
Abstract
Dengue fever is of great concern to public health in India as it contributes significantly to the burden of healthcare. The aim of our study was to measure mortality in dengue and its association with hepatitis and thrombocytopenia. Our study was performed in a tertiary care setting in the state of Kerala in southern India. Adult patients admitted in the year 2013 were included. Among 1308 confirmed dengue patients, the mortality rate was 1.76%. Hepatitis and thrombocytopenia were present in over 80% of all patients, but severe hepatitis was seen in 11.4% and severe thrombocytopenia in 9.3%. These were markers of fatal outcome. Other factors significantly associated with mortality were age >60 years, male sex, diabetes and the presence of any co-morbidity.
Introduction
Dengue, a flavivirus infection transmitted by the Aedes mosquito, is the world’s most common and geographically widespread viral haemorrhagic fever, especially in the Americas, the Pacific islands and continental Asia. 1 The incidence of dengue has been on the increase for many decades and the actual number of cases is seriously under-reported. It is estimated that globally, 390 million people are infected, of whom 96 million manifest clinical illness, 2 causing significant morbidity and mortality especially in low- and middle-income countries (LMICs) and is a huge burden on their economies. 3 During the epidemic of 2013, 75,808 cases and 193 deaths were reported in India. The southernmost state of Kerala ranked second in dengue mortality. 4 In the same year, our hospital saw an unprecedented increase in the number of dengue patients compared with an earlier study. 5 Manifestations of dengue, which were previously reported as rare, have become more common; and these include encephalopathy, liver and renal failure.6,7 Case fatality rate without treatment may be as high as 20%. Though there is no specific treatment for dengue, effective medical care may reduce case fatality to <1%. 2 Estimates suggest that annually >50 million cases of severe dengue occur in Asian countries with a case fatality rate of nearly 5%. 8
Hepatitis is common in dengue; hence, measurement of transaminases is mandatory. 9 However, acute liver failure is rare. 10 Liver involvement is known to have a spectrum from asymptomatic simple hypoalbuminaemia to symptomatic hepatitis, or acute or acute-on-chronic liver failure. 11 The virus seems to have a replication phase in hepatocytes, causing hepatic injury, stimulating apoptosis, microvascular steatosis and the development of Councilman-Rocha Lima bodies, similar to the situation found in yellow fever and other viral haemorrhagic diseases.12–14 Deranged liver function is common and may also be a response to unregulated host immune response.
Although dengue fever is a self-limiting febrile illness, dengue haemorrhagic fever (DHF) is characterised by haemorrhagic manifestations associated with thrombocytopenia and increased vascular permeability. 15 Secondary infection in dengue endemic areas constitute a risk for DHF. Bone marrow suppression and immune mediated destruction are proposed mechanisms. The severity of DHF depends on an associated capillary leak, subsequent haemostasis and hypotension. 16
Our objectives were to measure the mortality among inpatients with dengue and to study the association of mortality with severe hepatitis and thrombocytopenia.
Materials and methods
Our study was performed in a tertiary care teaching hospital situated in a rural setting in the southern state of Kerala in India. Ours was a hospital record-based cross-sectional study during an epidemic, which constituted a retrospective manual search of case sheets of all dengue in patients from 1 January to 31 December 2013. Patients aged >18 years and confirmed to have dengue by an IgM dengue antibody test or NS1 antigen were identified from hospital records. Outpatients were excluded from the study. Variables noted were age, sex, co-morbidities, liver enzyme assays and platelet counts, complications of dengue infections and condition at the time of discharge. The elderly age group was defined as ≥60 years. Dengue hepatitis was graded based on degree of elevation of either aspartate transaminase (AST) or alanine transaminase (ALT), whichever was higher. Our reference value for a normal level was ≤45 U/L. Hepatitis was graded as follows: mild (elevation <3 times); moderate (elevation >3–9 times); and severe (elevation >10 times). Platelet counts of 20,000–150,000/µL were graded as mild thrombocytopenia and <20,000/µL was graded as severe. Data entry was done using Epi Info software version 7 and analysis using R software version 3.1.1. Median and interquartile ranges (IQR) were calculated for time variables. Proportions were calculated for categorical variables. Fisher’s exact test was done for association of risk factors with mortality and odds ratios (OR) were calculated with 95% confidence intervals (CI).
Ethical consideration
The study was approved by Institutional Ethics Committee (IEC) of the hospital.
