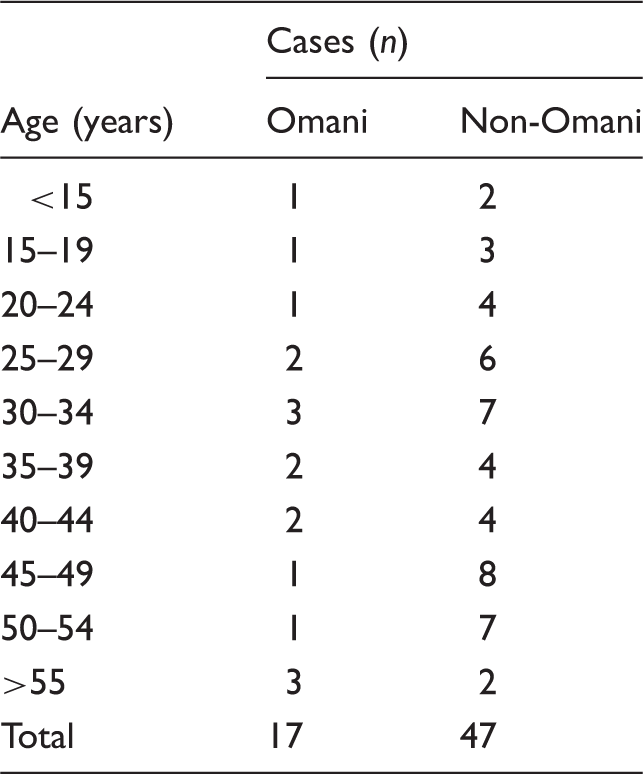
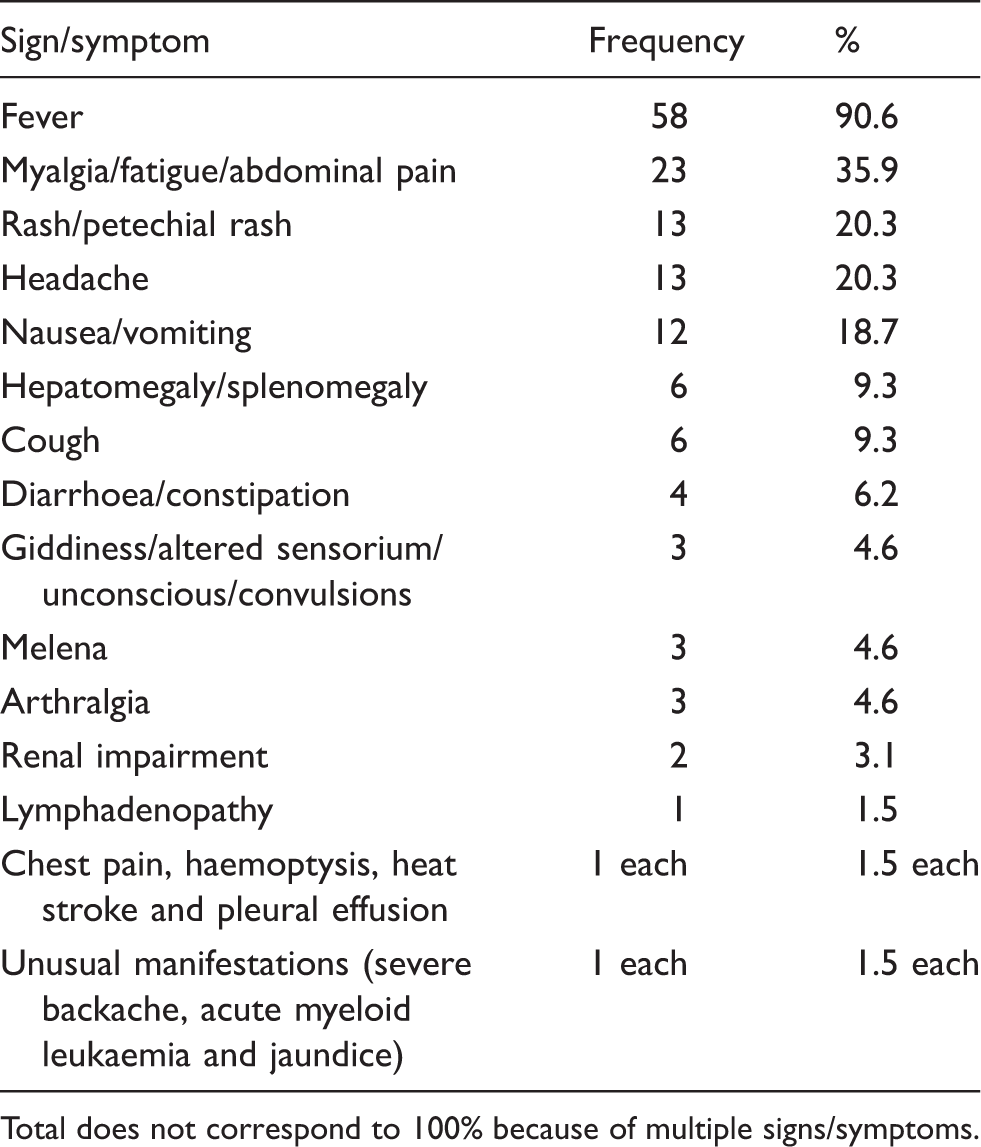
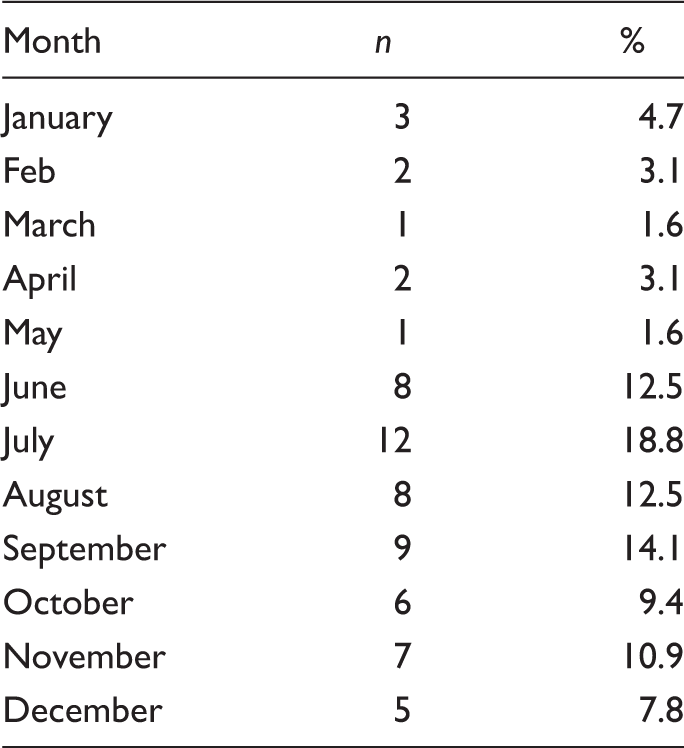
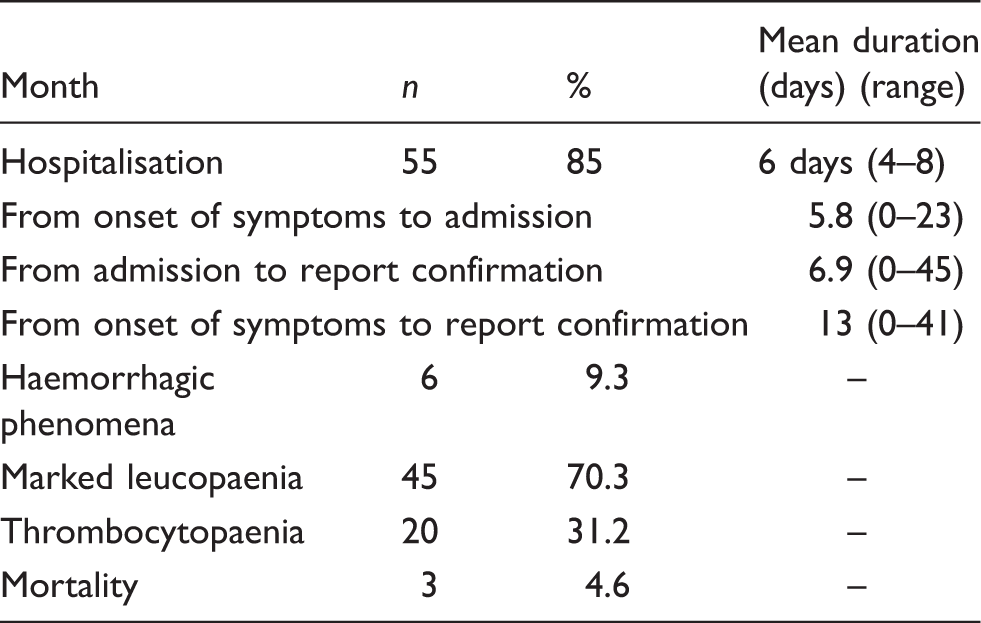
The mean age in the study population was 36.4 years (range, 3–72 years). The majority of the study subjects were working expatriate adults (Table 1). Fever was noted in 90.6% of patients. In 65% of patients, symptoms started a median of 3 days after return. Clinical signs and symptoms in our patients are summarised in Table 2. Figure 3 and Table 3 show the year-wise and month-wise distribution of cases. The maximum number of cases was observed between June and September 2012. The majority of the study subjects were men (76.5%, 49 of 64). Only two cases had the serotype report in which DENV-2 was isolated. There is no difference in reporting of cases in various regions/governorates or wilayat (administrative district). Table 4 elaborates the hospital and laboratory findings.
