
Abstract
Objectives
How traditional birth attendants (TBAs) in post-war Sierra Leone explain, handle and prevent postpartum haemorrhage (PPH) and their potential role in a better management of PPH to reduce maternal mortality in this low resource setting.
Methods
Semi-quantitative interviews about knowledge and measures in PPH and participant observation with 140 Sierra Leonean birth attendants, divided in three groups: (A) TBAs who never attended any official training course (n = 82); (B) TBAs who attended at least one official training course (n = 48); and (C) officially trained birth attendants (n = 10).
Results
There are several observable gaps in the knowledge of TBAs about PPH compared to modern obstetrics, however similar procedures exist. Herbal medicine is applied; metaphysical convictions about PPH remain present. Training courses show an impact. Officially trained birth attendants demonstrate knowledge deficiencies and lack resources and infrastructure to manage PPH adequately.
Conclusions
Morbidity and mortality of PPH in Sierra Leone is related to several factors and not solely to the ignorance of TBAs. TBAs still play an important role for many women there. Hence improvement of the formal health sector should be combined with life-saving programmes integrating TBAs in the care for the pregnant, delivering and breastfeeding mothers.
Keywords
Introduction
Each year, there are approximately 273,500 maternal deaths worldwide. Most of them take place in underserved nations, especially in sub-Saharan Africa. 1 Maternal haemorrhage accounts for 23% of all obstetric death cases. 2 The majority of postpartum haemorrhage (PPH) is related to uterine atony. 3 The management and outcome of PPH depends grossly on geographical location and resources available.
Sierra Leone is a country in West Africa with approximately 5.7 million inhabitants. During the civil war from 1991 to 2003, the infrastructure and the health system were battered dramatically. The consequences are still apparent. This is especially true for maternal and child health. 4 The maternal mortality rate in Sierra Leone is extraordinary high. For 100,000 live births, presumably 860–970 mothers die. 5 Reacting to these dramatic numbers, the government of Sierra Leone, supported by international donors, offered free healthcare services for children under the age of 5 years as well as pregnant, delivering and lactating mothers. This political decision was launched in April 2010. Whether this approach affects the morbidity and mortality rates remains to be seen.
Worldwide, around 60 million children are born outside of official health institutions each year. 6 The majority of these deliveries are attended by traditional birth attendants (TBAs). TBAs are political and religious authorities, embedded in the local traditions of their community. For many women, TBAs are the only assistance during pregnancy, delivery and post partum. Often the TBAs enjoy more trust than the staff of official health institutions. 7
Sierra Leone may have similar epidemiological data, although reliable data do not exist. The Ministry of Health in Sierra Leone believes that ante- and postpartum haemorrhage accounts for 17% of maternal mortality. 8
This study investigated how TBAs in Sierra Leone explain, handle and prevent PPH, as well as their potential role in the management of PPH.
Worldwide training programmes of TBAs started in the 20th century. In 1952 UNICEF began to hand out ‘birth kits’ to TBAs (containing material such as surgical scissors and clamps, ligatures for the umbilical cord, a kidney dish, a Pinard stethoscope, towels, an apron, soap and a brush, a disinfectant, eye drops and a mucus aspirator for the newborn). 9 Training programmes and the distribution of birth kits took place in Sierra Leone as well. 10 Mainly between the 1970s and the 1990s the training of TBAs was a World Health Organization (WHO) supported intervention to improve maternal and neonatal health. Based on research that indicated that this intervention alone did not contribute to reduction of maternal mortality 11 the enthusiasm of WHO about training programmes for TBAs started to decrease. Instead the focus changed to implement skilled care, with officially trained health professionals for all women during pregnancy delivery and post partum. 12
Other studies continued to conclude that TBAs should be included in clinical practice and in research. A meta-analysis published in 2011 showed that the integration and the support of TBAs may significantly reduce perinatal and neonatal deaths. In maternal mortality the incorporation of TBAs showed a non-significant reduction. 13
Tradition, rituals and cultural habits play an important role for much of the population, especially in rural areas. A positive interaction between modern empirical/evidence-based medical practice and the traditional approach is lacking. Jambai and MacCormack explain this as relating to insufficient appreciation and respect of the TBAs by the official medical staff and vice versa. 14
Using PPH as an example, this study aimed to explore if a positive interaction between traditional and modern obstetrics could improve maternal health in Sierra Leone.
