
Abstract
The gold standard for detecting bacterial sepsis is blood culture. However, the sensitivity of blood culture is low and the results take 48–72 h. Molecular assays for the detection of bacterial DNA permit early detection of a bacterial cause as the turnaround time is 6–8 h. We undertook an evaluation of the performance of universal bacterial primer (16S rRNA) polymerase chain reaction (PCR) in the diagnosis of neonatal sepsis at a tertiary care medical college teaching hospital. 16S rRNA PCR was positive in all cases of blood culture proven sepsis. PCR revealed 95.6% sensitivity, 100% specificity, 100% positive predictive value and 91.2% negative predictive value and so appears to be a useful tool for the early diagnosis of bacterial neonatal sepsis.
Introduction
An ideal diagnostic test for neonatal sepsis should be rapid with 100% sensitivity and specificity. A negative test should reliably exclude sepsis so that no neonate with sepsis is left untreated. 1 Prior antibiotic therapy frequently interferes with growth on blood culture. 2 Polymerase chain reaction (PCR) amplification of highly conserved DNA sequences found in all bacteria would permit fast and sensitive determination of the presence of bacteria in clinical specimens. 3 Recent reports on use of 16S rRNA PCR for the diagnosis of neonatal sepsis have shown promising results.
Materials and methods
The present study was conducted in the Neonatal Services Division, Department of Paediatrics in collaboration with the Department of Biotechnology & Molecular Medicine, Pt. B.D. Sharma PGIMS, Rohtak from May 2013 to October 2014. One hundred consecutive symptomatic neonates with birth weight >1500 g, clinically suspected to have sepsis and meriting empirical antibiotic therapy, were enrolled provided they had not received antibiotics in the preceding 72 h, including antepartum antibiotics to the mother in the previous three days. Neonates with major congenital malformations and severe birth asphyxia (APGAR score <3 at 5 min or cord pH < 7) were excluded from study owing to decreased life expectancy. Before starting antibiotic therapy, blood was collected for PCR, blood culture and sepsis screen in all the patients. In total, 200 µL of blood was collected aseptically in EDTA treated vacutainers (BD) and was further analysed immediately or stored at 4℃ until analysed. DNA was extracted using the Phenol Chloroform method as described by Sambrook et al. 4 16S rRNA gene was amplified from this sample as described by Chakravorty et al. 5 on BioRad, DNA engine endpoint PCR thermal cycler. A 203 bp amplicon was obtained as expected. PCR primers used in this study included a forward primer V3F 5′-CCAGACTCCTACGGGAGGCAG-3′ and a reverse primer V3R 5′-CGTATTACCGCGGCTGCTG-3′. PCR reaction mixture consisted of 0.2 mM dNTP, 1.5 mM MgCl2, 20 pM forward and reverse primers each and 100 ng of DNA template in a reaction volume of 50 µL. All the reagents used for DNA extraction and PCR were of Molecular Biology grade, whereas PCR reagents were from MBI Fermentas, the reagents and chemicals used for DNA extraction were of highest purity from Sigma chemical company. PCR was performed on a semi-quantitative/endpoint DNA engine Biorad thermal cycler. Conditions for PCR included an initial denaturation step at 95℃ for 10 min followed by 29 cycles of three steps of denaturation, annealing and extension at 95℃ for 1 min, 68℃ for 2 min, 72℃ for 1 min and a final extension step at 72℃ for 10 min. DNA extracted from healthy adult humans without any sepsis was used as negative control. DNAse, RNAse Free ultrapure water (Sigma) was used as no template control. DNA extracted from pure bacterial cultures—Salmonella typhi, Enterococcus fecalis and Staphylococcus aurous—were used as positive controls. The person performing the 16S rRNA PCR was blinded to the diagnosis of the patients (sepsis/no sepsis). For culture, blood samples were inoculated in brain heart infusion broth and bile broth, incubated and subcultured using standard methods. The sepsis screen included C-reactive protein (CRP), total white cell count (WBC), absolute neutrophil count (ANC), immature to total neutrophil ratio and micro erythrocyte sedimentation rate (ESR). The sepsis screen was considered positive if at least two of the screen parameters were positive. A chest radiograph was performed only if indicated.
CRP assay was performed by the qualitative method of latex agglutination and an agglutination titre of 1:2 dilutions was considered positive. A WBC and an immature to total neutrophil ratio >20% were considered positive. The ANC was considered positive if the value fell outside the limits of normalcy according to the charts of Manroe et al. 6 and Zipursky et al. 7 The micro ESR was considered positive if it was above ‘age in days +3 mm/h’ in the first week of life or >10 mm/h thereafter.