Year-wise distribution of cases. Dengue IgM positive cases during 2001–2013 age distribution and nationality (n = 64). Clinical spectrum of dengue disease patients reported in Oman (n = 64). Total does not correspond to 100% because of multiple signs/symptoms. Seasonal trend of dengue among study subjects (2001–2013) (n = 64). Hospital and laboratory findings (n= 64).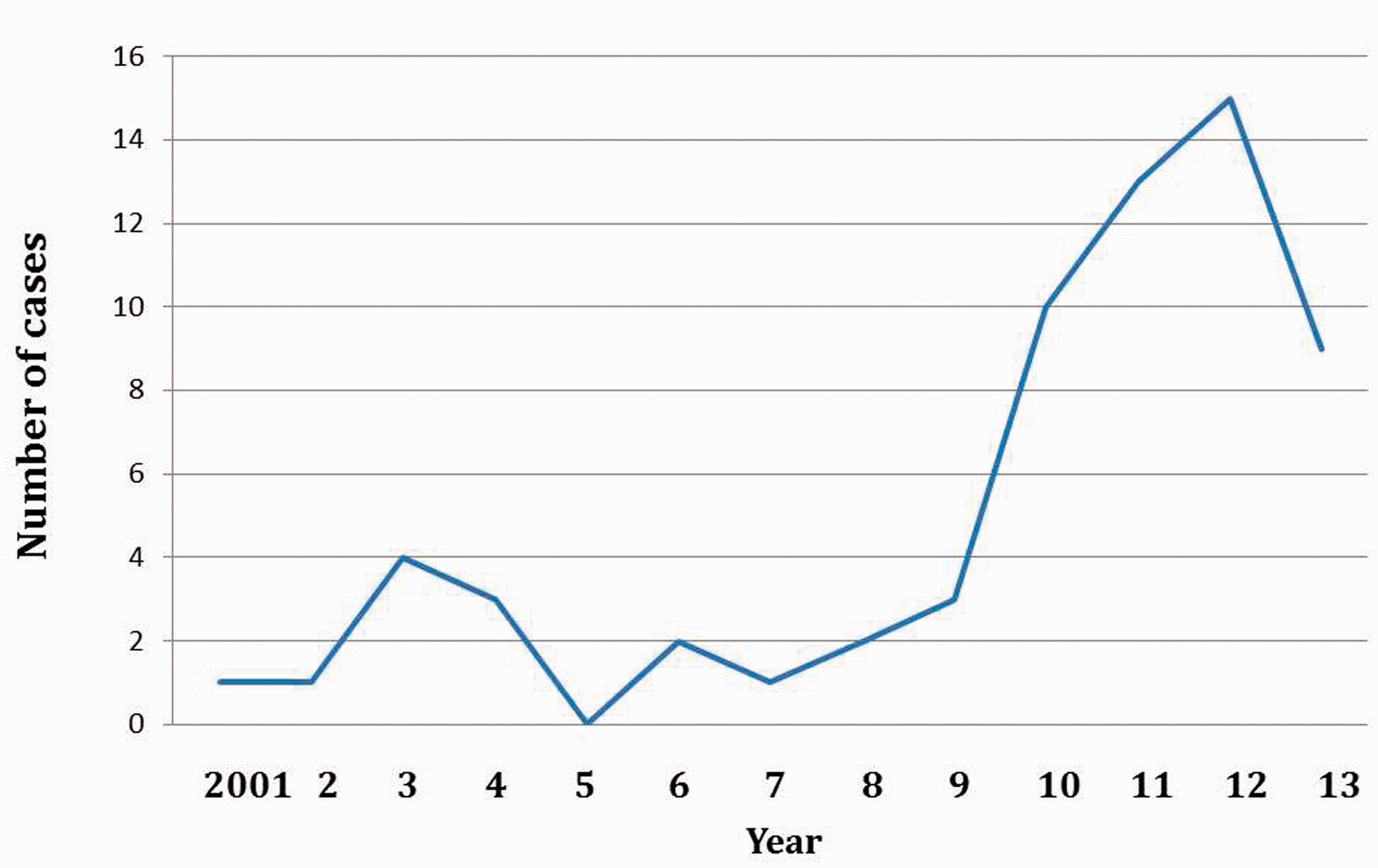
Discussion
Although dengue surveillance was started in 1995, we focused on the period 2001–2013, during which more complete and reliable data on patients were available. In general there was no change in the overall annual number of cases in the period 2001–2009, although there was an increase in case numbers in the last 4 years (2010–2013). The key contributing factors to the worldwide resurgence of dengue in the last few decades include the rise in number and size of densely populated urban cities, the adaptation, proliferation and geographical expansion of dengue vectors, particularly Aedes aegypti, and increased global travel.12,13
Few cases were seen in infants and children, presumably because itinerant workers are more frequently adult males.4,14–17
All the cases reported were travel-related and there was no indigenous transmission of dengue within Oman. Due to concerns over possibility of introduction of dengue in Oman the following recommendations were sought.
There is no completely effective method of preventing dengue infection in travellers visiting tropical areas with the absence of an effective tetravalent vaccine. The risk of infection can be significantly decreased. The single most effective measure of dengue prevention for travellers to areas where dengue is endemic is taking precautions to avoid mosquito bites.13,18,19
There was no evidence of dengue vector in Oman till recently it was reported in 2008 in Dhofar Governorate and Aedes egypti was seen in three villages, namely Surfat, Deem and Dhalqut. The House index used to monitor breeding potential of areas showed marked increase from 2008 to 2010. Hence, challenges remain in prevention of possible indigenous transmission in Oman.
6