Results
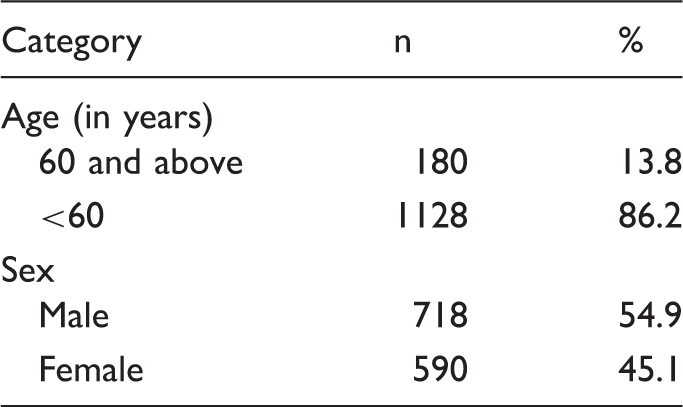
Age and sex distribution of study participants (n = 1308).
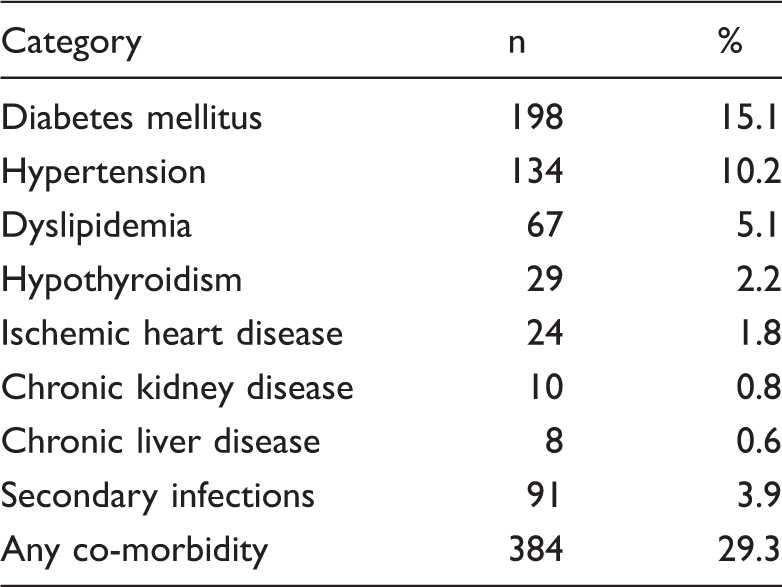
Co-morbidities of study participants (n = 1308).
Acute co-infections were noted in 27 (2.06%) patients and this list includes hepatitis A (0.91%), leptospirosis (0.46%), typhoid (0.23%), paratyphoid (0.23%), malaria (0.07%), scrub-typhus (0.07%) and chickenpox (0.07%). There were also associated urinary tract infection in 43 (3.29%), but the majority had insignificant bacteriurea with no significant growth in culture and most were treated with quinolones. Dengue does not usually cause upper respiratory infection, but among these six patients (0.46%) had sinusitis and tonsillitis as the predominant presentations. Lobar pneumonia, seen in five patients (0.38%), showed features of lobar involvement and needed treated with i.v. antibiotics. Sputum grew streptococcus pneumoniae in two patients. All patients were elderly and MRSA and E. Coli sepsis were seen in two patients (0.15%). Diarrhoea was seen in 31 patients (2.37%), but stool culture was negative in all, and so may have been due to an associated colitis. Association with pancreatitis was found in ten patients (0.76%), where lipase levels were elevated to ≤1500 IU/L, all having been shown echographically to have a normal pancreas, and symptomatic acalculous cholecystitis in eight patients (0.61%): all were managed conservatively. Two further patients presented with hypoxia and bilateral fluffy radiological lung infiltrates suggestive of acute respiratory distress syndrome. These patients were also managed conservatively with intravenous fluids and antibiotics. There were also two patients (0.15%) with severe headache and neck stiffness whose lumbar puncture suggested aseptic meningitis. These conditions indirectly prolonged hospital stay and morbidity. The median duration of hospital stay was four days (IQR, 3–6 days).
