
Abstract
This study was conducted to analyse the clinical characteristics of measles in infants and to compare them with those in older children. Clinical and sociodemographic details of all hospitalised children with suspected measles were recorded and confirmed cases were analysed further. Twenty-four infants and 34 children aged >1 year were included. Most infants were boys and 15 (62.5%) of them were aged <9 months. Early onset of rash (within three days of fever in 62.5% of cases) occurred in infants. The complications of measles in infants included bronchopneumonia (n = 17, 71%), acute diarrhoea (n = 8, 33%), meningitis (n = 1, 4%) and staphylococcal sepsis (n = 2, 8%). The number of infants with complications was significantly high (88% and 65%; P = 0.05). Measles in infants can have atypical presentations, a greater risk for complications and may occur before they are due to receive the conventional first dose of measles vaccine.
Introduction
Measles continues to be a major cause of morbidity and mortality among young children in spite of the availability of a safe and effective vaccine.1–3 India accounted for over one-third of measles mortality in 2015 and is now included in the global crusade for elimination by the year 2020. In India, the national immunisation schedule recommends the first dose of measles vaccine at the age of 9–12 months, and the second dose at 16–24 months.4,5 Immunisation campaigns for all children aged nine months to 15 years and case-based surveillance are part of the elimination strategy. 6
There is increasing recognition of early loss of maternally transmitted antibodies and the occurrence of measles in infants below the age of recommended vaccination.7–9 There are also reported differences in clinical presentation of infants and older children. 3 With renewed public interest in the epidemiology of measles after the launch of the measles rubella campaign, it was decided to analyse data of children admitted with laboratory-confirmed measles. The aim of our study was to analyse the clinical characteristics including risk factors, complications and outcome in infants and to compare them with those in older children.
Methods
Ours was a retrospective study conducted at a referral hospital catering for sick children from five northern districts of Kerala, India. Hospital data of children admitted with suspected measles from January 2014 to December 2016 were analysed. According to hospital policy, all children aged one month to 12 years with suspected measles were admitted if any of the following were present: (1) severe clinical course; (2) uncertain diagnosis; or (3) presence of complications. All children were treated in accordance with World Health Organization (WHO) recommendations.
Serum IgM ELISA or reverse transcription polymerase chain reaction (RT- PCR) on throat swab was done at the Manipal Centre for Virus Research (MCVR) for confirmation of measles infection in all children with clinical suspicion. 10 Data of those children with confirmed measles were analysed regarding sociodemographic characteristics, immunisation status, contact with measles, clinical features, laboratory results, complications and outcome; these data were noted from the hospital records. Clinical characteristics of infants and older children with confirmed measles were compared. Approval from the institutional ethics committee was obtained for analysing the data.
Results
There were 58 children admitted with measles during the study period, confirmed in 42 children by positive RT-PCR on throat swab and in 16 by positive IgM antibody.
Age and gender of infants and older children with measles.
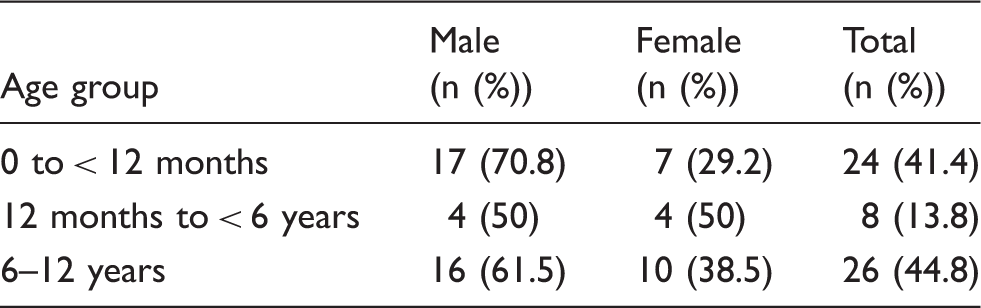
None of the infants had received any measles-containing vaccines (MCV). A single dose of MCV had been administered in 18 (52.9%) children aged >1 year and one child developed measles despite two doses of MCV. A history of contact with measles could be elicited in 6/24 (25%) infants, of whom one had a history of maternal measles. Three children aged <9 months visited hospital during the incubation period.
