
Abstract
Orbital trauma is often associated with foreign bodies. Wooden foreign bodies pose an urgent need for removal owing to their reactive nature and the high risk for infection. Though visual prognosis depends on associated ocular trauma, in selected cases, excellent visual and cosmetic outcomes are possible. An 18-year-old woman presented to our trauma facility with a history of fall directly onto a wooden stick from a height. On examination, there was a large wooden foreign body in the left medial orbit, extending into the ethmoidal sinus as visualised on imaging. After administration of perioperative antibiotics, the foreign body was removed in toto using careful tissue dissection and the soft tissue was closed in layers. Postoperatively at six months, the vision in the left eye was 20/20 with mild ptosis. Early surgery, careful dissection of soft tissues and adequate infection prophylaxis can lead to good outcomes in such cases.
Case report
An 18-year-old woman presented to our centre having fallen 3 h before from a height on to a wooden stick with the resultant foreign body penetrating the left eye. Right ocular examination was within normal limits; there was a piece of wood penetrating the left orbit through the medial canthal region of the left eye (Figure 1a). Eye-opening was limited, not allowing further ocular examination. General physical examination was normal with no injury elsewhere. A plain computed tomography scan of the orbits and head revealed that the large hypodense foreign body in the medial orbit extended into the ethmoidal sinus (Figure 1b). The globe appeared to be preserved.
(a) Wooden foreign body seen in the medial aspect of the orbit, (b) CT scan showing a hypodense mass in the medial orbit with extension into the ethmoid sinus and (c) the extracted wooden foreign body measuring 5 × 1 × 1 cm. (d) Follow-up at six months postoperatively.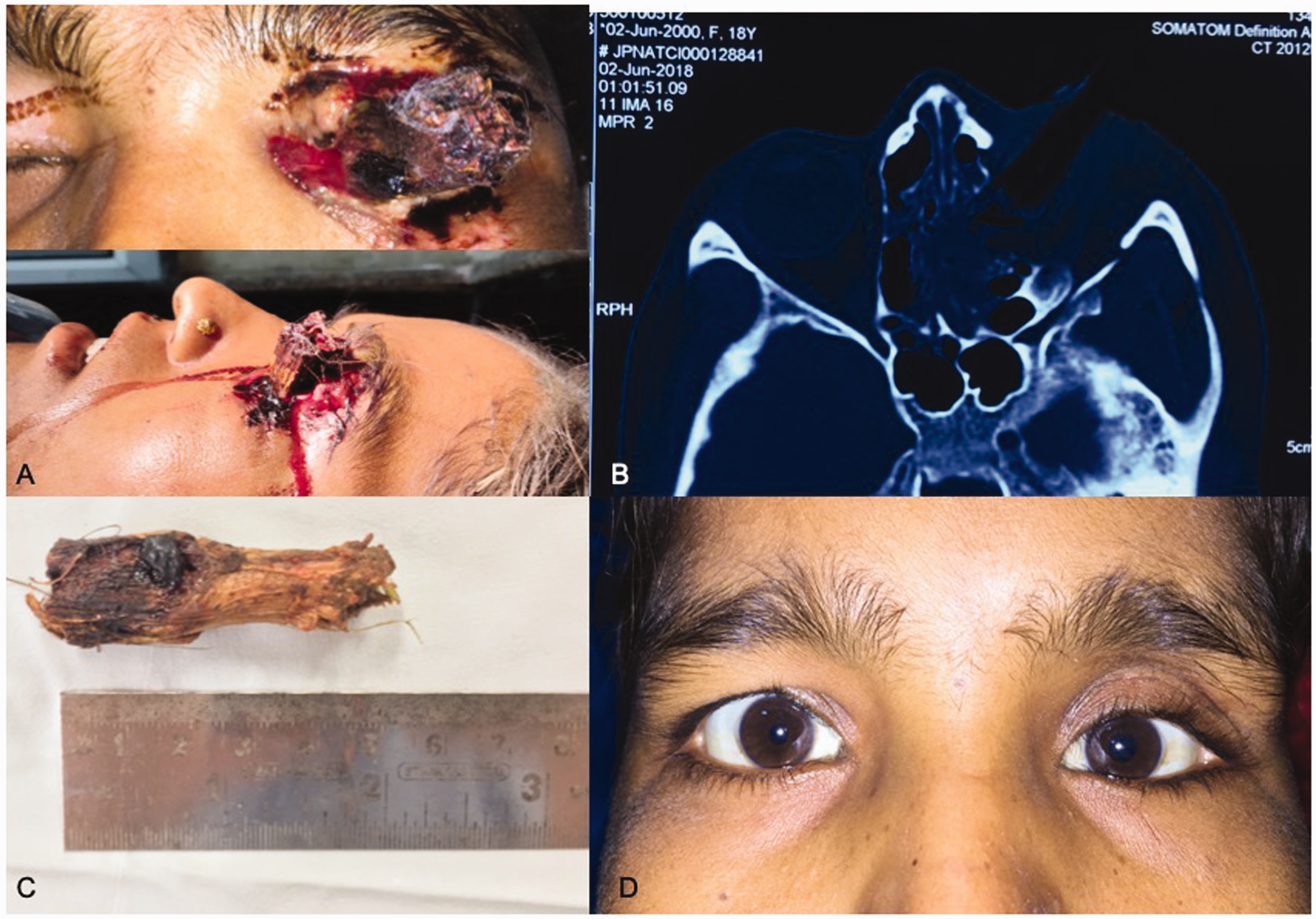
Immediate surgery was arranged after administering perioperative antibiotics. Enlarging the wound of entry, the surrounding tissues were carefully dissected and retracted; after separation of adhesions, the foreign body measuring 5 × 1 × 1 cm (Figure 1c) was pulled out in toto. Remaining splinters were looked for and removed with the help of an adrenaline-soaked gauze. The site was irrigated with normal saline followed by antibiotic and antifungal solution for 1 min each. At intraoperative examination, the globe was found to be intact. There was a large laceration in the upper lid at the entry site which was repaired in layers. Postoperatively, systemic antibiotics and anti-fungal agents, along with topical antibiotics and steroids, were continued.
