
Abstract
Vaccine vial monitor (VVM) is now commonly used for vaccines that are included in the National Immunization Schedule in India. It helps to indicate the viability of the vaccine and of the proper functioning of the cold chain. This is useful as it prevents health personnel from administering damaged vaccine. Studies have shown a lack of awareness of health workers regarding the use and interpretation of a VVM. The current study, undertaken among the caregivers of children who were immunized, showed that this lack of information about the VVM also exists among the caregivers. This deficiency in knowledge, both in the health workers and the caregivers, can affect the health of the child and needs urgent attention.
Introduction
India has been certified polio-free by the World Health Organization (WHO) after going three years without an endemic case of polio. The eradication of polio in India is heralded as one of the biggest achievements in global health efforts. Much of this success can be attributed to the massive effort involving a surveillance network and a highly structured immunisation plan in place. 1 The WHO has acknowledged the role of immunisation as the prime factor for the observed success. 1 In general, to ensure that the vaccine does not lose its potency during transport and storage, vaccine vial monitors (VVMs) are used. 2 A VVM is a thermochromic label put on vials containing vaccines which gives a visual indication of whether the vaccine has been kept at a temperature which preserves its potency. The labels are designed in response to the problem of delivering vaccines to developing countries where the cold chain is difficult to preserve.2,3 The VVM changes colour as it is exposed to heat, letting health workers know at a glance whether the vaccine has been damaged or can still be used for immunisation. Currently, a VVM is being used in other vaccines as well as oral polio vaccine (OPV). These vaccines include hepatitis B, BCG, DPT, DT etc. 4
Research has shown that despite several rounds of training of health workers, the level of awareness and practices regarding the significance of a VVM in maintaining potency of vaccines has been low.5,6 The level of awareness regarding a VVM will have huge bearing on the success of the ongoing immunisation activities. Awareness of the significance of a VVM among beneficiaries may also help, by compelling health workers to check for a VVM status during each immunisation session. Till now, the studies have focused on assessing the knowledge of the health workers regarding the VVM and we found no study that looks at the awareness among caregivers of the children receiving immunisation.5,6
With this background, the current study was done primarily to document the awareness of the caregivers, accompanying the children to immunisation clinics, about the VVM. As a secondary objective, a brief assessment of the caregiver’s knowledge about polio was also undertaken.
Materials and methods
This cross-sectional study was conducted in an urban resettlement colony of Gokulpuri in the north-east district of Delhi. It is the field practice area of the Department of Community Medicine, Maulana Azad Medical College, New Delhi, India. It represents the situation of urban resettlement slums in Delhi and has been in existence for more than 20 years. According to the economic survey of Delhi, 2002 slums have been categorised typologically into eight types. Resettlement colonies were formed in Delhi under a scheme wherein the residents of slums were relocated in permanent colonies. Gokulpuri is divided into four blocks with a total population of around 21,000. Healthcare services are largely provided by an Urban Health Centre (UHC) Gokulpuri which is associated with the Department of Community Medicine at Maulana Azad Medical College, New Delhi. As per the yearly survey conducted by the UHC along with the Department of Community Medicine, Gokulpuri mostly comprises the urban population belonging to the lower to lower-middle socioeconomic class.
The sample size was calculated based on the findings of the study by Chudasama et al. where all members present at the immunization booth, working on National Immunization Day were interviewed by using predesigned and pretested questionnaires to assess their awareness regarding type of OPV and VVM in urban areas of Valsad district. 5 There were four categories of study participants: (1) Auxiliary Nurse Midwife (ANM)/Female Health Worker (FHW)/Lady Health Visitor (LHV)/Pharmacists; (2) nursing students, (3) Nagarpalika staff (i.e. members of the municipal corporation); and (4) volunteers. The findings related to the ‘volunteers’ were considered for calculating the sample size for the current study as no prior study could be found which carried out such a study in normal population or among the caregivers of the children. ‘Volunteers’ were considered closest to the normal population. In the study by Chudasama et al., only 13% of the volunteers had heard about the VVM. 5 This finding was used to calculate the sample size for the current study along with an absolute precision of 5% and alpha error of 0.05. Accounting for a non-response rate of 10%, the final sample size was 200.
A pre-designed, pre-tested, semi-structured, interview schedule containing demographic data, awareness regarding polio and polio vaccination, and the vaccine vial monitoring, was used to collect data. Data were collected from March till May 2013. A total of 200 people were included and interviewed. The caregiver accompanying every third child who was being vaccinated was included for the study after obtaining a written consent. This selection process continued till the sample size was achieved. The study was conducted during routine immunization days (Wednesdays and Fridays) at the UHC. The questions were asked in the local language (Hindi) to elicit the desired information. Statistical analysis was done using SPSS version 16 and Microsoft excel. Chi-square test was applied and P value < 0.05 was considered statistically significant.
Results
Sociodemographic characteristics of the study respondents (n = 200).