The details of antibiotic treatment and clinical signs of sepsis (decreased acceptance, lethargy, regurgitation of feed, fever, neonatal seizures, excessive cry, tachypnea, sclerema, loose stool, capillary filling time >3 s) were recorded. Patients were categorised as having definite sepsis (clinical diagnosis of sepsis and blood culture positive), probable sepsis (clinical diagnosis of sepsis, positive sepsis screen but sterile blood culture) and no sepsis (septic screen negative and blood culture sterile). The primary outcome was the sensitivity and specificity of the test for the diagnosis of definite (blood culture positive) sepsis. A secondary outcome was its sensitivity and specificity for any sepsis (definite + probable sepsis)
All data were entered into a Microsoft Excel spread sheet by the principal investigator. Data were analysed using SPSS version 20.0 statistical software. All quantitative variables were described as mean (SD) or median (IQR) and all qualitative variables were depicted as a number (proportion). For determining the statistical significance between the two groups, the χ2 /Fisher’s exact test was applied for categorical variables whereas the unpaired Student’s t-test/non-parametric Mann–Whitney test was used for comparing continuous variables. The level of significance was set at <0.05.
Results
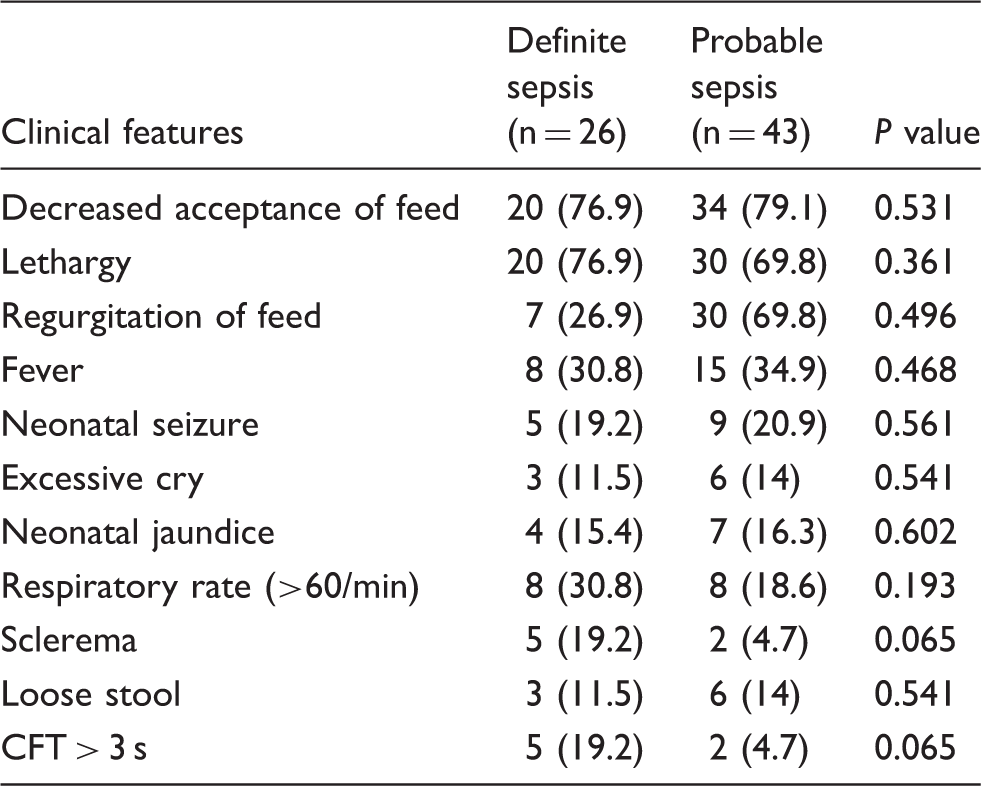
Figure 1 gives the flow of patients in the study. A total of 138 neonates were evaluated for eligibility, of whom 100 were enrolled. The study population had a mean (SD) birth weight of 2324.6 g (±535.2 g), gestational age of 37.1 weeks (±2.4 weeks) and mean age at enrolment of 10.9 days (±8.9 days). Boys accounted for 58% of the participants. Table 1 gives the clinical features of the study population.
