
Abstract
Objective
The aim of this study was to describe and define an outbreak of human anthrax in two villages in the northern savannah region of Togo.
Patients and Method
In December 2009, localised groups of deaths occurred among villagers and their livestock, confirmed to be due to anthrax at the district hospital of Dapaong in Northern Togo. The National Disease Control department undertook an investigation to describe the epidemiological, clinical and bacteriological characteristics of this outbreak.
Results
Thirty-four individuals presented with clinical manifestations of anthrax. All patients were known to have consumed meat from cattle who had died of unknown causes or had been killed as a result of unknown illness. All patients presented with muco-cutaneous lesions; some had gastro-intestinal, neurological or meningeal symptoms, or septicaemia. One patient was co-infected with Plasmodium falciparum. Six deaths (17.6%) were reported at the beginning of the epidemic; 28 patients were successfully treated with a 10-day course of intravenous Penicillin or oral Amoxicillin. The two factors that contributed to the ultimate resolution of the anthrax outbreak were the increase of community awareness toward health promotion and vaccination of all farm animals.
Conclusion
Although six deaths occurred among families’ members who were infected, new human anthrax cases were prevented by rapid treatment of victims as well as aggressive public health interventions. However the risk of re-emergence of infection and exposure still exists as there are no existing epidemiological mapping and no identification of infected zones; and furthermore, no functional anthrax surveillance system exists in the affected region.
Keywords
Background
Anthrax is an acute infectious disease caused by the spore-forming bacterium, Bacillus anthracis. As a spore-forming bacterium, B. anthracis can survive for decades in soil and infect herbivores during feeding. 1 Humans usually acquire anthrax through occupational exposure to infected animals or their products,2–4 but infection can also occur from exposure to an environment contaminated with B. anthracis spores.3,5,6 Inhalation of anthrax has a mortality rate of 85%, but with appropriate antimicrobial and supportive therapy, the rate should decrease to 45%.7–9 Clinical manifestations include cutaneous manifestations, septicaemia, pulmonary failure, digestive illness and neurological or meningeal lesions. 10 Cutaneous anthrax is rarely fatal if treated, but without treatment, approximately 20% of patients evolve to sepsis and death. 10
Human anthrax has been virtually eliminated in industrialised countries because of effective control measures.7,11 However, in sub-Saharan Africa, it continues to be a devastating disease, especially in rural areas where livestock farming is the inhabitants’ daily occupation and where human and animal vaccination, veterinary supervision of animal slaughtering and quality of animal products control are poor. This report is the first to detail an outbreak of anthrax in Togo. This information is indispensable in establishing rapid detection, management and prevention strategies for future anthrax outbreaks in sub-Saharan Africa.
Patients and method
Description of the epidemic
On the evening of 3 December 2009, a cattle farmer (Patient A) from Warkambou village, Togo (Figure 1) collapsed with rigors and died in his home. On 5 December 2009, two siblings of the dead farmer (Patients B and C), who had been living with the latter, collapsed with rigors while in pasture with the cattle and died in the bush. The deceased cattle farmers’ relatives reported to the chief of the village that on 25 November and 2 and 3 December, three cows from the dead farmers’ cattle died suddenly following bleeding from orifices. Farmers guarding the deceased cattle had butchered, prepared and consumed some of the dead cows’ meat, and sold the other pieces of meat at the village market. Three days following the death of the third cattle farmer, another sibling (Patient G) who also had eaten the meat, became ill and sought for medical care at the Hospital of Dapaong. He reported that he had suffered, as had the dead cattle farmers, pustules of the neck, face and trunk, a fever (≥38℃), myalgia, nausea and vomiting, with weight loss. Blood smear examination of this consulting patient revealed infection with Plasmodium falciparum. He was thus treated with Quinine and intravenous Penicillin, which resulted in a rapid recovery and discharge from hospital after 5 days.
