
Abstract
Hyperuricaemia in type 2 diabetes mellitus (T2DM) has been less well investigated in sub-Saharan Africans. Our study of 438 patients found that alcohol intake, body mass index ≥25 kg/m2, hydrochlorothiazide use, statin use, diabetic retinopathy and glomerular filtration rate <60 mL/min/1.73m2 were independently positively associated with hyperuricaemia; whereas smoking reduced this risk. Hyperuricaemia is strongly associated with some modifiable factors, diabetic complications and certain drugs. Our results suggest that further studies should evaluate the potential cost–benefit of screening for hyperuricaemia in type 2 diabetes.
Introduction
The burden of type 2 diabetes mellitus (T2DM) is increasing alarmingly worldwide, especially in sub-Saharan Africa (SSA). 1 This disease often occurs as a feature of the metabolic syndrome (MS), a cluster of cardiovascular and metabolic conditions that have insulin resistance as the underlying mechanism. 2 Hyperuricaemia, an increase in serum uric acid levels above the normal range, has been described as a component of MS, 3 although its clinical importance is often overlooked.
The relationship between hyperuricaemia and T2DM or its chronic complications has been explored in the recent years. Wang et al. found a prevalence of 32.6% in 2917 Chinese patients with T2DM and central obesity. 4 Also, a recent meta-analysis of nine studies including 20,891 T2DM patients from Asia, Italy and Australia revealed that elevated serum uric acid (SUA) was an independent predictor of vascular complications and cardiovascular mortality in T2DM patients. 5 However, this meta-analysis did not include any study from sub-Saharan Africa. In 2010, Ogbera et al. reported a 25% prevalence of hyperuricaemia in 601 Nigerian patients with T2DM. 6
The potential mechanism that links hyperuricaemia to T2DM and its complications is unclear, but it has been suggested that insulin resistance causes a decrease in urinary excretion of uric acid. 2 Uric acid may cause endothelial dysfunction by inhibiting the bioavailability of nitric oxide,7–9 and monosodium urate can cause an inflammatory reaction by triggering the activation of cytokines and liberation of interleukin-1 (IL-1). 10 These put together may in turn worsen diabetic vascular complications. Hyperuricaemia is therefore strongly associated with T2DM and constitutes an additional burden. However, data on this association are scarce among sub-Saharan Africans. The aim of our study was to investigate the prevalence of hyperuricaemia and look at its associations in a group of type 2 diabetic patients in Cameroon.
Patients and methods
After ethical approval (reference no. 53) from the Institutional Review Board of the Faculty of Medicine and Pharmaceutical Sciences, University of Douala, we conducted a hospital based cross-sectional study at the Diabetes and Endocrine Outpatient Unit of Douala General Hospital (DGH).
Diabetic patients receiving care provided by specialists in this unit undergo an annual check-up that includes: clinical assessment, evaluation of diabetes control, and screening for chronic complications and cardiovascular risk factors. All consecutive type 2 diabetic patients who were attending for their annual assessment during the study period were invited to participate. Uric acid analysis was done as a free-of-charge additional assessment to the standard tests. No refusal was registered; pregnant women were excluded.
The sample size was estimated using the Cochran’s sample size formula. Using prevalence of 25% of hyperuricaemia in type 2 diabetic patients obtained in Nigeria by Ogbera et al. 6 as reference, the minimum required sample size was 288.
A trained sixth-year medical student collected the data on a pretested data collection form and did the measurements, under the supervision of the principal investigator. Data were collected on medical history, lifestyle (diet, smoking, physical exercise and alcohol consumption), drug history, anthropometric and vital parameters (weight, height, body mass index [BMI], waist and hip circumferences, and blood pressure).
Biochemical assessments were performed with a Roche-Hitachi Cobas C311® analyser (Roche Diagnostics GmbH, Mannheim, Germany; Hitachi High-Technology Corporation, Tokyo, Japan) using the colorimetric method for fasting serum uric acid, the immune-turbidimetric method for glycated haemoglobin (HbA1c), the enzymatic method for fasting total cholesterol, high density lipoprotein cholesterol and triglycerides, and the Jaffé method for fasting serum creatinine. Low density lipoprotein cholesterol was calculated by the Friedwald formulae, and the estimated glomerular filtration rate (eGFR) was calculated by the Cockroft–Gault formula.