Study flow. Clinical features in ‘definite sepsis’ and ‘probable sepsis’ neonates. Values are presented as n (%). SD, standard deviation.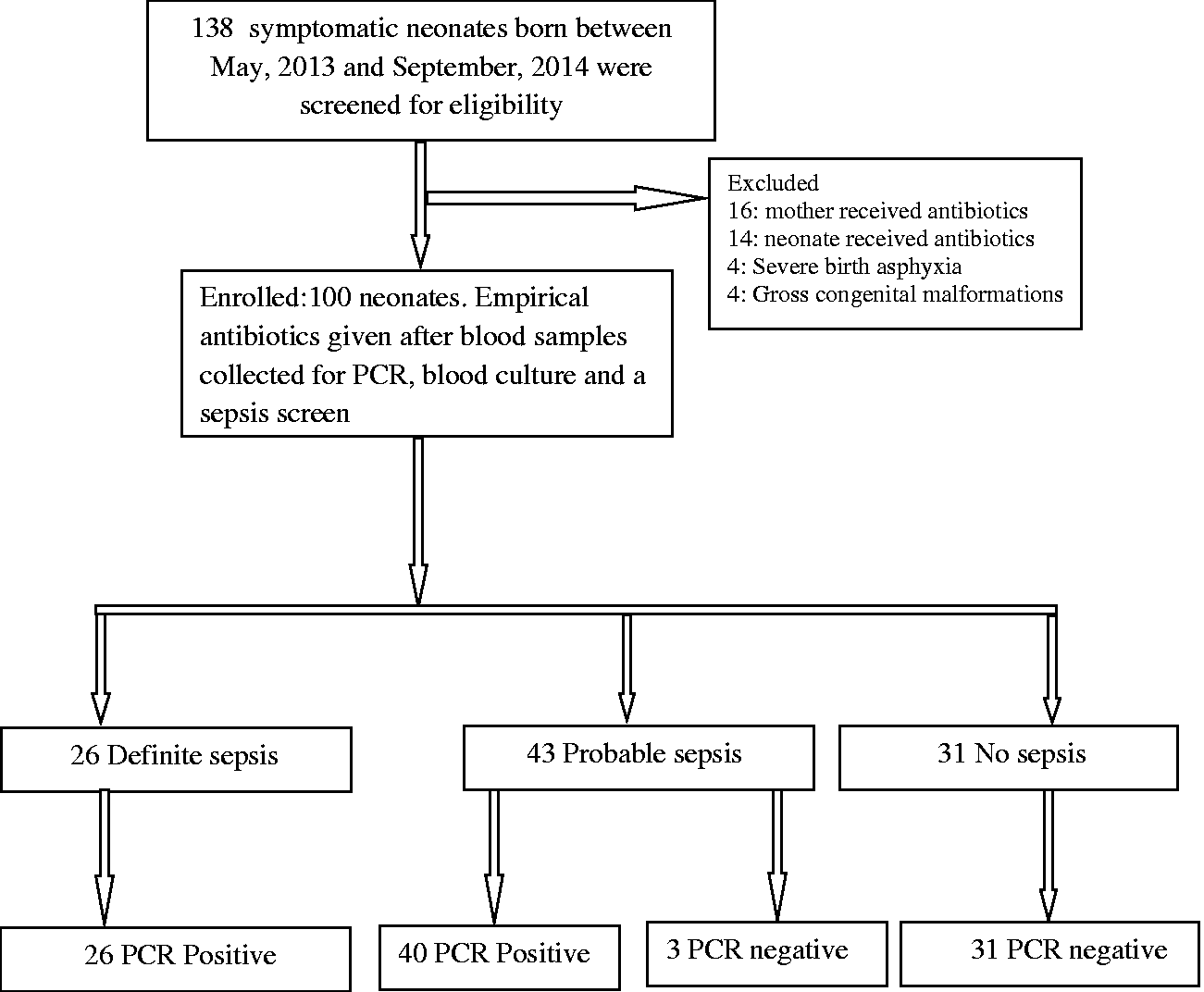
Among the 100 neonates, 26 had definite sepsis and all 26 were PCR positive. A further 43 had probable sepsis of whom 40 were PCR positive and three were PCR negative. The remaining 31 had no sepsis and all were PCR negative.
S. aureus was the commonest isolated pathogen (23%) followed by coagulase negative Staph (19%), Acinetobacter (15%), Enterococcci (15%), Klebsiella (12%), Pseudomonas (8%) and E. coli (8%).
A diagnosis of neonatal sepsis by blood culture revealed 37.7% sensitivity, 100% specificity, 100% positive and 41.89 % negative predictive value. In the definite sepsis group, 16S rRNA PCR revealed a100% sensitivity, 100% specificity, 100% positive and 100 % negative predictive value. In the ‘any sepsis’ group (definite + probable), PCR revealed values of 95.6%, 100%, 100% and 91.2%, respectively.
Discussion
Our study shows that universal primer 16S rRNA PCR is as rigorous as well as being as sensitive and specific a method for diagnosing culture positive bacterial infections. Forty-three cases of probable sepsis where blood culture was negative, PCR was positive in 40. Although the possibility of contamination of PCR cannot be ruled out given the sensitive nature of this test, all 40 cases presented with clinical symptoms and signs of sepsis and all had a sepsis screen that was documented positive. All cases with positive PCR but sterile cultures were true positives and not false positives; this can be explained by the probable low level of bacteraemia and the known lower sensitivity of the gold standard.
By PCR, a diagnosis of neonatal sepsis in 40 (58%) neonates could be made who would have been missed by blood culture, within the short turn-around time (6–8 h) available. PCR had a high sensitivity as compared to blood culture (95.7% versus 37.7%) and high negative predictive value (91.2% versus 41.9%) in neonates with any sepsis. In comparison to blood culture, PCR demonstrated a high negative predictive value for ruling out neonatal sepsis. This necessarily serves to avoid unnecessary antibiotic therapy. 8
PCR in our study meets some of the criteria of an ideal diagnostic test for any neonatal sepsis, but it does not provide information on antibiotic sensitivity and is costly. PCR by itself cannot distinguish between asymptomatic bacteraemia, contamination and true infection.
We conclude, therefore, that 16S rRNA PCR is a useful test for diagnosing neonatal sepsis but larger randomised control trials are needed before it can be recommended for routine clinical use. We do not recommend replacing blood culture by this PCR test, but as an initial diagnostic tool it is powerful.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.