
Abstract
There is a paucity of data on the spectrum of benign gastric outlet obstruction in India. Our aim was to evaluate its spectrum and to identify the subgroup which would be most amenable to endoscopic therapy. We studied 64 patients whose aetiology revealed in approximately equal proportions: corrosive injury; gastroduodenal tuberculosis (TB); and peptic ulcer disease. The median number of endoscopic dilations required was two for TB, four for peptic ulcer disease and five for corrosive injury. Gastroduodenal TB and corrosive injury appear now to be more, or at least as, common as peptic ulcer disease as causes of benign gastric outlet obstruction in India. Gastroduodenal TB responds best to endoscopic therapy.
Keywords
Introduction
Gastric outlet obstruction (GOO) is defined as a mechanical impediment to gastric emptying, secondary to complete or partial obstruction of the distal stomach, pylorus or proximal duodenum.
The aetiology of GOO is divided into two broad groups: benign or malignant. Although malignant aetiology is the commonest cause of GOO, 15–25% have a benign cause,1,2 the commonest of which were known previously to be peptic ulcer disease (PUD), corrosive injury and chronic pancreatitis. Non-steroidal anti-inflammatory drug (NSAID)-related diaphragm disease, tuberculosis (TB), Crohn’s disease and annular pancreas are much less frequent causes.3–5 Peptic ulcer disease has traditionally been the commonest aetiology but recently we have noticed a significant decrease in its incidence owing to the widespread availability and use of proton pump inhibitors (PPI).3–6 Gastric outlet obstruction is now the least common complication of PUD and is seen in only about 2% of cases.7–9 Corrosive injury due to accidental or suicidal ingestion of acid or alkali is now a common cause of GOO in India.10,11 Tuberculosis, however, is considered as an uncommon cause and accounted for <10% of cases.12,13 The involvement of the stomach and duodenum is uncommon in TB as gastric acid creates an unfavourable environment for the survival of Mycobacterium tuberculosis. In a recently published study, the use of PPI for >3 months was associated with an increased risk of TB. 14
There is little data regarding any change over the last decade in the spectrum of benign GOO. We therefore conducted this study with the aim of evaluating its spectrum and to identify the subgroup which would be most amenable to endoscopic therapy.
Methods
Our prospective study was conducted at Govind Ballabh Pant Hospital, New Delhi, India, between November 2013 to January 2015. Consecutive patients of all age groups were included. The diagnosis of benign GOO was made on the basis of endoscopic and/or radiological evidence. Patients with gastroparesis without any mechanical obstruction, drug-induced delayed gastric emptying and malignant GOO were excluded from the study.
Each patient underwent a detailed clinical evaluation followed by laboratory investigations including full blood count, liver and kidney function tests, serum electrolytes, acid base analysis, HIV ELISA and Mantoux test (in suspected TB patients). Investigations included chest radiography, upper gastrointestinal (GI) barium series and abdominal CT scan. An upper GI endoscopy was done after proper nasogastric lavage using a forward viewing endoscope (Olympus GIF-1TQ 160, Tokyo, Japan). Multiple biopsies (8–10 biopsies) and/or endoscopic mucosal resection (EMR) for nodular lesion was done by the technique previously described by us. 13
Peptic ulcer related GOO was defined in patients, with established PUD, presenting with features of GOO with typical radiological/endoscopic features suggestive of PUD in the absence of any mass lesion on endoscopy or abdominal CT.
The diagnosis of gastroduodenal TB was made on the basis of pathological lesions in the antrum, pylorus or duodenum showing the presence of acid fast bacilli (AFB) on Ziehl Neilson staining or polymerase chain reaction (PCR) positivity for Mycobacterium TB on endoscopic biopsies. Where AFB could not be documented, the presence of epitheloid granulomas, coupled with unequivocal clinical response to anti-tubercular therapy (ATT) within 6–8 weeks of starting such, were taken as diagnostic criteria for gastroduodenal TB.
The diagnosis of corrosive GOO was based on a history of corrosive ingestion with evidence of injury on endoscopy.
Duodenal web-related GOO was diagnosed based on endoscopic and/or radiographic evidence of a web in the absence of any mass lesion on abdominal CT.
