
Abstract
The milky sap of the Euphorbia plant is highly toxic and causes inflammation to the skin and eyes. Damage to the eye ranges from superficial epithelial defects, keratoconjunctivitis, mild to moderate corneal edema, anterior uveitis, Descemet membrane folds, raised intraocular pressure and rarely corneal opacity in severe untreated cases. Here we report a case of visual restoration by optical penetrating keratoplasty in a patient with severe corneal opacity following exposure to Euphorbia latex.
Introduction
Euphorbia is a genus of plants belonging to the family Euphorbiaceae. The Euphorbiaceae family includes trees, succulents and herbaceous plants. Different species of Euphorbia grow all over the world. 1 The milky latex or sap causes intense inflammation of the skin and the eyes. Ocular toxic reaction varies from mild conjunctivitis, corneal oedema, kerato-uveitis to severe corneal opacification in untreated cases. There are a few case reports of permanent blindness resulting from accidental inoculation of Euphorbia sap into the eye.2,3 Ocular toxicity can be caused by different species of Euphorbia, namely, E. trigona (African milk tree), E. neriifolia (Indian Spurge tree) and E. milii (Crown-of-thorns houseplant). The other species of Euphorbia causing ocular toxicity reported are mostly with E. royaleana, E. lathyris and E. tirucalli.2,3
Case report
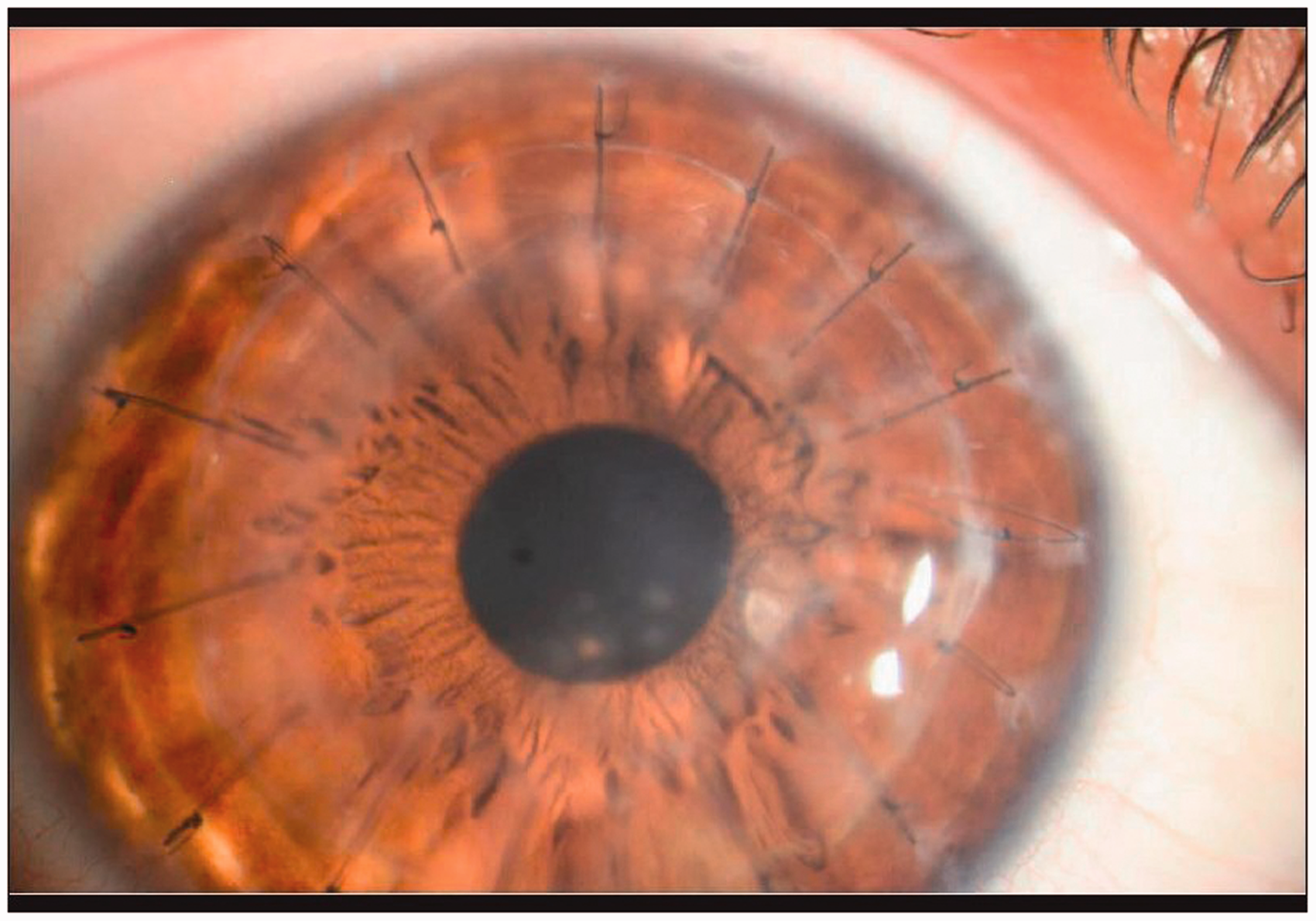
We present here a case of ocular toxicity in a 35-year-old woman with loss of vision in her right eye who presented to our outpatient department in July 2013. She gave a history of exposure to Euphorbia latex 8 months previously in her right eye while working in the garden. After the initial exposure, she had experienced intense burning with acute congestion, redness and