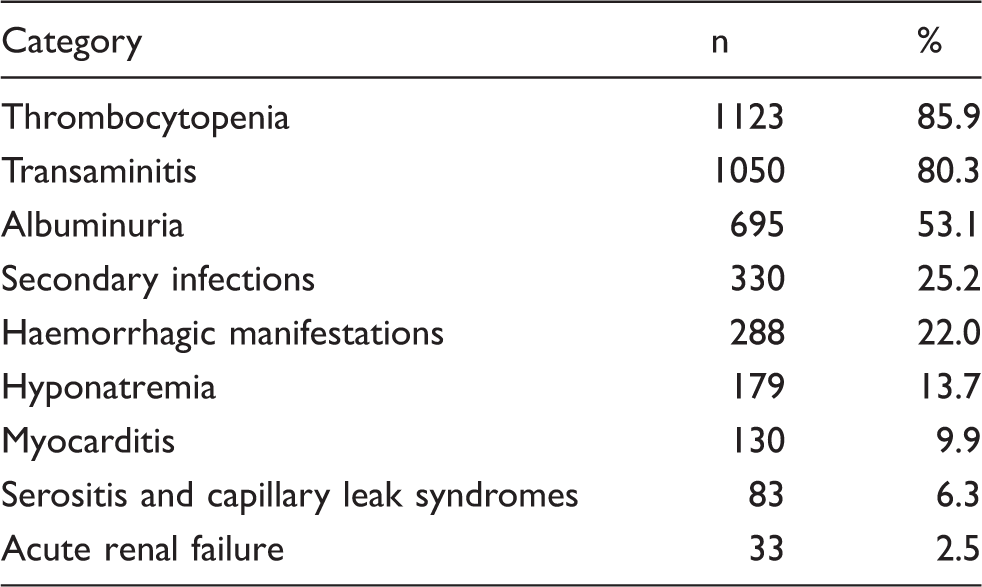
Severe complications encountered were thrombocytopenia or hepatitis in >80%. Thrombocytopenia was mild in 76.6% and severe in 9.3% patients, resulting in melena and haematuria in 25%. Hepatitis was mild (grade B) in 33.9%, moderate (grade C) in 35.0% and severe (grade D) in 11.4% patients. ALT was elevated in 1023 (78.2%) and AST in 1041 (79.5%). The former level was higher than the latter in 963 (73.6%). The remaining parameters were tested only in some patients at the discretion of the treating doctor and may not be representative of the entire cohort.
Complications of dengue among study participants (n = 1308).
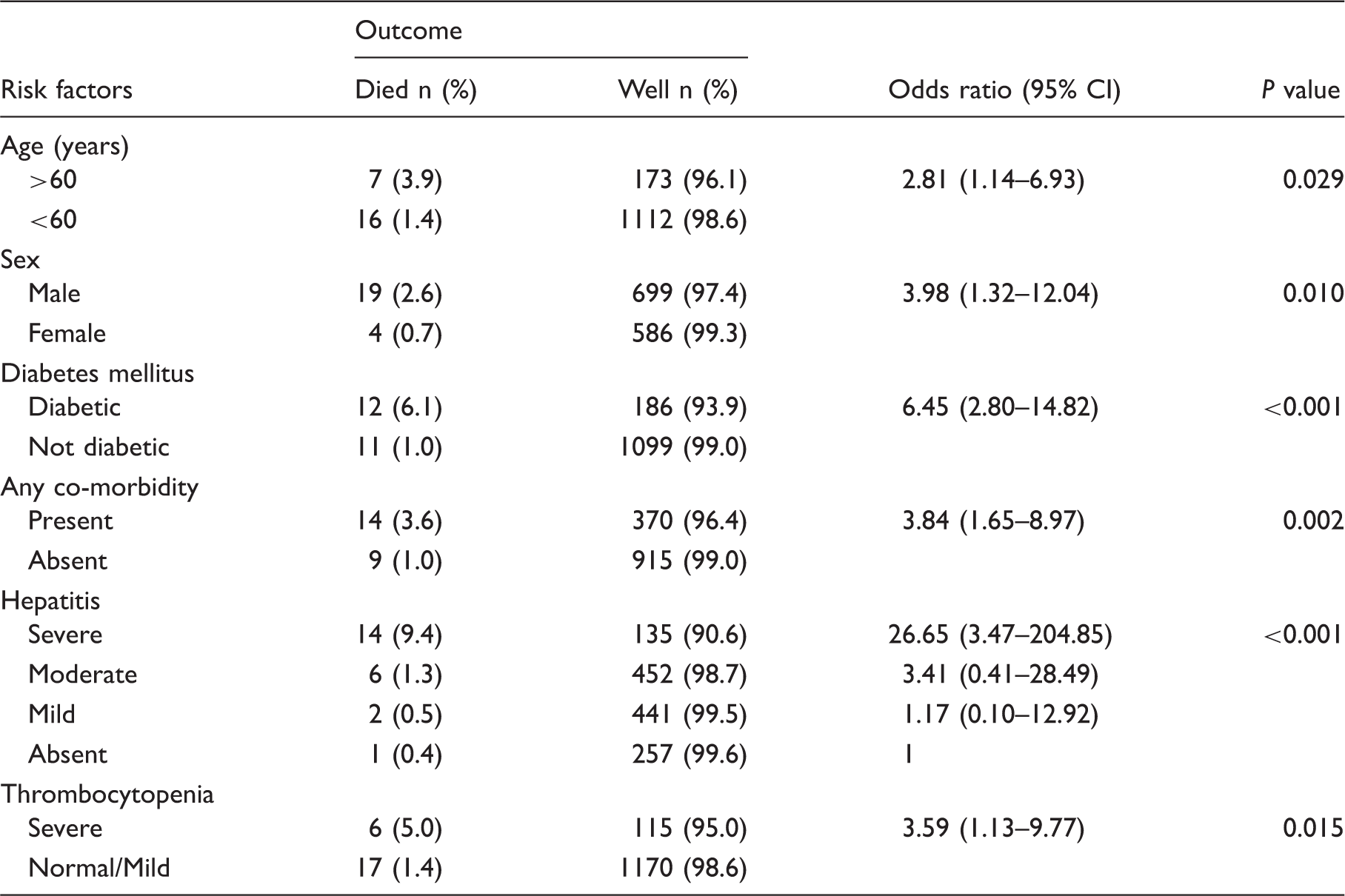
Risk factors for dengue mortality.
Discussion
In studies reported from other parts of India, mortality rates were somewhat higher (3.5% and 6%).17,18 As in our study, Lee et al. also reported higher mortality for the elderly, who are expected to have greater co-morbidities.19,20 Likewise diabetes, hypertension and other co-infections have been found to lead to higher mortality.13,21 Male sex may, however, be less reliable as a factor.20,22,23 The important message of our study is that mortality is related to severe liver impairment 24 and thrombocytopenia. 25 Transaminase levels begin to rise in the first three days of illness and peak during the second week of illness. Elevated transaminase levels have been suggested as potential markers to help differentiate dengue from other viral infections during the early febrile phase. 26 In dengue, AST rises sooner than ALT and reaches a higher peak, which is unusual in viral hepatitis; 27 this was also observed in children with dengue. 28 ALT is primarily associated with hepatocytes but minimally with cardiac and skeletal muscle, but AST is found in hepatocytes, erythrocytes, cardiac and skeletal muscle, kidney and brain tissue.9,29 The latter levels fall faster than ALT; this may be explained by the shorter half-life of AST 9 or by a quicker recovery of hepatic than musculoskeletal disease. 30 Severe liver involvement (acute liver failure and/or jaundice) may occur during the second week of illness, but is rare. 31 Jaundice may occur occasionally in dengue. 9 We found in common with Pakistani colleagues that a rise in transaminases tenfold or higher was associated with higher mortality. 32