Retinography and angiography (when indicated, if retinography could not provide the final diagnosis) were performed using a TOPCOM® MARKII Retinal Camera (TOPCOM Corporation, Tokyo, Japan).
The diagnosis of diabetes was based on the 2009 American Diabetes Association diagnostic criteria. 11 For our study purposes, we defined hyperuricaemia as serum uric acid level greater than 7.0 mg/dl for men and 6.0 mg/dl for women. Metabolic syndrome was defined according to the criteria of the National Cholesterol Education Program Adult Treatment Panel III. 12 Chronic kidney disease (CKD) was defined as eGFR <60 mL/min/1.73 m2.
A history of nephropathy was defined as any report of dipstick proteinuria or microalbuminuria with or without any decrease in eGFR.
Alcohol drinking consisted of history of drinking any alcohol beverage independent of its type and frequency of intake. It was further sub-categorised as: rare drinking (less than weekly); occasional drinking (weekly); and regular drinking (drinking daily). Smoking was defined as any history of cigarette smoking independent of its quantity and duration. We considered regular physical activity as report of participation in more than 30 min of moderate or vigorous intensity activity per day for at least 3 days per week.
Statistical analyses were performed using STATA version 11.0 software (StataCorp, College Station, TX, USA). Continuous variables were compared between the groups using independent sample t-test, and expressed as mean (standard deviation [SD]), whereas proportions were compared using a two-sample Z test. Bivariate analysis was used to identify factors associated with hyperuricaemia and presented as odd ratio (OR) with 95% confidence intervals (CI). All variables that were significantly associated with hyperuricaemia in bivariate analysis were forced into a multiple logistic regression model. These variables were first used to generate a correlation matrix and when a pair was significantly correlated (P < 0.05), one was omitted from the final model to avoid multicolinearity. A two-tailed P value < 0.05 was considered statistically significant.