All patients were admitted and underwent fluid and electrolyte correction as required. Patients with GOO were treated for the underlying aetiology where indicated and subjected to endoscopic balloon dilation to alleviate the obstruction. Balloon dilation was done under fluoroscopic guidance using a side viewing endoscope (Olympus GF-TJV180, Tokyo, Japan) and through the scope (TTS) balloon (Wilson Cook, NC, USA). Serial dilation was done starting with a balloon size of 12 mm every 2 weeks; the dilation endpoint was defined as successful at 18 mm for adults and 16 mm for children, respectively. All patients were monitored over the next 24 h for any procedure-related complications. Oral feeding was started 24 h post dilation. After achieving dilation endpoints, it was repeated only if the patient had recurrent obstructive symptoms. The number of dilations required for complete relief of GOO symptoms was recorded for each patient. Endoscopic dilation in corrosive GOO was started after healing of ulcers as confirmed by upper GI endoscopy.
Patients with gastroduodenal TB were started on a four drug regime (rifampicin, isoniazid, pyrazinamide and streptomycin) according to dose as per body weight for an initial 2 months, followed by rifampicin and isoniazid in the continuation phase. Injectable streptomycin was used in place of ethambutol as its absorption is unaffected by recurrent vomiting. Compliance to ATT and its related side effects were monitored regularly on follow-up visits. Patients with PUD-related GOO were treated with Helicobacter pylori eradication therapy along with PPI as per standard guidelines. Patients with pancreatitis-related GOO received standard therapy for pancreatitis and its complications along with endoscopic balloon dilation. Patients with non-congenital duodenal web underwent web incision by the technique described earlier. 15 They were advised to avoid NSAIDs. Duodenal polypectomy was done for the patients with an obstructing duodenal polyp. Patients refractory to endoscopic dilation were referred for surgical management.
Our study was approved by the institutional ethics committee and informed consent was taken from each study subject.
Statistical analysis
Statistical analysis was performed using statistical package for social sciences (SPSS) version 22.0 for Windows (SPSS, Chicago, IL, USA). Data were expressed as absolute numbers and percentage for categorical variables and mean ± standard deviation (SD) or median and ranges for continuous variables, as appropriate. Wilcoxon’s signed rank test and Mann–Whitney U test were used to analyse paired and unpaired data, respectively. A P value of <0.05 was considered to be significant.
Results
Baseline demographic, clinical and laboratory data of patients (n = 64).
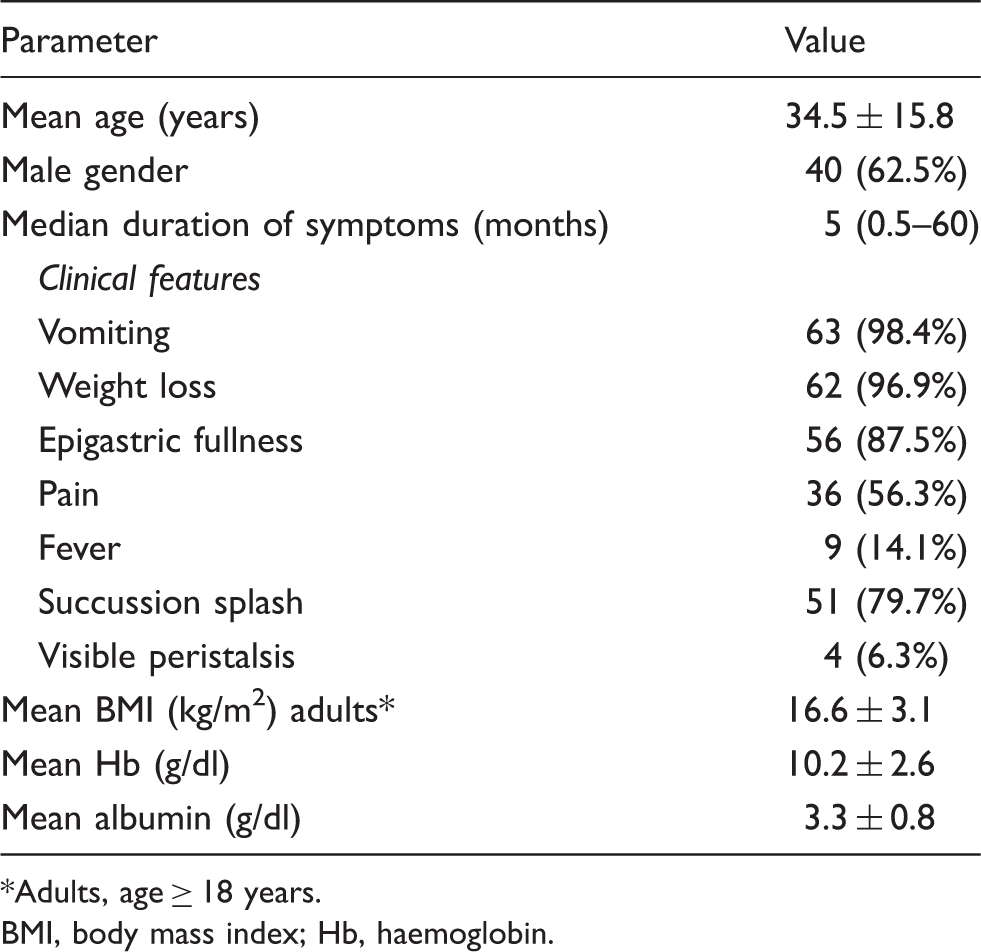
Adults, age ≥ 18 years.
