
Abstract
Spontaneous perforation of pyometra is a rare entity with a reported incidence in the range of 0.01–0.05%. The clinical picture is similar to peritonitis arising from intestinal perforation and commonly the correct diagnosis is only made perioperatively. We report a case in an elderly postmenopausal woman presenting with an acute abdomen.
Case report
A 60-year old postmenopausal woman, Para 10, presented with lower abdominal pain for the previous 7 days, together with frequent bilious vomiting for the previous 2 days, and an acute onset of abdominal distension and obstipation on the last day. There was no history of fever, postmenopausal bleeding or discharge per vaginam. She was a chronic tobacco and bidi (smoked 3 bidis/day for 15 years) smoker. On examination, she had a tachycardia (pulse rate 110/min) and was mildly hypotensive (blood pressure 100/60 mmHg). The abdomen was distended with generalised guarding; scanty bowel sounds were heard. An erect chest radiograph demonstrated gas under the diaphragm. An abdominal ultrasound scan revealed a moderate amount of free fluid with internal septations and non-peristaltic bowel loops. A provisional diagnosis of peritonitis due to gastrointestinal perforation was made and the patient was submitted to an exploratory laparotomy.
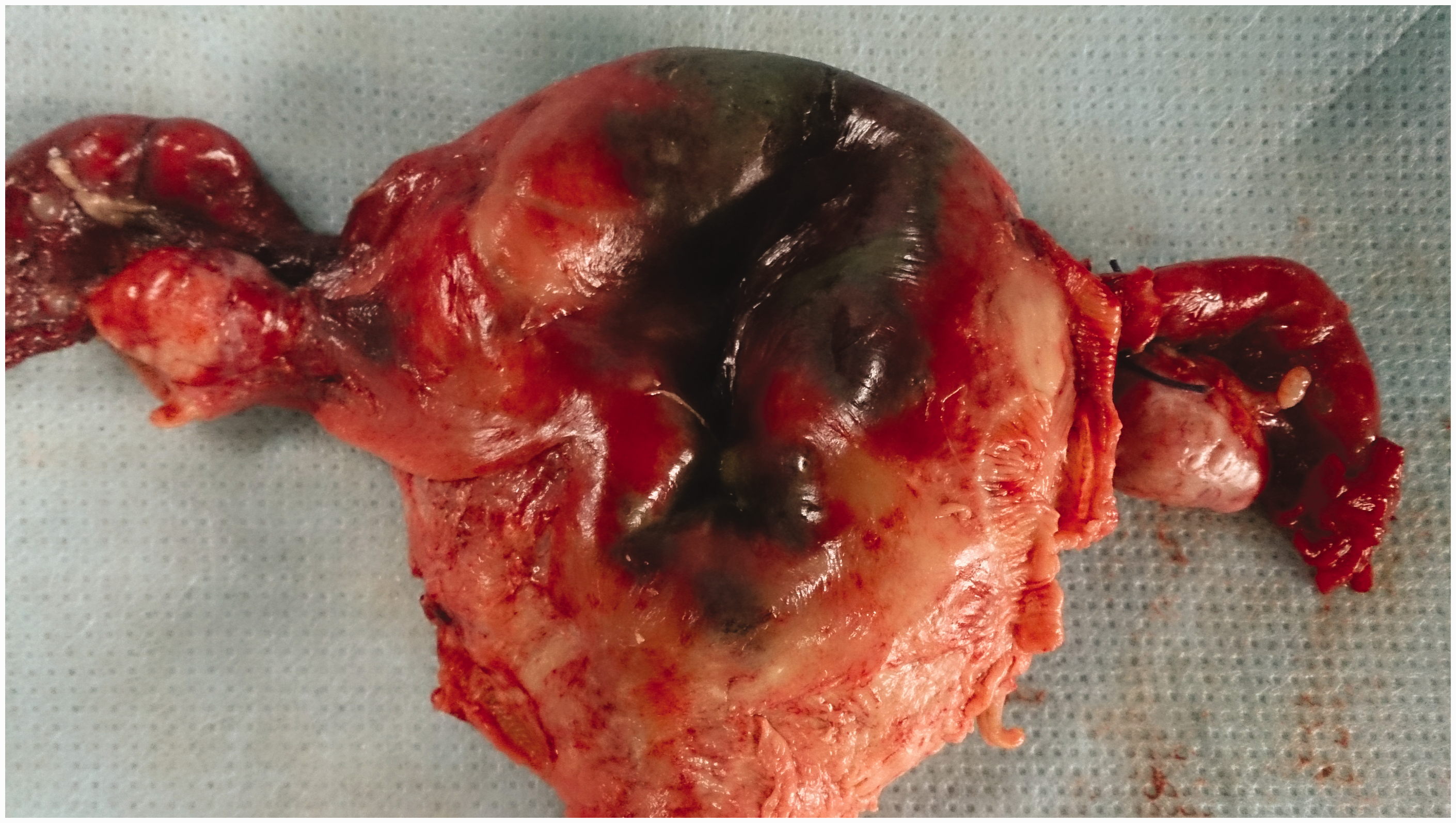
Perioperatively, circa 1 L of pus was found in the peritoneal cavity. An extensive peritoneal lavage was carried out, but no gastro-intestinal perforation was found. Purulent fibrin was adherent throughout to bowel, omentum and mesentery. The uterus was approximately 8–10 weeks’ size, soft in consistency with a gangrenous patch seen at the fundus. On its posterior aspect, there was a 1 × 1 cm rent, through which frank pus was oozing. A total abdominal hysterectomy with bilateral salpingo-oophorectomy was thus performed. Cut section of the uterine specimen revealed a gangrenous purulent endometrium (Figures 1 and 2). Histopathological examination described an atrophic endometritis and cervicitis.
Cut section of the uterus-anterior aspect showing pyometra. Posterior aspect of uterus showing gangrenous area with a rent in the fundoposterior aspect.