Results
Demographic, clinical and biochemical characteristics of participants.
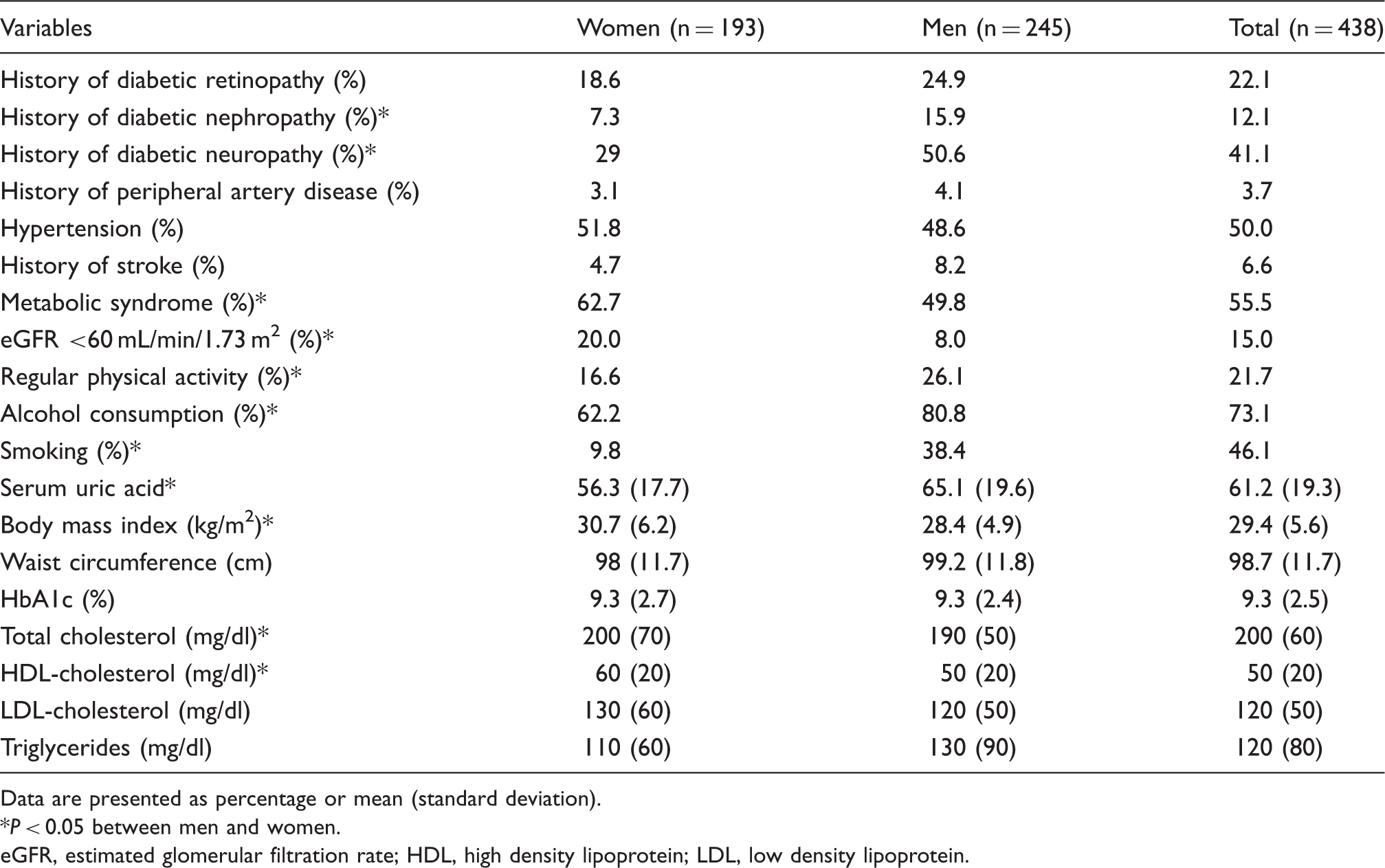
Data are presented as percentage or mean (standard deviation).
P < 0.05 between men and women.
GFR, estimated glomerular filtration rate; HDL, high density lipoprotein; LDL, low density lipoprotein.
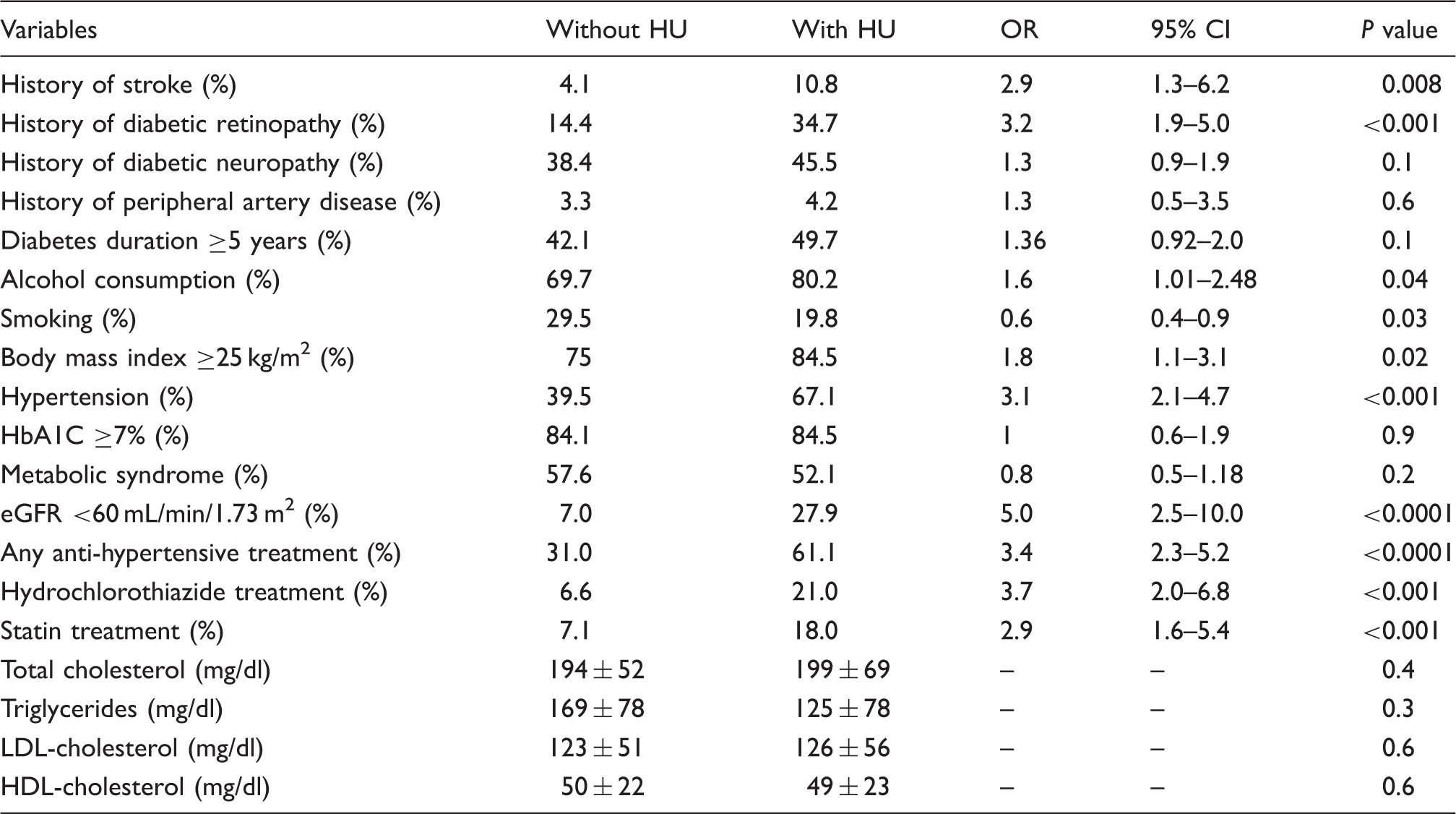
Comparison between patients with and those without hyperuricaemia.
Factors independently associated with hyperuricaemia in multivariate analysis.
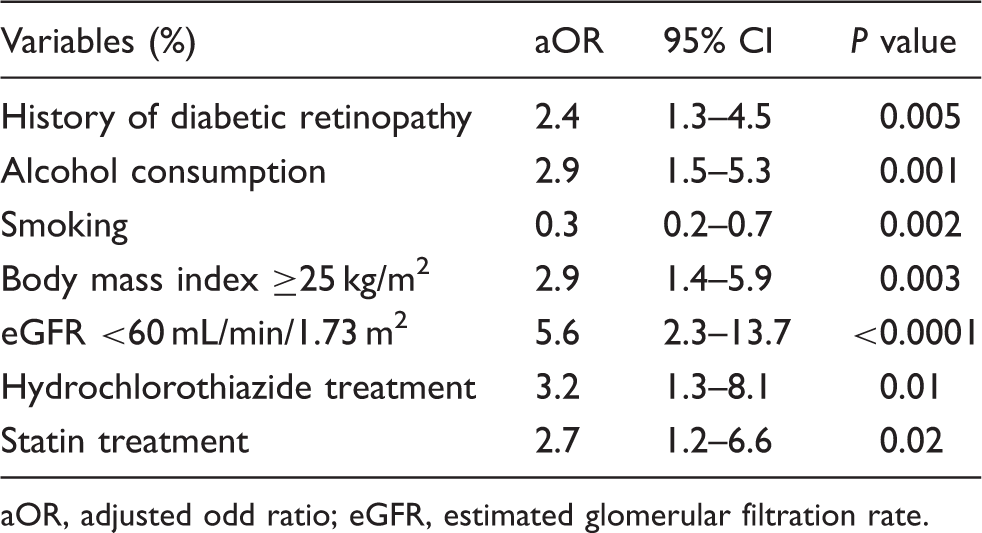
OR, adjusted odd ratio; eGFR, estimated glomerular filtration rate.
Discussion
In our study, we found that 38.1% of patients with type 2 diabetes had hyperuricaemia. We also identified overweight/obesity, alcohol intake, diabetic retinopathy, eGFR < 60 mL/min/1.73 m2, hydrochlorothiazide and statin treatment as factors independently associated with hyperuricaemia in our population.
