
Abstract
Rabies has two distinct clinical syndromes, encephalitic (or ‘furious’) and paralytic (or ‘dumb’). The paralytic form presents as acute flaccid myelitis and is more common in patients who received post-exposure anti-rabies vaccination without rabies immunoglobulins. We have recently had the opportunity to manage a middle-aged man presenting as ‘dumb’ paralytic rabies.
Case report
A 50-year-old man was admitted to the emergency department of a tertiary care hospital in north India with left lower limb weakness. Three weeks before admission, while working in his field, he was bitten on the left leg by a stray dog, sustaining a category III wound, which he washed with water, applying Capsicum powder. The following day, at a primary health centre, post-exposure anti-rabies vaccination with four doses of a purified Vero cell rabies vaccine (trade name Abhayrab) was commenced. He did not receive rabies immunoglobulins. Three days after vaccination completion, he developed left lower limb weakness, progressing rapidly to involve the right lower limb followed by both upper limbs within 24 h, combined with urinary and faecal retention.
On examination, he was alert and oriented, with normal vital signs. His higher mental functions appeared normal. Generalised muscular fasciculations were seen over all four limbs and the upper chest.
Cerebrospinal fluid (CSF) analysis showed 240 leucocytes/µL (60% lymphocytes, 40% neutrophils), protein 124 mg/dL and glucose 2.8 mmol/L. A 3-T magnetic resonance imaging (MRI) revealed increased T2-weighted (T2W) signal in the long segment of the spinal cord (Figure 1a), the basal ganglia and the midbrain (Figure 1b). Subsequently, rabies virus-specific neutralising antibodies were detected in CSF by a rapid fluorescence focus inhibition test. A diagnosis of paralytic rabies was made and supportive management was started. However, rapid deterioration ensued, with the development of encephalitis and respiratory failure; our patient died on day 10 of his illness.
(a) MRI spine showing revealed increased T2W signal in the long segment of the spinal cord (arrows). (b) MRI brain showing increased T2W signal in the basal ganglia (arrows) and the midbrain (arrowhead).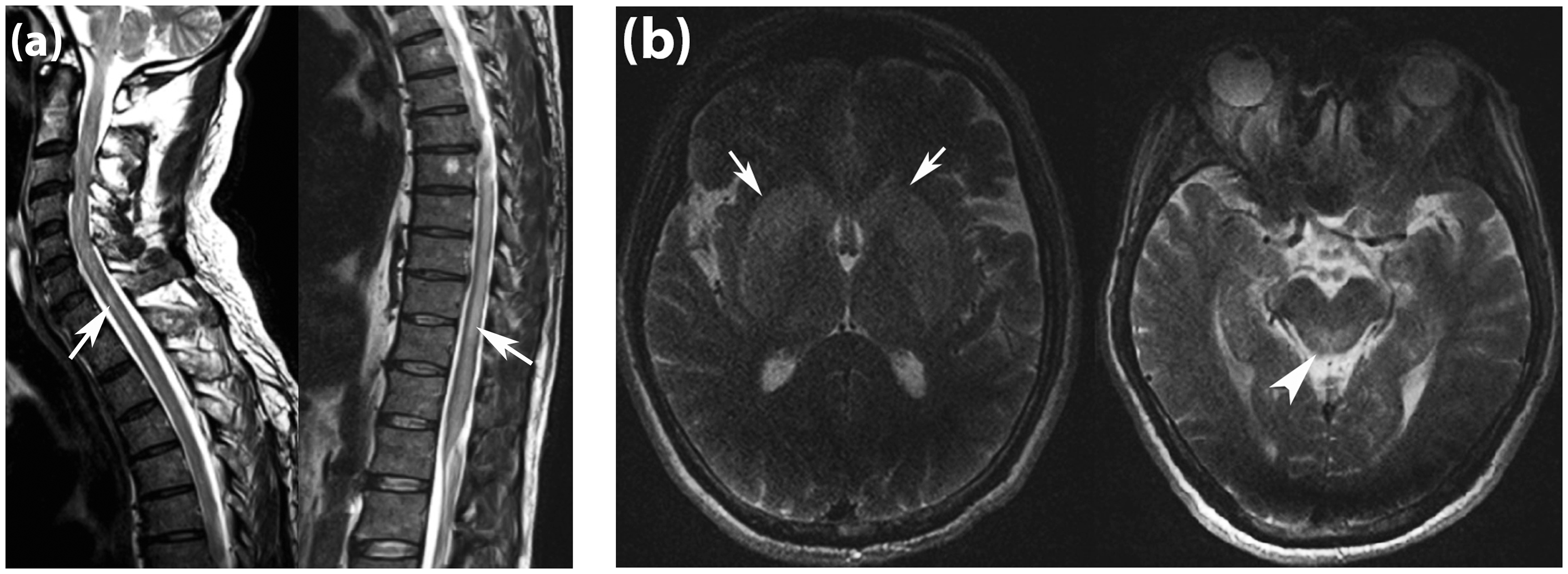
Discussion
Rabies may cause an acute flaccid myelitis (AFM). The disease presents in this paralytic form in 20% of cases. The cardinal features of encephalitis, hydrophobia, aerophobia, agitation and anxiety are absent. The pathogenesis involves the centripetal spread of the virus along peripheral nerves to the spinal cord, in contrast to spread to the limbic system and brain stem as in encephalitic rabies. Paralytic rabies usually occurs after inadequate post-exposure management, i.e. anti-rabies vaccination without rabies immunoglobulins, incorrect administration of the vaccine or immunoglobulin or exposure to bites of vampire bats.1–4
The clinical presentation mimics Guillain–Barre syndrome or polyradiculitis. Moreover, the former may occur as a complication of the rabies vaccine. Points favouring the diagnosis of rabies are the presence of fever, urinary dysfunction, muscle fasciculation, altered sensorium, CSF pleocytosis and an abnormal spine MRI scan, typified by spinal cord involvement demonstrating T2 hyperintensity spanning more than one vertebral segment. Limb weakness in AFM is frequently asymmetric, and may range from monoplegia to quadriparesis, and is usually preceded by a viral prodrome with fever or a mild respiratory illness. CSF examination reveals a lymphocyte-predominant pleocytosis with elevated protein levels. The underlying specific aetiology of AFM is still debated; however, a virus that triggers an autoimmune process leading indirectly to paralysis is a potential cause. 5 Enteroviruses, flaviviruses and adenoviruses are among the common causes, poliovirus being the commonest culprit of the past. However, enterovirus EV-D68 or EV-A71 associated prodromal respiratory illness was seen in most cases of recent AFM outbreaks in North America. 5 Rabies, being a serious public health problem in low- and middle-income countries, remains an important cause of AFM and is mainly attributed to bites from unimmunised dogs and inadequate post-exposure management.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.