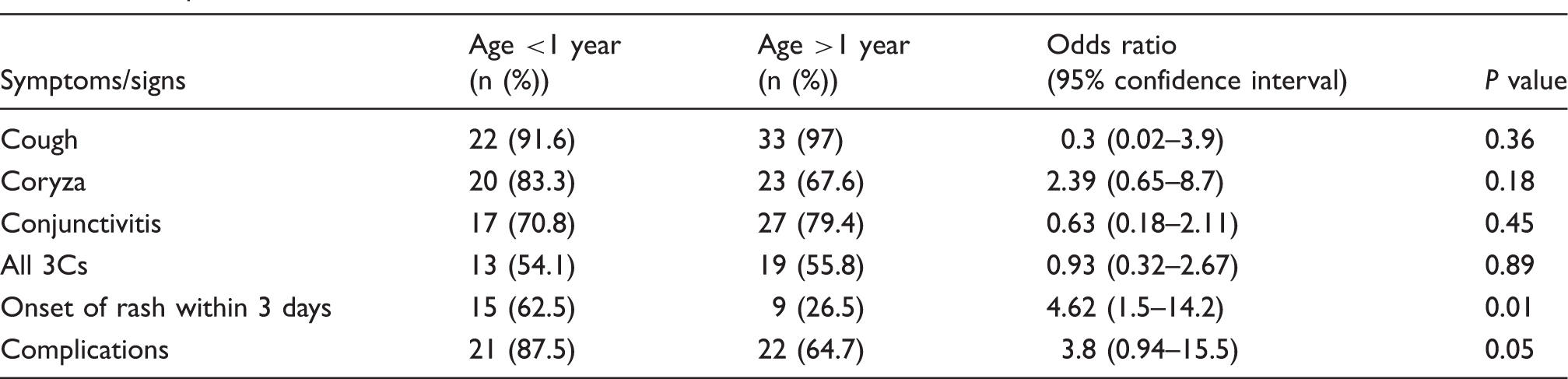
A rash appeared within three days of onset of fever in 15/24 (62.5%) infants, of whom 3/24 (12.5%) developed a rash on the first day of fever. Koplik spots were documented in 5/24 (21%). Though oral mucosal erythema was present in 10/24 (42%), none of them had oral ulcers. The classic symptoms of measles, namely cough, coryza and conjunctivitis, were recorded in 22 (91.6%), 20 (83.3%) and 17 (70.8%) children, respectively.
Nutritional anaemia was present in 11/24 (46%) children; 5/24(21%) had varying degrees of protein energy malnutrition. Two babies had a primary immune deficiency disorder. One six-month-old baby had Di George syndrome and a seven-month-old boy had a suspected T cell disorder with BCG adenitis.
The most common complication of measles was bronchopneumonia (n = 17, 71%) followed by acute diarrhoea (n = 8, 33%). Meningitis (n = 1, 4%) and staphylococcal sepsis (n = 2, 8%) were other complications noted. The mean duration of hospital stay was six days (range = 2–25 days). One infant with suspected primary T cell immunodeficiency developed bronchopneumonia and died before the exact cause could be ascertained.
A rash occurred within three days of onset of fever only in 9/34 (26.5%) children aged >12 months (mean age = 6.6 years; age range = 2–10 years) and none of them had rash on day 1. Koplik spot were noted in 17/34 (50%) of children aged >1 year. Cough, coryza and conjunctivitis occurred in 33/34 (97%), 23/34 (67.6%) and 27/34 (79.4%) children, respectively. Common complications of measles in older children were also bronchopneumonia (n = 17, 50%) and acute diarrhoea (n = 5, 15%). A two-year-old girl treated with maintenance chemotherapy for acute lymphoblastic leukaemia died due to bronchopneumonia as a complication of measles.
Comparison of clinical features of measles in infants and older children.
Discussion
We found that significantly more infants with measles had complications compared to older children, even though their nature was similar. Bronchopneumonia was the most common in both infants and older children, but those aged <9 months had more severe infections. Atypical presentations are common in measles in infancy, and the clinical features may be modified by the presence of maternal antibodies. We observed measles in significant numbers among infants aged <9 months, the recommended age of first dose of measles vaccine in India. It is possibly due to the early waning of maternal antibodies after vaccination as opposed to immunity following natural infection.7,8 The B3 subtype of measles was recorded in Thiruvananthapuram, commonly present in certain regions of Africa, 11 in two-thirds of infants aged <12 months. We could not undertake viral genotyping, so cannot comment on the responsible types in our sample. However, other studies have also reported the occurrence of new genotypes of measles virus in India.5,12
It is a moot point whether a supplementary dose of measles vaccine should be administered at the age of 6 months (MCV0) as recommended by the WHO in outbreak situations. 13 The finding that >50% of older children in our sample who developed measles had received a single dose of measles vaccine points, however, to the need for additional doses of the vaccine.
Hospital visitation was the largest risk factor for measles infection in Chinese infants aged 0-7 months. 9 As recorded in our sample, the three infants may have benefitted from hospital infection control programmes and educating mothers regarding the importance of protecting unvaccinated infants to risky exposure to measles.
Infants younger than the age at which routine MCV is recommended need special attention, since they throw up unique challenges. The WHO recommends that countries should build their own evidence base to determine age-specific immunity gaps and determine the target age range for measles and MR campaigns. 13 We also point to the need to evaluate maternal antibody titres over time.
The generalisation of our findings should be taken with caution, as they are from one hospital only.
Conclusions
More extensive preventive strategies need to be evolved urgently if the goal of measles elimination by 2020 is to be achieved.
Footnotes
Acknowledgements
The authors thank Dr G Arunkumar, Professor and Head, Manipal Centre for Viral Research, Manipal University, Karnataka for conducting the virological tests. They also thank the faculty at the Department of Paediatrics, especially the head of the department, Dr M Vijayakumar, who were involved in the care of these children.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.