Previous studies have reported prevalence between 16.1% in type 2 diabetic Italians 13 and 32.6% in Chinese patients with type 2 diabetes and central obesity. 4 In an ethnically similar population to ours in Nigeria, the prevalence obtained – using a similar cutoff to define hyperuricaemia – was 25%. 6 Contrary to these authors, we did not exclude patients taking diuretics, and we further showed that diuretic therapy, especially hydrochlorothiazide, was strongly associated with hyperuricaemia. This may explain the higher prevalence in our study. Potential mechanisms that link hyperuricaemia to diabetes include: inhibition of glucose-stimulated insulin secretion as observed in the animal model, 14 and inhibition of renal uric acid excretion by hyperinsulinaemia – a consequence of insulin resistance; alteration of endothelial function which in turn decreases nitric oxide bioavailability, and triggers hyperinsulinaemia, thus creating a vicious circle (reviewed in Li et al. 2 ).
Alcohol consumption and diuretic therapy are known elsewhere as risk factors of hyperuricaemia. 15 Thiazide diuretics decrease renal reabsorption of uric acid (reviewed in Chalès and Guggenbuhl 16 ). The strong association between hyperuricaemia and overweight/obesity we observed reinforces the role of hyperuricaemia as a component of the metabolic syndrome in our population.
Having hypertension was associated with hyperuricaemia in bivariate analysis, but not in multivariate analysis. This suggests that although hypertension and hyperuricaemia may commonly co-occur as components of the metabolic syndrome, the use of antihypertensive drugs such as thiazide diuretics probably play a more important role in causing hyperuricaemia.
Our finding of low eGFR as a factor independently associated with hyperuricaemia is in line with reports of many authors.5,17–19 Decreased eGFR is associated with a decrease in uric acid excretion. On the other hand, chronic inflammation, vascular endothelial dysfunction, decreased vascular bioavailability of nitric oxide and activation of renin angiotensin system induced by hyperuricaemia could damage the kidney.20–24 The association between hyperuricaemia and diabetic retinopathy has also been shown by other investigators in China.25,26 In the animal model, hyperuricaemia promotes endothelial thickening and progression of renal disease, 21 both mechanisms that could be involved in microvascular complications.
In longitudinal studies, atorvastatin reduced serum uric acid levels by increasing its urinary fractional excretion, whereas simvastatin did not. 27 In our study, statin use was independently associated with hyperuricaemia. Atorvastatin is the statin prescribed to almost all our patients. We speculate that this association may instead be related to dyslipidaemia rather than secondary to statins per se.
Similar to other reports in China 28 and in Nigeria, 6 we did not find any association between hyperuricaemia and HbA1c nor the duration of diabetes, despite the strong association with diabetic retinopathy. Whether hyperuricaemia contributes to the occurrence of these microvascular complications or is instead a consequence cannot be concluded from our study. However, the endothelial toxicity of urate monosodium 10 suggests that it is a contributing factor to endothelial injury and thus microvascular complications in type 2 diabetic patients.
Data on the association between hyperuricaemia and smoking in people with cardiovascular disease29–31 or diabetes4,6,13,32 remain controversial. In our report, smokers were less likely to have hyperuricaemia. Similar findings were reported in China. 4 Given that smoking is recognised as a major risk factor for cardiovascular disease and cancer, this certainly outweighs any risk associated with hyperuricaemia. Thus any potential protective role of smoking against hyperuricaemia would have neither clinical nor epidemiological benefit.
Our study adds new data on the clustering of cardiovascular risk factors in type 2 diabetes in Africans. However, we should acknowledge the following limitations: ours was a single-centre hospital-based and cross-sectional study, hence causality cannot be ascertained. Patients were included by consecutive sampling, which can cause selection bias. Inter-observer variations in eye examination by different ophthalmologists could be a source of error. Also we could not assess microalbuminuria, hence chronic kidney disease was defined based solely on the eGFR.
In conclusion, almost two out of five type 2 diabetic Cameroonian patients have hyperuricaemia which, as an additional cardiovascular risk factor, may contribute in increasing morbidity. Factors we found to be independently associated – overweight and obesity, some diabetes complications and thiazide diuretics – are preventable. Our results suggest that further studies should evaluate the potential cost–benefit of screening for hyperuricaemia in type 2 diabetes.
Footnotes
Acknowledgements
The authors are grateful to Yannick Mboue-Djieka for his assistance in participants’ inclusion and data management. The 2HD Research Group receives technical support from the NIHR-Bristol Biomedical Research Unit (BRU) in Nutrition, University of Bristol, UK.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The 2HD Research Group is supported by a Cruddas Link Fellowship to SPC, from the Harris Manchester College, University of Oxford, UK.