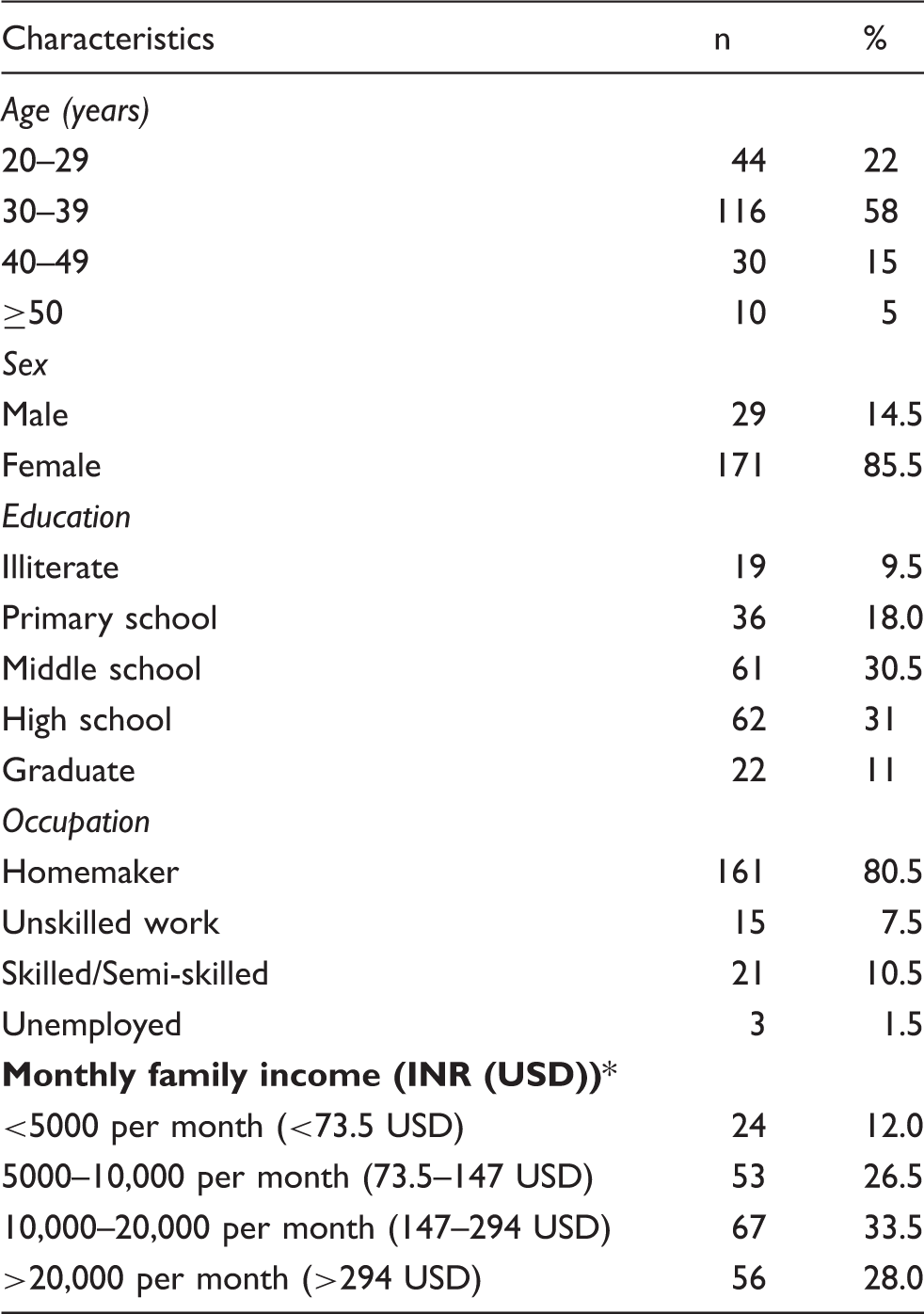
Considering 1 USD equal to 68 INR.
Awareness about poliomyelitis and its prevention, among the study participants (n = 183).