Methods
The collection of data took place between October and December 2010 in urban (Freetown, Bo City) and rural areas (Bo District, Kambia District, Moyamba District) of Sierra Leone. The primary research tool was a semi-quantitative questionnaire about the causes of PPH and therapeutic and preventive measures. The tool was applied to a sample of 140 participants, women aged 18–70 years who were attending deliveries in Sierra Leone. They were divided into the following subgroups: (A) TBAs with training – TBAs who at least once attended a training course by the government or a non-governmental organization (n = 48); (B) TBAs without training – TBAs with no official contact to modern obstetrics (n = 82); and (C) officially trained birth attendants (n = 10), as a small comparison group, representing the reality of modern obstetrics in Sierra Leone.
The questionnaire was filled out in single, double and group interviews. The questions were asked in English and translated by native speakers of the various local languages.
As an early sign of a significant haemorrhage includes tachycardia, 15 we included the question if the pulse of the bleeding patient was checked. Blood loss is known to be frequently underestimated. 16 This well-known fact prompted us to include the question about the measurement of blood loss. In most cases, the participants had the opportunity to select more than one option. Some of the questions were open-ended questions (e.g. reasons for PPH). The answers of these questions were categorised using a method of qualitative analysis. In a majority of the closed questions, the participants were asked to specify their answers (e.g. change of body position – which position?). These specifications were also clustered and quantified. Not all questions were answered by all participants. The number of participants responding to each question (n) is included in the chapter of results and in the tables.
In addition to the questionnaire, the participants were asked to demonstrate the manoeuvres that they apply in PPH (Figure 5). The fact that 63% of the participants were not able to read and write justifies this approach.
Results
Explanations for PPH. Total number of participants in this question: 124.
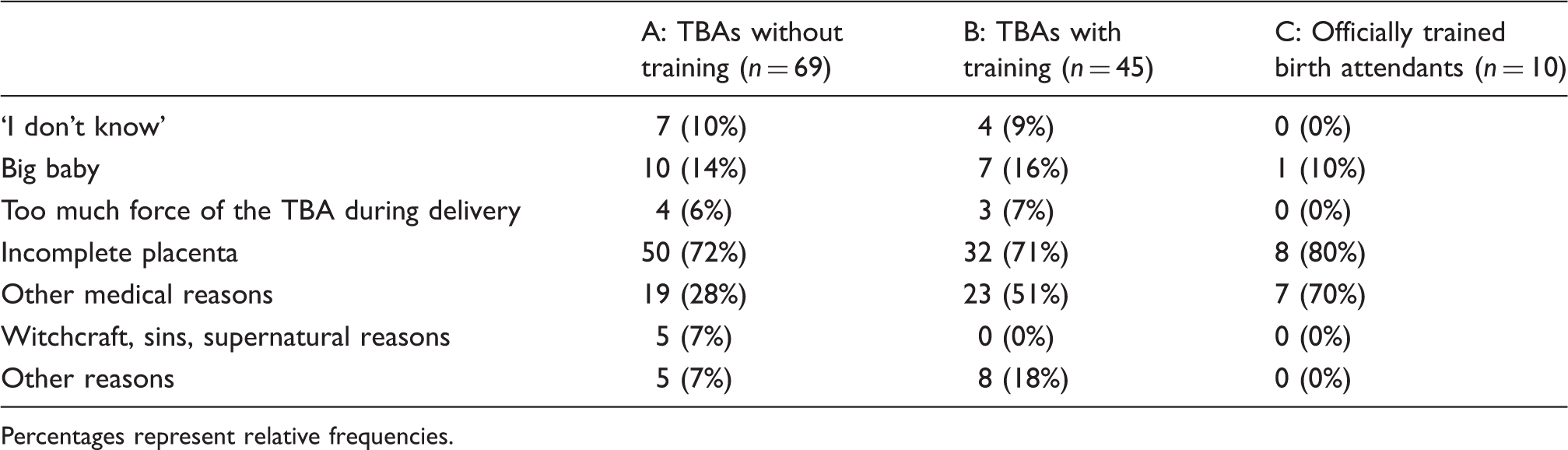
Percentages represent relative frequencies.

Rural non-trained TBAs present how they would change the position of the patient in PPH- the patient would be rolled to the side, with the feet slightly elevated.

