
Abstract
Primary hyperparathyroidism is not so uncommon a disease. In high-income countries, with the introduction of routine biochemical testing in 1980s, it is diagnosed early, and the majority are seen as asymptomatic disease. However, in India, a severe symptomatic form is still seen, and many times patients are undiagnosed, thus continuing to suffer debilitating disease. Here, we report such a patient who was being treated as having bony metastases from an unknown primary source, when in fact he had osteitis fibrosa cystica due to primary hyperparathyroidism and was cured after surgery.
Case report
A 45-year-old male was referred to our hospital with paraplegia for six months with a diagnosis of vertebral metastasis from an unknown primary. He had bony pain over both lower limbs for three years, bony swelling over the left clavicle (Figure 1(a)) and inability to walk for six months. He also had bilateral multiple renal stones for one year. He had consulted multiple physicians over the years. On presentation, his serum calcium was very high (3.49 mmol/L), serum parathormone (PTH) 84.8 pmol/l and alkaline phosphatase level 5.2(mu)kat/l. His vitamin D levels were adequate and serum creatinine was normal. A skeletal survey revealed multiple lytic expansile lesions involving both femurs, tibiae and fibulae, with similar lesions involving the metacarpals, phalanges and both radial epiphyses. Acro-osteolysis of phalangeal tufts was noted with subperiosteal resorption in the phalanges (Figure 1(b)). On CT study, multiple lytic expansile lesions were noted in the spine involving the vertebral body, transverse processes, vertebral posterior elements, left sternoclavicular joint (Figure 1(c)). A 4D non-contrast CT scan revealed an iso-dense mass in the left side of the neck posterior to the left thyroid lobe. The lesion showed enhancement in the arterial phase and washout on venous phase (Figure 1(d)).