BMI, body mass index; Hb, haemoglobin.
The three commonest causes of benign GOO were: corrosive injury, 16 (25%); gastroduodenal TB, 16 (25%); and peptic ulcer disease, 15 (23.4%). Other causes were: duodenal web, 5 (7.8%); chronic pancreatitis, 5 (7.8%); duodenal polyp, 1 (1.6%); strongyloidosis, 1 (1.6%); and idiopathic, 5 (7.8%), where no cause could be identified despite a detailed workup (Figure 1).
Spectrum of benign gastric outlet obstruction. GOO, gastric outlet obstruction.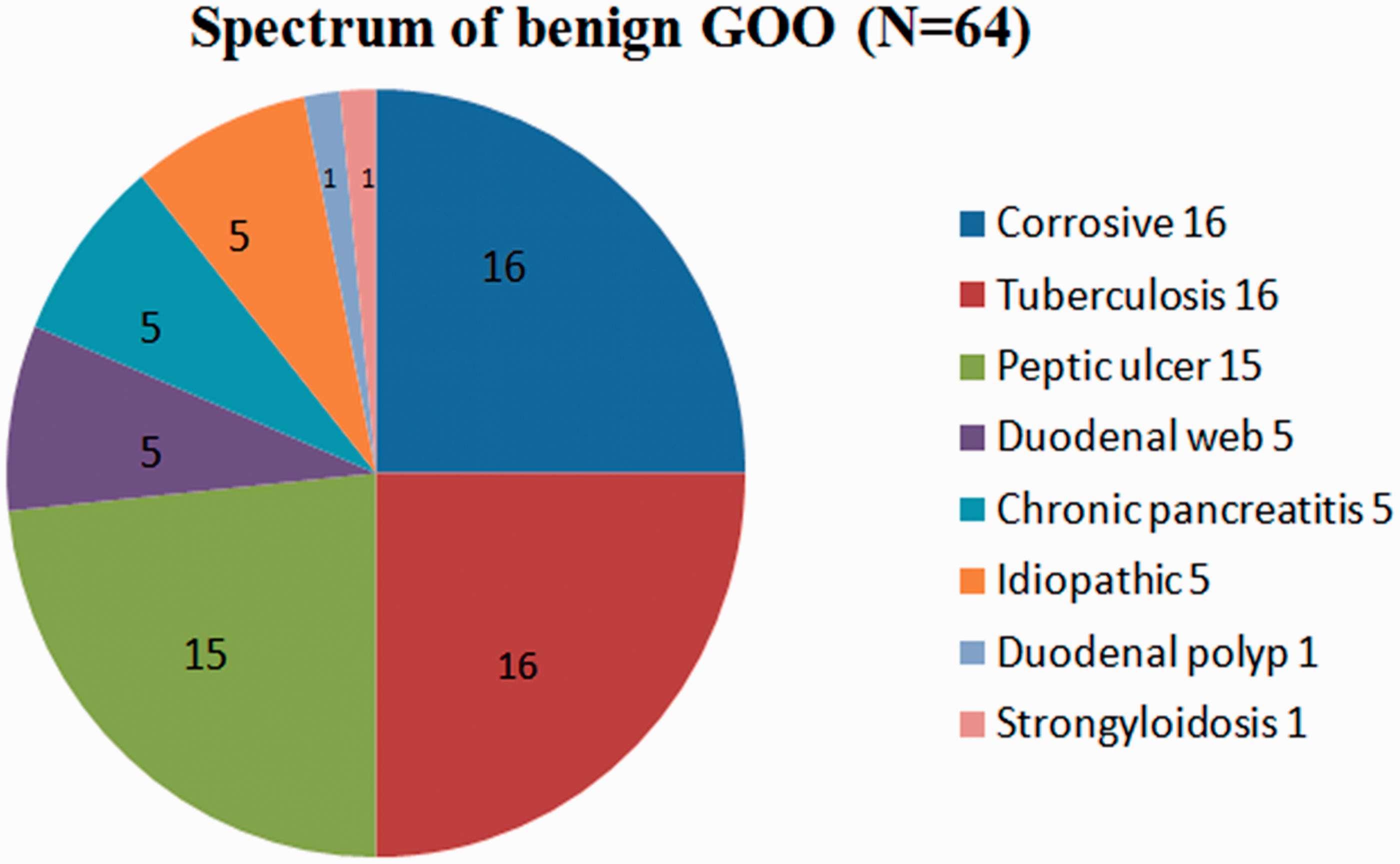
All patients with corrosive GOO had pyloric stenosis. Five (31.3%) of 16 patients also had a concomitant oesophageal stricture. Concomitant pyloric involvement was documented in five (31.3%) of the 16 patients with GOO due to gastroduodenal TB. Four (25%) patients with tubercular GOO had a prior history of treatment for pulmonary TB, whereas concomitant extra-abdominal TB (mediastinal lymphadenopathy) was documented in one patient only. Granulomatous inflammation was documented on histology in 15 (93.8%) patients of tubercular GOO, while one patient had positive PCR for Mycobacterium tuberculosis. None of tissue biopsy/EMR specimens were positive for AFB. Among the 16 patients with tubercular GOO, 10 (62.5%) had tissue diagnosis on pinch tissue biopsy while EMR was required to establish the tissue diagnosis in four (25%) patients. In the remaining two (12.5%) patients, the tissue diagnosis was established by fine needle aspiration from either mediastinal or mesenteric lymph nodes. None of the tubercular GOO patients had co-existing HIV infection. Of the 15 patients with PUD related GOO, the pylorus was involved