TBAs with official training present how they would change the position of the patient in PPH- the patient would have the legs elevated.
Measures in PPH.
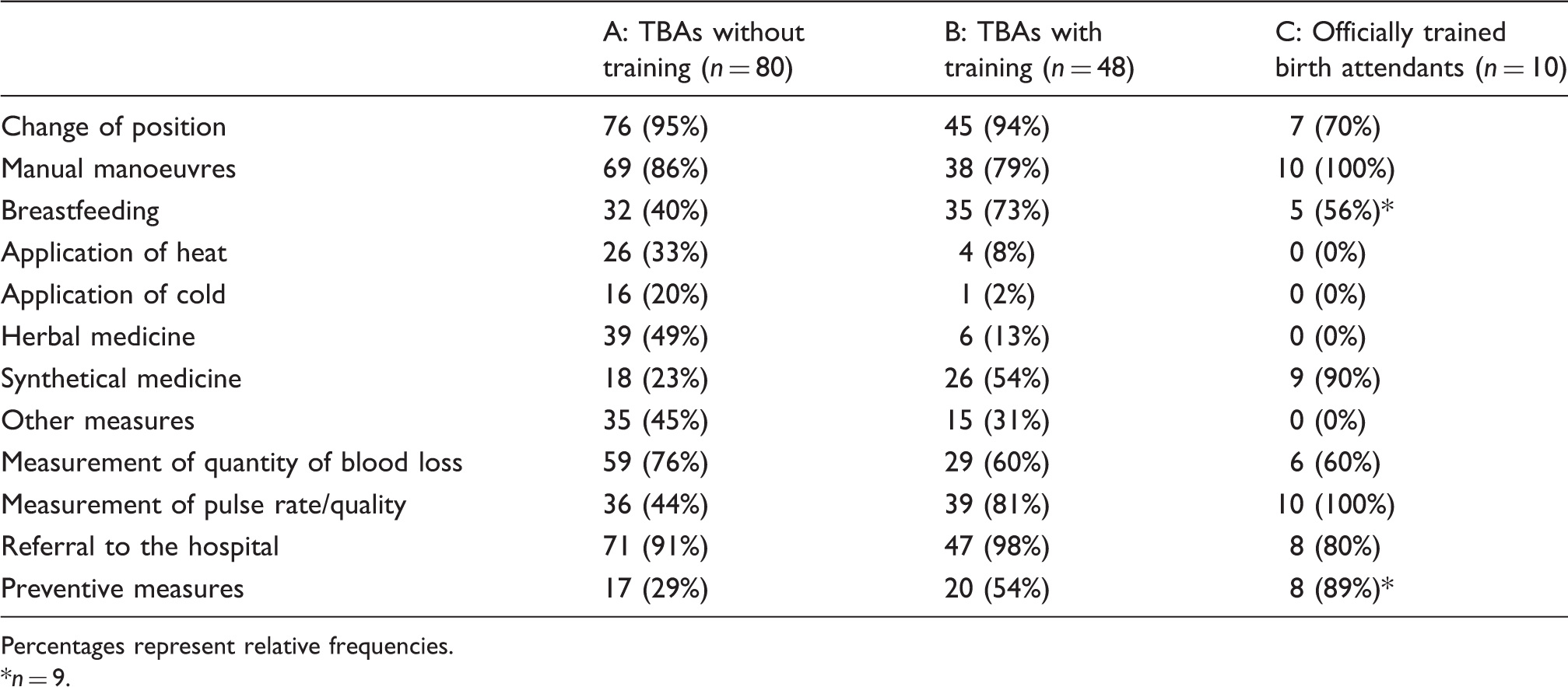
Percentages represent relative frequencies.
n = 9.

Rural non-trained TBAs present how they would apply a uterine massage with a mix of herbal medicine.
A majority of group C attempted to measure the amount of blood loss (60%, 6/10), whereas majorities of group A and B did not (70%, 88/126). Those participants who attempted to measure blood loss were asked to provide a detailed response. In descending order they explained the following measures: counting the number of pieces of cloth that were soaked with blood; counting the number of times the patient needed to be washed of blood; and measuring the amount of blood loss with a cup.