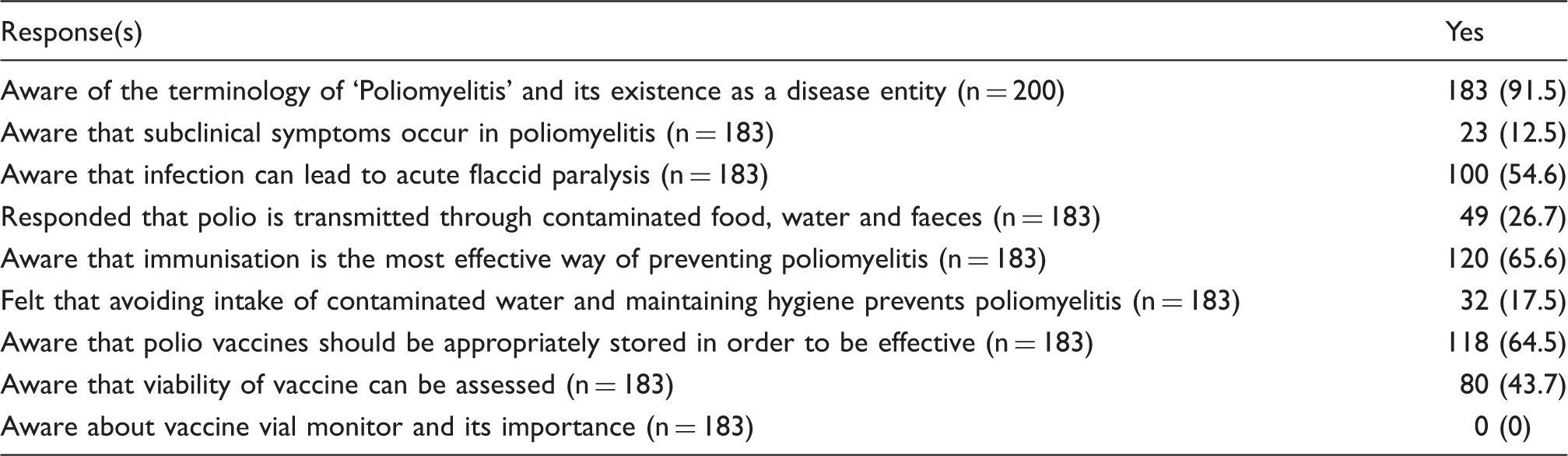
Out of the respondents who were aware of polio, more than half (100/183; 54.6%) knew that infection with polio can lead to acute flaccid paralysis and disability whereas only 12.5% (23/183) were aware that subclinical symptoms occur in polio. Nearly two-thirds were aware that polio vaccine should be stored appropriately in order to be effective (118/183; 64.5%) (Table 2).
Around 40% were aware that the vaccine viability could be assessed (80/183; 43.7%). Among these, 22.5% (18/80) relied on the health worker, whereas 18.7% (15/80) were in favour of checking the date of expiry. None of the respondents were aware of the importance of a VVM and the interpretation of colour change in the VVM on exposure to heat (Table 2).
Overall, the awareness regarding polio and the OPV was found to be more among the respondents who received some sort of education as compared to those who were illiterate (P <0.05). There was no significant difference between male and female respondents and across different ages.
Discussion
Pulse Polio Immunization programme was launched in India in 1995. Children in the age group 0–5 years are administered polio drops during national and sub-national immunisation rounds (in high-risk areas) every year. The Pulse Polio Initiative was started with an objective of achieving 100% coverage under OPV. It aimed to immunise children through improved social mobilisation, plan mop-up operations in areas where the polio virus has almost disappeared and maintain a high level of enthusiasm among the public. The term ‘pulse’ has been used to describe the sudden, simultaneous mass administration of OPV on a single day to all children aged 0–5 years, regardless of the previous immunisation. Vaccine vial monitoring was introduced in the intensive pulse polio immunisation programme in 1998. The idea behind its use was to help the booth staff to ensure the viability of the vaccine and identify cold chain breakdown if accidentally occurred.
In spite of repeated training of healthcare workers prior to every pulse polio immunisation day, studies show that a lack of knowledge about VVMs still exists. A study done in Valsad, Gujarat among members working on the pulse polio booth on National Immunization Day found that 51.6% of them had not heard of a VVM. 5 Awareness was very poor for the VVM regarding its function, how to read a VVM and when OPV should be discarded. 5 Similar findings have been reported by Thakur et al. in Chandigarh. 7
For the success of any public health program, community awareness has always been considered important. Ownership of their health by community members forms a solid foundation for any health initiative to achieve its goal and an immunisation programme is no exception to it. While public awareness about the importance of immunisation is extremely important, it further needs to be strengthened. It would be useful if the parents/caregivers of children receiving immunisation have the required knowledge about the VVM and are able to check the potency of the vaccine using this information. The awareness of the importance of the VVM among beneficiaries would not only increase their participation but would also make the health workers more vigilant about a VVM during vaccination sessions, thus helping to improve the quality of immunisation services.
This awareness regarding VVM can be generated through community activities like role plays, involving community leaders and through the use of local media. Posters/banners at strategic positions in the community and involving frontline health workers to educate the family members will also be helpful. Another useful approach could be to educate some mothers/caregivers within the community and motivate them to spread the information to other mothers/caregivers in the community. Community discussions at regular intervals, initiated by health personnel, would be another potential opportunity to educate the community and fill this gap in their knowledge. Audiovisual aids can be used in the immunisation clinics so that those waiting for their turn to get their child immunised can be exposed to the concept of VVM and its importance. Overall, a dedicated effort needs to be made by the health system to fill this knowledge gap in the community.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.