in eight (53.3%) while duodenal involvement was observed in all patients. Of the five patients with duodenal web, two had a congenital web, whereas three had a NSAID-induced web. Of the five patients with pancreatitis related GOO, all had chronic pancreatitis, diagnosed on abdominal imaging. One patient had a large duodenal polyp (3.5 cm) and one had gastric strongyloidosis which was documented on antral biopsy. In five patients the cause of GOO could not be established although malignancy was excluded on the basis of histopathology and abdominal imaging (Figure 2).
Endoscopic and barium radiographic images of patients with benign gastric outlet obstruction (a–d).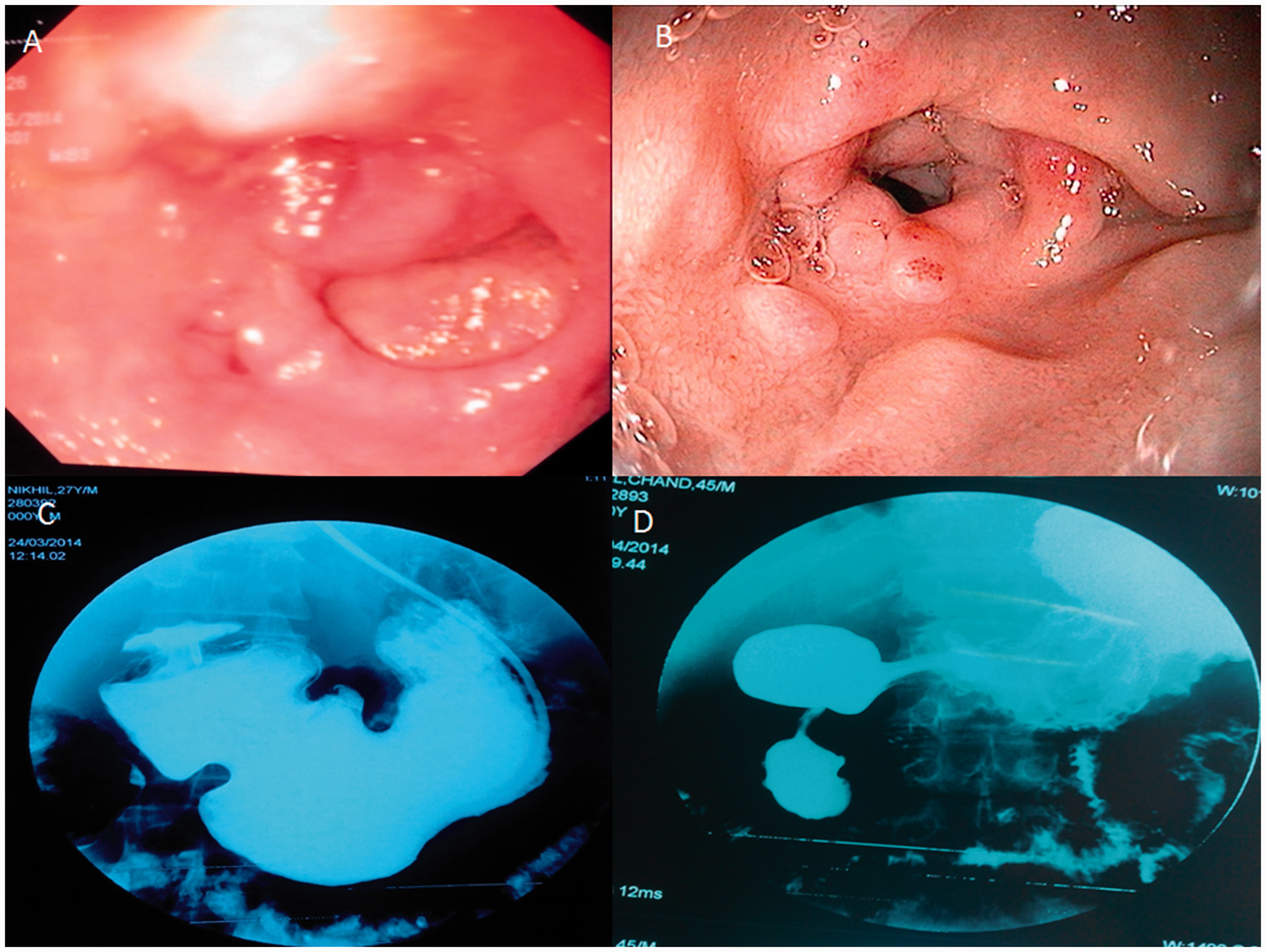
Endoscopic and surgical intervention.

Discussion
In our study, corrosive injury, gastroduodenal TB and PUD were equally common causes of benign GOO while other causes were rare. The mean age of the cohort was 34.5 years which highlights the fact that most patients with GOO are young adults. Recurrent vomiting with weight loss were the two cardinal symptoms present in majority. Prolonged fever of longer than 2 weeks was recorded only in patients with TB-related GOO.
Gastric outlet obstruction has traditionally been considered synonymous with pyloric stenosis as a result of PUD in adults, accounting for up to 90% cases in the past. 16 The proportion of PUD cases has been falling with TB accounting for <10 % in studies over the past 20 years.3–6