watering associated with photophobia. Her vision and cornea were normal prior to her exposure to the latex. She was treated by a local traditional doctor with oral medications to reduce pain and there was gradual decrease in her vision following the acute episode. On examination her best corrected visual acuity in the right eye (OD) was hand movement close to face. Her left eye (OS) was normal. Slit lamp examination showed total corneal opacification with 360° superficial and deep corneal vascularisation in OD (Figure 1). No underlying iris details were visualised. Optical penetrating keratoplasty (PKP) was planned. PKP was performed from a suitable donor cornea 1 week later. Postoperative topical prednisolone acetate, moxifloxacin and cycloplegic drops were used. The patient also received 60 mg of oral prednisolone to improve graft survival. She was followed up at weekly intervals initially for 2 months and later bimonthly for the last 6 months. Both systemic and topical steroids were gradually tapered off. She was last examined on April 2014 and her best corrected visual acuity was 20/60 unaided with proper retention of the corneal graft, good graft clarity and normal intraocular pressure (Figure 2).
Right eye showing corneal opacification with neovascularisation. Six months postoperative photo showing clear corneal graft.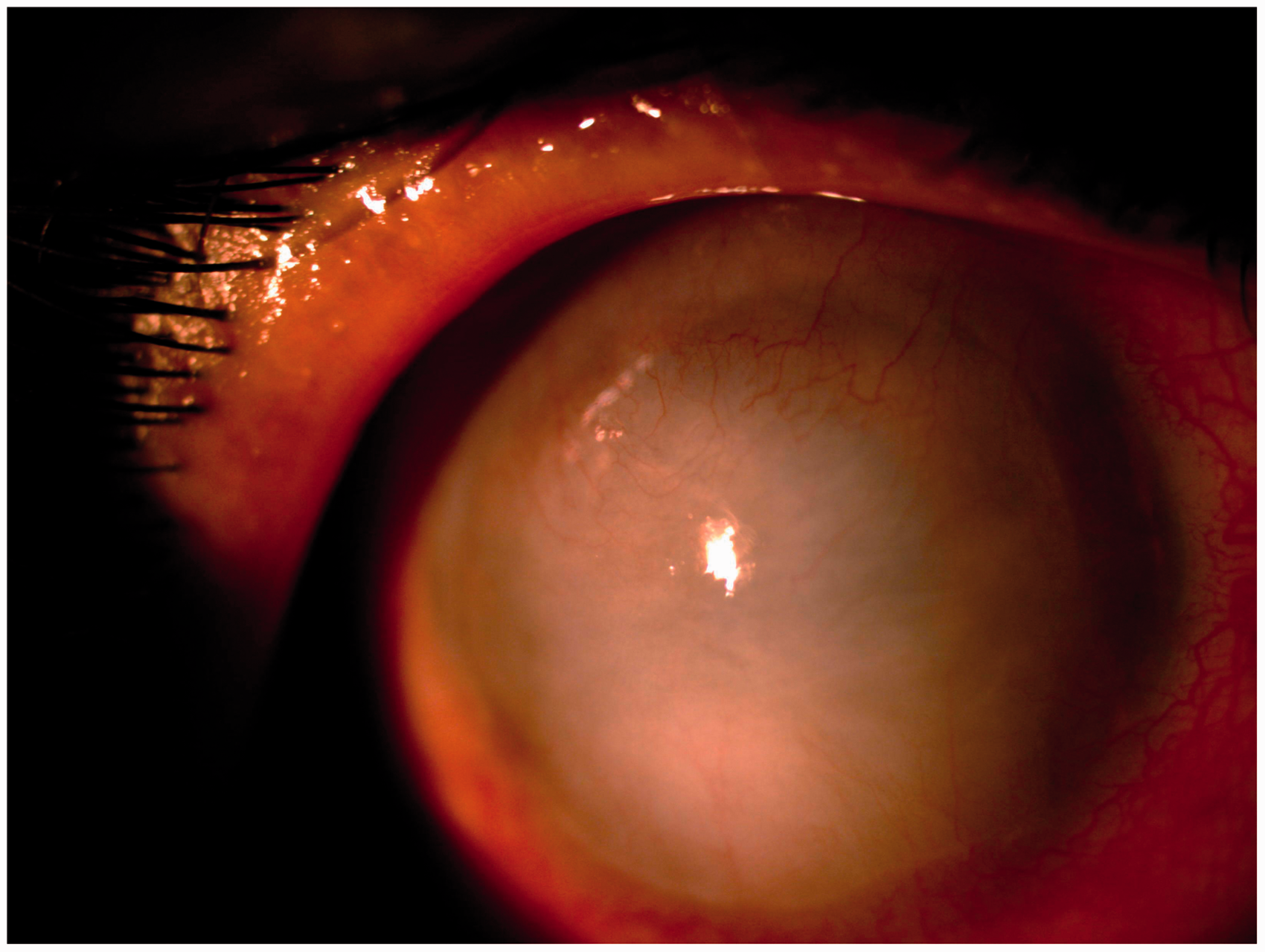
Discussion
Euphorbia keratopathy is reported in several case series from all around the world but this work is a rare report of severe corneal opacification from inadvertent exposure to the sap of Euphorbia that has been treated with optical PKP. Euphorbia is a diverse plant genus consisting of more than 2,000 species with worldwide distribution, chiefly in subtropical and temperate regions. The toxic variants are