On the second postoperative day, the patient developed diabetic ketoacidosis and was commenced on an insulin infusion, but subsequently developed pulmonary oedema, uncontrollable blood sugar levels, acute renal failure and a burst abdomen. Despite haemodialysis, and 1 month in intensive care, she ultimately died from multi-organ failure. The pus grew Staphylococcus aureus, sensitive to teicoplanin.
Discussion
Pyometra is collection of pus in the uterine cavity, resulting from impairment of natural drainage via the cervix. Benign or malignant tumours of the cervix or uterus, radiation cervicitis, atrophic cervicitis, trauma to cervix, infection and congenital abnormalities of genital tract can all result in cervical occlusion leading to pyometra. 1 It is also a rare complication of endometrial ablation, often necessitating hysterectomy. 2 The reported incidence of pyometra ranges from 0.5% in young premenopausal women and increases to 13.5% in elderly postmenopausal women. 3 The classic triad of pyometra includes lower abdominal pain, discharge per vaginam and postmenopausal bleeding. However, half of all cases remain asymptomatic. 4 Symptoms may be non-specific resulting in delayed or even missed diagnosis and subsequently increased probability to perforation of such a pyometra, if not detected at its early stages. Frequently, the correct diagnosis is only made at laparotomy. The clinical picture of a perforated pyometra often mimics intestinal perforation. A transvaginal sonography is helpful in detecting intrauterine fluid collection, but this was missed in our case.
However, this would not have altered the therapeutic approach. If a fluid collection is detected in the uterus without perforation it is often possible to drain the uterine cavity carefully via the cervical canal with the help of a thin plastic cannula. Material obtained from the uterus in such a way should be examined for malignancy.
Pyometra and its close association with malignancy, risk of spontaneous rupture and subsequent high mortality make it a medical emergency. This differential diagnosis must be borne in mind, especially in postmenopausal women. Perforated pyometra requires prompt and aggressive treatment, by peritoneal lavage and hysterectomy.
Literature review 5 .