Map of Togo and the locations of Warkambou and Pligou from where Bacillus anthracis were isolated from patients and cattle.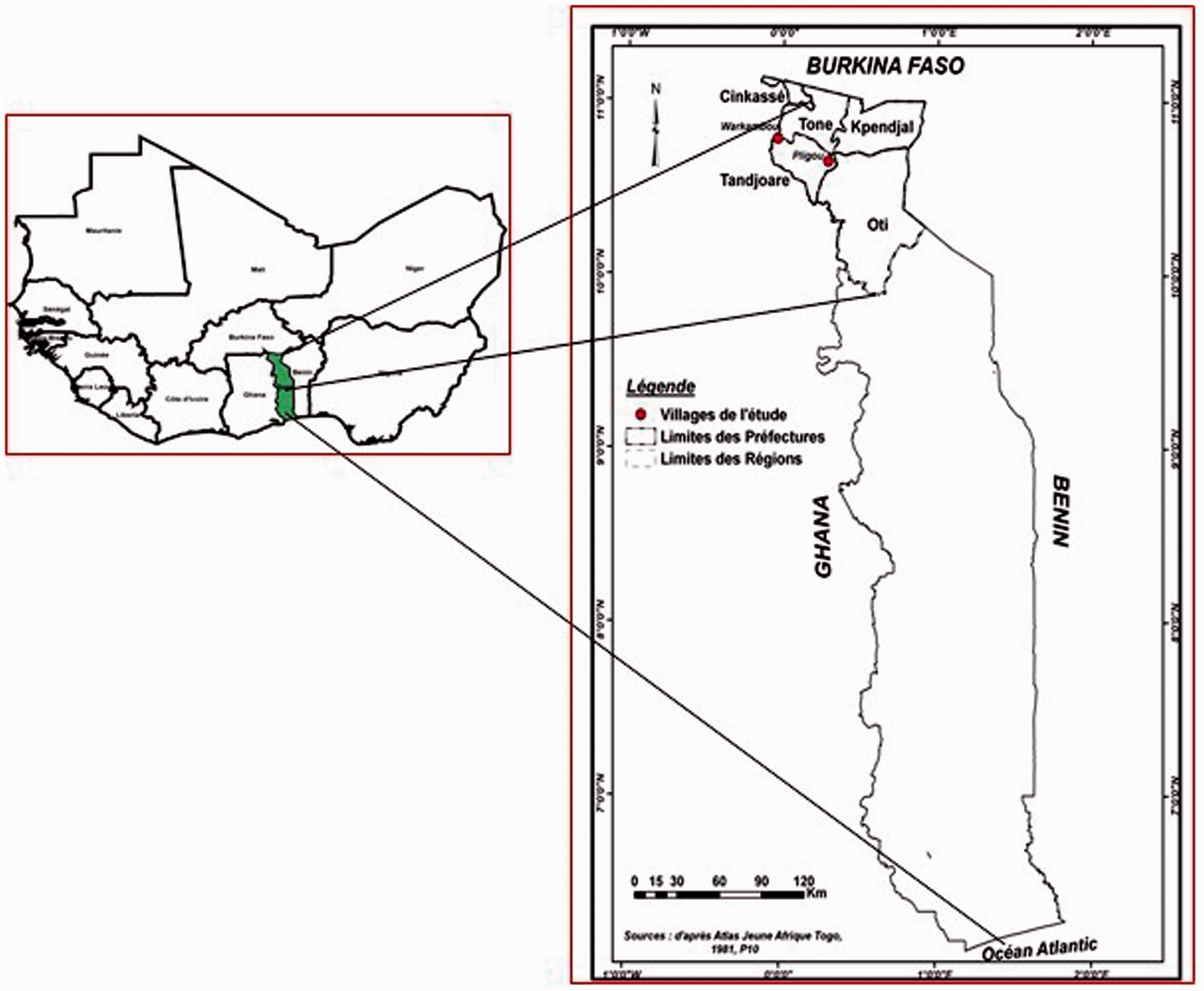
On 5, 6 and 7 December, three siblings (Patients D, E and F) from Pligou village, located 60 km northwest of Warkambou, consulted at the local dispensary because of fever, accompanied by chills, bloody diarrhoea, pustules and severe myalgia persisting for approximately 1 week. Two days later, their condition deteriorated rapidly with sepsis and haemorrhagic meningitis. All three died on the third day.
The patients’ family members reported that just before the onset of symptoms, they had consumed some cow meat they had bought at the village market, from a cow that was said to have died suddenly of unknown causes. The National Disease Control Department consequently dispatched a multidisciplinary investigation team of a physician, a veterinarian, a biologist and two nurses to the villages for further investigation.
Definition of anthrax cases
Because of the association between exposure or consumption of infected meat, 2 and the occurrence of a disease suggestive of anthrax, the investigation team suspected exposure to anthrax spores. Thus, any individual presenting with signs and symptoms suggesting anthrax-like illness such as skin lesions, digestive or pulmonary illness was considered as a suspect anthrax case. Animals or humans who had been reported to have characteristic lesions or had died in either November or December 2009 were considered as possible cases. A confirmed anthrax case was defined by the isolation or identification of B. anthracis after laboratory investigation from cutaneous brushings or a blood sample.
Specimens and diagnostic testing
Nine specimens, seven cutaneous brushings (Patients K, L, M, O, S, W and Z) and one blood sample (Patient X) were collected from those who met suspected case definition for further laboratory investigation. Specimens were taken also from some suspected animals and leftover meat in order to detect B. anthracis. Two skin specimens were taken from the family members of the first deceased in Pligou village. Additional tests such as catalase, haemolysis or phage lysis were not done.
Results
Age and sex distribution, source of contact, incubation period, clinical manifestations, sample taken and results.