The patient’s pulse was checked by all the members of group C (100%, 10/10) and a majority of group A (81%, 39/48), whereas only 44% (36/82) of group B had their pulse checked. The participants were asked to demonstrate how to check the patient’s pulse. We defined the presentation of a superficial artery (such as the radial or the ulnar artery) using any finger except of the own thumb as the correct technique. Using this definition the majority of groups A and B (86%, 30/35) did not check the pulse correctly (Figure 4), whereas 78% (7/9) of group C presented it correctly. Additionally it is important to mention that none of the TBAs was using a watch to count out the rate. It was a rather ‘qualitative’ measurement with the resulting categories ‘faster’ or ‘slower’ than the normal pulse rate. Speaking about these changes in the pulse in PPH a majority of all participants said that the pulse after blood loss was faster (39%, 26/67) and weaker (42%, 28/67), respectively. However, there were participants of all three subgroups who were convinced that the patient’s pulse rate became slower (16%, 11/67) or ceased completely (4%, 3/67).
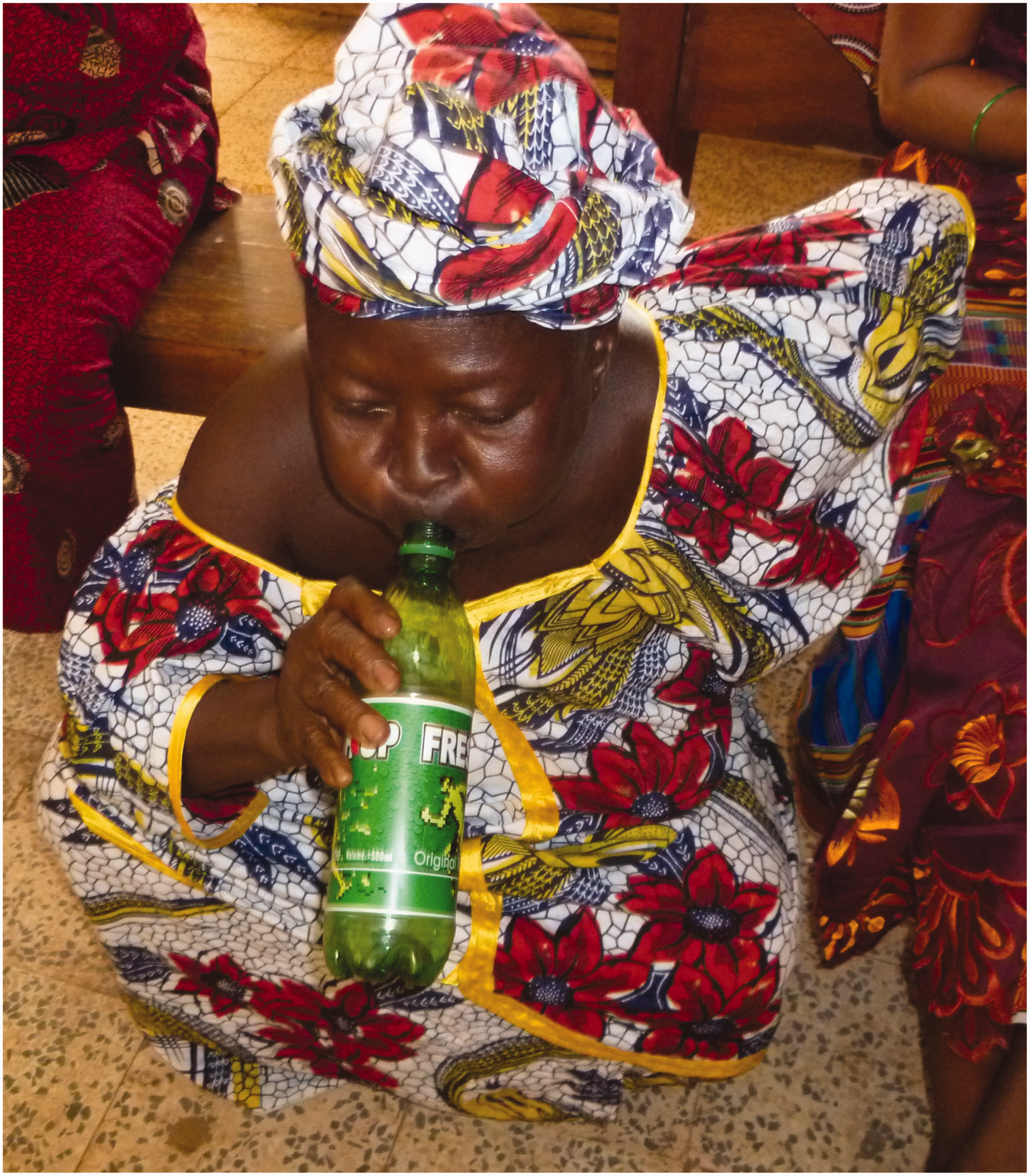
TBAS (without official training) present how they check the pulse. A TBA presents what she does, if the placenta does not come in time: she lets the mother blow in a bottle.