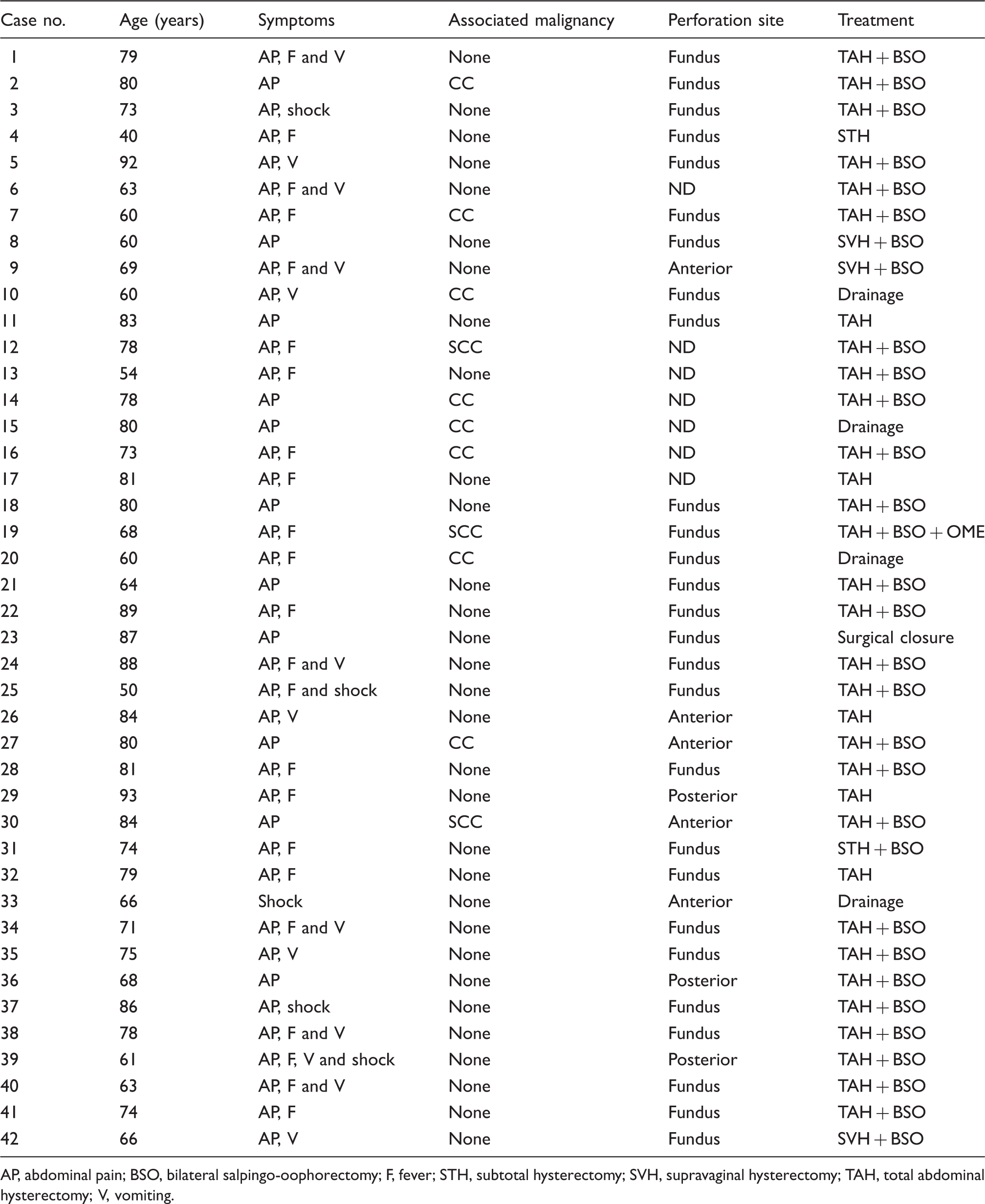
AP, abdominal pain; BSO, bilateral salpingo-oophorectomy; F, fever; STH, subtotal hysterectomy; SVH, supravaginal hysterectomy; TAH, total abdominal hysterectomy; V, vomiting.
Mortality from spontaneously perforated pyometra exceeds 40%. Sepsis must be rigorously dealt with. 6 Malignant disease is present in 35% of cases, and this is more common among diabetics, who are themselves more prone to suffer serious consequences of sepsis. 7 Although malignancy was not confirmed in our patient, it is quite possible that there was an area of endometrial carcinoma which became necrotic and hence remained undetectable by microscopy. Obviously, perforated pyometra not associated with malignancy has a better prognosis. 8
Conclusion
At emergency laparotomy for sepsis in a postmenopausal woman, perforation of a septic uterus, though rare, must be kept in mind as a source of infection. While preoperative diagnosis may be elusive, once found, rapid and radical action is necessary to save the patient’s life.
Footnotes
Declaration of conflicting interests
All the authors have seen the manuscript and approve it for submission. The authors have no competing interest in the publication of the manuscript to declare.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.