On the first postoperative day, the visual acuity of the left eye was 20/40 and the pupil was reacting briskly. Ocular examination was otherwise unremarkable. At one-month follow-up, it improved to 20/20. However, there remained some compensatory lid retraction on the right side. At six-month follow up, there was no diplopia (Figure 1d) and normal extra-ocular movements were found.
Discussion
Orbital trauma is a common clinical scenario in any ophthalmic practice. Approximately one out of every six cases of penetrating orbital trauma is associated with a foreign body. 1
Wooden foreign bodies, being organic and thus reactive, require urgent removal. 2 The pores in their substance may act a nidus for bacteria, leading to higher rates of abscess, granuloma and orbito-cutaneous fistula formation, and osteomyelitis. 3
Optimal visualisation of the site of impaction and the whole tract of the foreign body is essential while operating in such cases. Large wooden pieces often tend to involve adjoining structures along with the orbit such as the sinuses, infratemporal fossa, nasal cavity and even the cranium.4,5 In such cases, it may be necessary to enlist a multidisciplinary team. 1 Splinters are peculiar to wooden foreign bodies, and if not completely removed, may lead to persistent infection. 6 The use of an adrenaline-soaked gauze can help with their removal as it reduces local vascularity. Surgical debridement of the surrounding necrotic tissue, if any, and irrigation of wound site with copious amounts of antibiotic solution is essential.
Large foreign bodies may slip between the globe and orbital walls, thus causing little or no damage to intraocular structures. However, the impact of the immediate direct trauma may damage intraconal structures, such as the optic nerve. Periosteal breach by foreign bodies may lead to the formation of a hematoma and increased chances of intracranial involvement via the superior orbital fissure or optic nerve foramen. 7 There are very few reported cases describing orbital trauma with large wooden foreign bodies where good visual acuity is preserved.4,5
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.