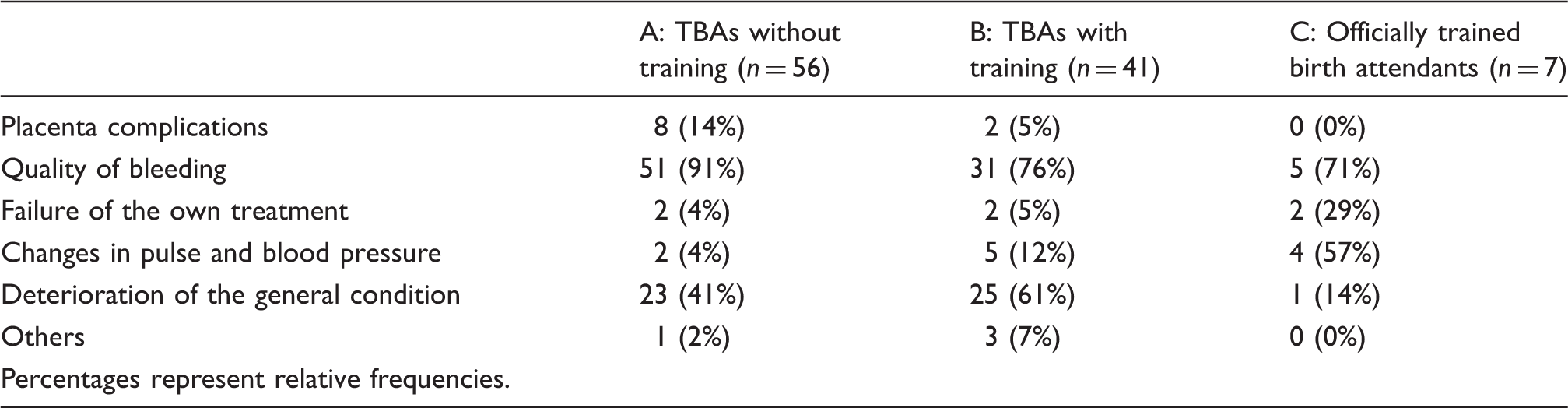
Decision to refer in PPH. Total number of participants in this question: 104.

TBAs present how they would apply a uterine massage if the placenta does not come out.
A majority of group A (54%, 20/37) as well as a majority of group C (89%, 8/9) claimed to take preventive measures for PPH. Of group B only 29% (17/58) did so. Twenty-three percent of group A (11) and 29% of group B (24) did not answer the question, which the authors hypothesized that the term prevention was not well understood. The participants who took preventive measures were asked to describe the measures. Group A and B (90%, 27/30) reported that the most important way to prevent PPH was to avoid excessive force during delivery (such as massive fundal pressure), followed by crossing the legs of the parturient after delivery of child and placenta (83%, 25/30) and the application of non-herbal medicine (83%, 25/30) such as oxytocin. In TBAs the latter answer seemed to be a theoretical one only as they neither have an official access to the drug oxytocin nor a fridge to store it adequately. The cooling of the drug oxytocin is not only a problem for TBAs but also for the officially trained birth attendants as steady electricity is very unreliable even in the biggest hospitals of the country. Besides the application of non-herbal medicine, members of group C explained various preventive measures such as active management of the postpartum period including: controlled cord traction, examination of placenta for completeness; cautious care of those patients with previous history of PPH; frequent emptying of the urinary bladder; effective monitoring of the delivery process (dilatation of the cervix and descending of the child); and effective perineal protection.