Thrombocytopenia has always been one of the criteria used by World Health Organization (WHO) guidelines as a potential indicator of clinical severity. 3 In the most recent 2009 WHO guidelines, the definitions generally describe a rapid decline in platelet count or a platelet count <150,000/µL. 6 The virus directly or indirectly affects bone marrow progenitor cells by inhibiting their function 33 to reduce the proliferative capacity of haematopoietic cells, 34 and invades platelets and uses a translational machinery for virus replication. 35 Besides platelets counts, the functional disruption of these cells is associated with a significant deregulation of the plasma kinin system and the immunopathogenesis of dengue. 36 Dengue infection may also induce platelet consumption due to disseminated intravascular coagulation (DIC), platelet destruction due to increased apoptosis, lysis by the complement system and by the involvement of antiplatelet antibodies.37–39
Other studies report an association of mortality with various clinical, haematological and biochemical parameters such as absolute atypical lymphocytes, haematocrit, prothrombin time, activated partial thromboplastin time, serum lactate levels, plasma leakage signs and acute kidney injury.40–43 Only some of these were found to be relevant in our study and they may not be readily available in LMIC settings. Severe liver impairment and severe thrombocytopenia are, however, definite markers of fatal outcome in dengue fever. Therefore, close monitoring of these is essential, and rigorous treatment of co-existing illnesses or infection is mandatory.
Footnotes
Acknowledgements
The authors thank Dr. Blessy Sara Eldos (intern), Dr. Ashly Alexander (intern), Dr. Lakshmi Parvathy Sasi (intern), Dr. Mary Neteeya (intern) and Dr. Sreekanth Shenoy (intern) for their support in data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.