Our study showed a paradigm shift in aetiology of benign GOO with TB emerging as a common cause along with corrosive induced gastric injury. Tuberculosis is still a major public health problem in low and middle-income countries such as India. One hypothesis to explain this change is related to the widespread use of PPI, leading to a general decrease in the incidence of PUD.5,17 Additionally the use of PPI weakens the natural barrier against mycobacteria by its profound suppression of acid secretion. A recently published study showed that use of PPI for >3 months is associated with an increased risk of tubercular infection and reactivation of TB. 14 Corrosive ingestion is a third cause.18,19
Our study showed that tubercular GOO required a lower number of endoscopic dilation sessions and surgical treatment compared to corrosive and PUD-related GOO. These results are in agreement with our previous published study in which all 10 patients with gastroduodenal TB were effectively treated with a combination of endoscopic balloon dilation and ATT. 13 Patients with corrosive GOO are known to require more sessions of dilation vis-à-vis PUD-related GOO. 20 Only two of our patients developed endoscopic dilation related complications: haemorrhage was managed conservatively in one and duodenal perforation required surgery in the other. Our study manifestly showed that endoscopic dilation for benign gastric outlet obstruction, especially for tubercular GOO, is effective along with the definitive treatment with ATT.
In conclusion, our data suggest that in addition to peptic ulcer and corrosive injury, gastroduodenal TB is an important but under-reported cause of GOO. Among these three groups, endoscopic therapy has the best outcome in the subset of patients with gastroduodenal TB.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.