Periodic entomological surveillance, monitoring the vector breeding seasonality especially during July to August (Khareef season), monitoring the insecticide spray and sensitivity, training of local health staff in monitoring, community involvement and community participation are some of the suggested measures.
6
Dengue fever is a complex disease and surveillance is a challenging task because of rare occurrence and DF may not be suspected as a cause of particular symptoms. Dengue diagnosis cannot be made by clinical judgement alone; it requires laboratory support that may not always be available in health centres. Problems of under-diagnosis, incomplete reporting and reporting delay also weaken surveillance.
20
Laboratory testing algorithm modifications are required to include additional tests for confirmation of the diagnosis. Further studies, which should include full genome sequencing, are needed to explore the association between dengue serotype, virus virulence and disease severity. Monitoring serotypes and strains circulating in the population may be an important indicator of future epidemics of dengue disease.20,21
Conclusion
Dengue is currently a global threat and is endemic or epidemic in almost every country located in the tropical regions. Owing to an increase of the expatriate population and frequent travel of native Omani people to South-East Asian countries, prevention and control of imported cases of dengue are a challenge. Dengue is a complex disease and its prevention and control is a multi-sectoral effort which requires strong community participation. The current presence of the vector in Dhofar Governorate in Oman increases the risk of indigenous transmission and effective vector control is the only way to prevent the disease. While waiting for new tools such as a safe and effective tetravalent vaccine, antiviral drugs and improved diagnostic tests, better use should be made of the interventions that are now readily accessible. With proper focus, new initiatives and continual effort, we hope to prevent the indigenous transmission in Oman.
Footnotes
Acknowledgements
We are grateful to all governorate epidemiologists and regional hospital staff for their invaluable support.
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.