Discussion
Using the algorithms for PPH of modern obstetrics as a benchmark there appeared to be several gaps in knowledge of TBAs. The participants were not able to describe many preventive measures. The measurement of the patient’s pulse rate did not play a role or was not performed correctly by non-trained TBAs. The blood loss was not quantified. TBAs tended to describe the severity of bleeding in a more phenomenological way (‘bright red bleeding’, ‘bleeding like a tap’) than in accurate quantities. Heat in the form of hot clay was applied. Herbal medicine was applied. There is limited research literature relating to herbal medicine use for PPH in Sierra Leone. Harmful practices such as provoking the pharyngeal reflex with a wooden spoon in placenta retention are still common. Metaphysic convictions such as ‘seeing sins of the mother’ as a reason for PPH remain present in Sierra Leone. This conviction might be a factor in delayed or overdue referral of bleeding patients by their TBAs and relatives to official health institutions and would benefit from additional research.
However there did appear to be similarities between modern and traditional obstetric practices. This was especially true for manual measures such as uterine massage or compression.
The responses of TBAs with versus without training showed that the training courses appeared to have had an impact. For example the recommendation to breastfeed in the postpartum period and specifically in PPH was probably included as a modality in training courses, which have tried to make optimal use of the available options to the TBAs in the rural home setting, however this measure did not show to have a significant effect on PPH. 17
Numerous obstacles to managing PPH in Sierra Leone are present to stakeholders of modern obstetrics as well: The lack of material and medicine could be a factor in additional to training deficiencies. Misuse of medicine was observed. The single officially trained participant was only able to provide us partial fragments of the algorithms for PPH of modern obstetrics. As a result of war and poverty, the infrastructure to refer a patient with PPH from health centres to the next level of care is lacking in Sierra Leone. Even if patients reach hospital in time, the institutions are often lacking resources to meet the obstetric emergency of PPH successfully.
The high maternal mortality is multifactorial and should not only be attributed to traditional obstetrics. It may not be possible to eliminate traditional obstetrics from birthing customs in Sierra Leone, but there may be an opportunity to include traditional customs into health programmes. The participating TBAs seemed highly motivated to improve their knowledge and to contribute to an improvement of maternal health in their country. As a consequence of this research we propose the integration of TBAs in research programmes and particularly in the care for the pregnant, delivering and breastfeeding mothers which is already implemented in other countries in West Africa. Various approaches exist. One study in neighbouring Liberia evaluated the outcome of a teaching programme called ‘Home-based Life-saving Skills’ in four life-saving measures in obstetrics. This study found a major change in the knowledge base of the traditional and trained traditional midwives in the evaluation and re-evaluation of the programme. 18 In Gambia a double-blind randomised controlled trial was conducted about misoprostol in the management of the third stage of labour in the home delivery setting. 19 . The usage of misoprostol is a promising tool in the home delivery setting in low resource countries as concluded in a systematic review. The distribution through first line health workers could help in reducing maternal deaths as misoprostol is an inexpensive drug which does not need cold chain storage. 20
A review published in 2011 concluded that skilled birth attendance increases as TBAs are integrated into the health system. 21
Improvement of the formal health sector in Sierra Leone would, we believe, benefit from a combined approach including integration of traditional practices into health programmes. There is further research opportunity to evaluate the implementation and outcome of such programmes.
Current developments
The dramatic outbreak of the Ebola virus disease in West Africa has profound consequences for all health services as there is a climate of discrimination and fear. Many health workers were already infected. 22 We were informed that in Sierra Leone healthcare workers and patients avoid healthcare services as they are afraid of infection. This crisis of the health system existentially affects maternal and neonatal health.
It is possible that the Ebola outbreak and its secondary consequences will increase the influence and importance of TBAs again as they work independently of the official health system. They are used to work with less material and infrastructure. Thus they are more flexible to react to external changes. This principle was already observed during the civil war, when the official health care services collapsed as well. 14
Nevertheless we hope that the national and international responses to the Ebola crisis succeed in controlling the outbreak and that the healthcare services recover fast.
Footnotes
Acknowledgments
We acknowledge the support received from colleagues at the Sierra Leone MoHS, and the Centre for Scientific Research into Plant Medicine (CSRPM) in Ghana, the World Health Organization and the Non-Governmental Organizations EMERGENCY, Amnesty International Sierra Leone and the AG FIDE (Women’s Health in International Development).
Conflict of interest
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.