iarr: bloody diarrhoea; F, female; M, male; mening: haemorrhagic meningitis; P, Pligou; Skin, skin lesions; Syst, systemic manifestations; W, Warkambou.
Patients V and AB had cut and smoked the meat but not consumed it; Patient AG presented as facial oedema and splenomegaly; Patient AH presented with ulcer on the chest wall.
A total of 34 patients presented with pustules; 19 (55.8%) had both processed and eaten infected meat, while 13 (38.2%) had only eaten the contaminated food. The remaining two patients (Patients V and AB) had cut and smoked the contaminated meat without consuming it. Their mean age was 21.3 years (age range, 4–68 years), and 62% were children aged ≤14 years. The sex ratio (male:female) was 1:3 (summarized in Table 1).
In 70% of cases, the pustules involved the arms, face and neck. One patient (AB) developed a fistulising abscess of the throat. Two of the 21 children (Patients O and S) presented with cutaneous lesions of the feet, from which specimens were obtained. One 60-year-old patient (AF) had a single papule of the right flank. In one 11-year-old child (Patient AG), the disease presented as facial oedema and splenomegaly. A 47-year-old woman (Patient AH) presented with an ulcerated scarified lesion, covered with a black crust, of the anterosuperior left chest wall (Figure 2). Seven patients (20.6%) developed sepsis. There were five cases (14.7%) presented with diarrhoea. No evidence of respiratory symptoms was noted among the patients investigated.
Ulcerated scarified lesion, covered with a black crust, of the anterosuperior left chest wall.
Of the 28 survivors, 22 (75%) were treated with parenteral penicillin, and six had oral amoxicillin for a period of 10–14 days. In 75% of cases, skin lesions had significantly improved or resolved by the fifth day of treatment.
The outbreak was declared over on 31 January 2010, approximately 35 days following the diagnosis of the last anthrax case.
Discussion
The complete and rapid control of this anthrax outbreak was successful due to the aggressive and rapid measures taken, which included: (1) reinforcement of sanitary practices; (2) public education and awareness of the illness within the surrounding communities; (3) all animals that had died or were sick in the period were considered potentially infected and their meat systematically isolated; (4) prohibition of the sale of all meat, milk products and animal skins at all local markets for 1 month before and after the animal vaccination programmes; (5) vaccination of 4764 goats and cattle with Anthracin vaccine (lot 192), Bamako Central Laboratory; and (6) free treatment of all infected or exposed patients.
As the result of a combination of factors including: (1) the epidemiological association between anthrax and handling and/or consumption of infected meat; (2) the evolution and recognition of resultant clinical symptoms of disease; and (3) the isolation of B. anthracis in samples taken from infected humans and animals, it was possible to confirm the diagnosis of anthrax in Pligou and Warkambou in the northern region of Togo with confidence. The transmission of anthrax infection via muco-cutaneous and/or oral-digestive route is typically found in epidemics characteristic to sub-Saharan Africa.13–16 This is in contrast to the mode of transmission recently reported in the USA and Europe, following heroin injection.17,18 The clinical spectrum of the disease in this report is similar to those reported in Zimbabwe 11 and Gambia. 13
In the absence of antibiotic sensitivity testing, the antibiotic of choice is considered to be parenteral penicillin as most patients had the cutaneous form of the disease. This antibiotic has low cost and therefore easy affordability; an additional advantage of intravenous administration is that it allows closer monitoring and observation of patients. No prophylactic program of antibiotic administration was recommended or performed in the two villages.
This anthrax outbreak had two particular and notable features, namely the time period of appearance of the disease and the impact of heightened communication within the community. The outbreak occurred at the beginning of the dry season, concomitantly in two different places, separated by a distance of 60 km. There is no transport connection between these two communities, as there is neither road nor river that connects them. No known transport or migration of animals had occurred either. However the sale of sick animals or contaminated meat from one village to another could not be completely excluded.
Another consideration is that the anthrax may have been spread by migratory bird vectors, such as birds of prey or vultures, as was the case in Gambia. 13 In addition, in August 2007, the savannah region in northern Togo experienced severe flooding that resulted in the loss of considerable human and animal lives. According to oral reports, there were reports of cases of anthrax in these regions. Thus, the flooding could have created conditions favourable to the emergence, dissemination and contamination of vegetation and watering holes used by grazing animals by anthrax spores.
Until this epidemiological study was carried out, there was no prior isolation mapping done in these uncharted areas. This is important as it suggests a risk of re-emergence of anthrax in the future especially given the long viability of anthrax spores. It is imperative that continued vigilance as well as veterinary and clinical surveillance be reinforced in the regions where animals are farmed and agricultural activities continue.
Footnotes
Acknowledgements
The authors thank Dinnye Kombaté-Noudjo and Eyaba Tchamdja for their help in the control of this anthrax outbreak.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.