mostly found in India, Southern Africa, Madagascar and North America. The toxicity is variable between and within genera and species. Some species have no apparent ill effects on the eyes, while the others may cause the same clinical pictures with variable severity. The severity of ocular inflammation may be related to the species of plant, the concentration of sap into the eye and the duration of contact. The main phytochemical substances in the latex are di- or tri-terpene esters, pyrrogalic and catechuic tannins, and the alkaloid xanthoramnine.4,5
Symptoms usually start immediately on contact with the milky latex. There is a burning sensation, pain, photophobia and lacrimation. At first, there is mild diminution of vision, but this may diminish further to 20/200 or counting fingers to hand movements. Neglected cases can progress to blindness due to corneal scarring. 6 In the described case dense corneal opacity and neovascularisation was observed. Optical penetrating keratoplasty was the only viable option in this case to restore vision. The success of operation in our case was that the active corneal pathologies had resolved and the patient had been followed up regularly. The patient was evaluated at every visit by detailed slit lamp examination of corneal graft and anterior chamber to rule out any onset of graft failure.
Conclusion
Although Euphorbia keratopathy seems to be self-limiting when managed supportively, it is important to remember that blindness can occur, particularly in neglected cases. Pharmacologic therapy is aimed at minimising inflammation in majority of cases but surgical therapy may be required to restore vision in rare neglected cases.
Footnotes
Declaration of conflicting interests
None declared.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.