(a) Clinical photograph showing bony swelling over left sternociavicular joint (brown tumour), (b) skeletal X-ray showing multiple lytic bone lesions (marked with arrow) over left femur and left tibia and fibula, acro-osteolysis of phalangeal tufts with subperiosteal resorption in phalanges (circled), (c) CT showing expansile lytic bony lesions involving sternoclevicular joint bilateral should joints (circled) and vertebral body (marked with arrow), (d) CT showing parathyroid posterior to left thyroid lobe, (e) operative view after port placement for trans-oral vestibular parathyroidectomy, (f) endoscopic view showing mobilisation of parathyroid adenoma and (g) excised en bloc parathyroid adenoma with left lobe of thyroid.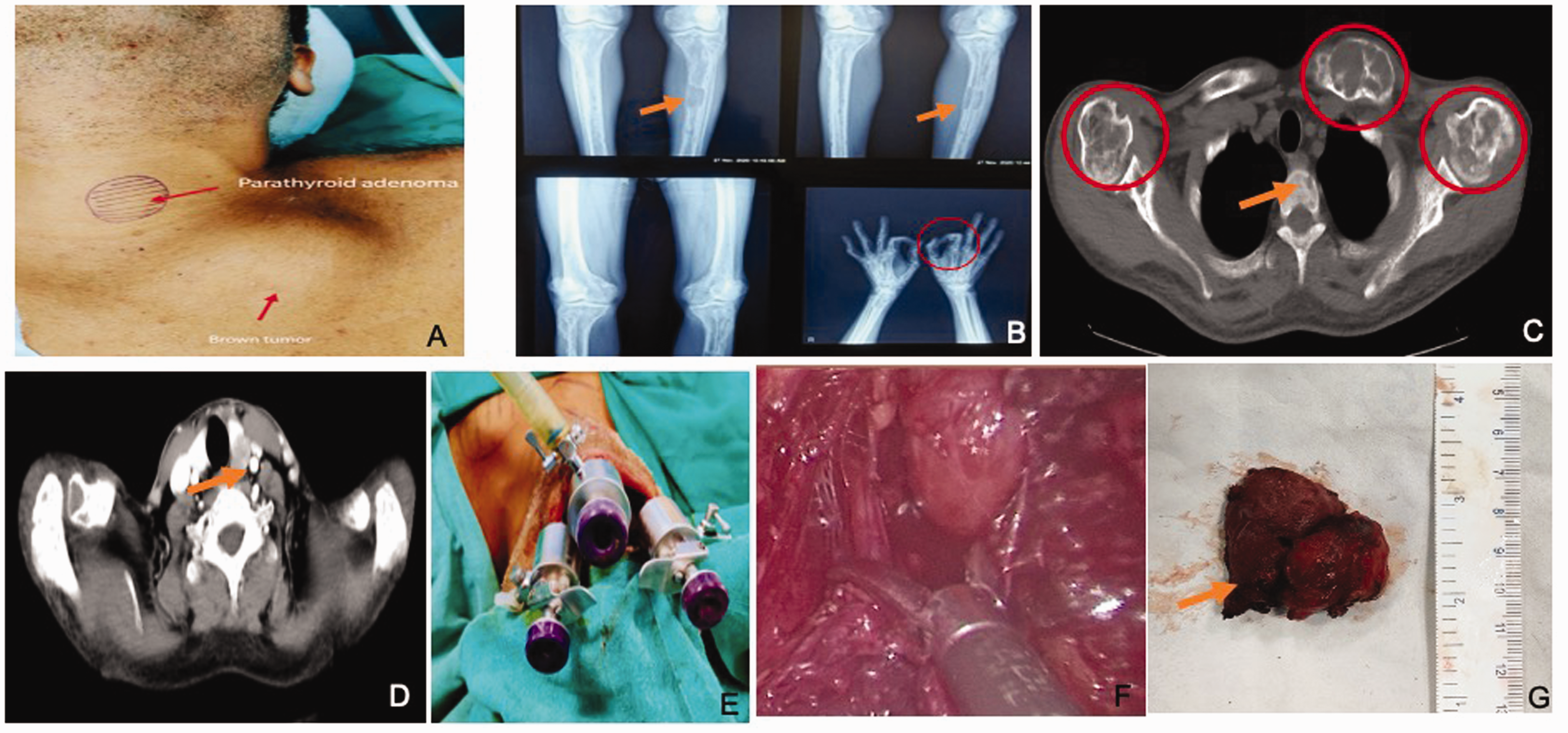
After his hypercalcaemic crisis was corrected with forced diuresis (hydration and furosemide intravenously), he underwent trans-oral en-bloc endoscopic parathyroidectomy with left hemithyroidectomy (Figure 1(e) to (g)). Intraoperative neuromonitoring was not used. Our patient developed biochemical hypocalcaemia on the second post-operative and symptomatic hypocalcaemia the following day. He was started on intravenous calcium infusion along with oral calcium and vitamin D supplements, with which the serum calcium levels returned to within normal limits. After three months’ follow-up, his calcium level and serum PTH levels are normal, and he is now able to walk. The final histopathology was reported as a benign parathyroid adenoma.
Discussion
The presenting characteristics of PHPT in India have also changed over the years with less severe disease. However, the majority of Indian PHPT patients are symptomatic but with milder form of disease.1,2 Our patient presented with the classical hypercalcaemic ‘stones, bones, moans and groans’. However, his true diagnosis was delayed owing to the detection of multiple osteolytic lesions usually associated with metastatic involvement of the bone; however, metabolic bone disease should still have been included in the differential diagnosis.
Biochemical diagnosis of PHPT is established with raised calcium and serum PTH levels. As technetium 99m sesta-methoxyisobutylisonitrile scanning is not available at our centre and the superior accuracy of four-dimensional CT allows it to be used as the sole pre-surgical localisation method, 3 we used it to confirm the source of the tumour in left inferior parathyroid. Our centre does not have the facility of intra-operative PTH monitoring and frozen section biopsy. Nonetheless, we were able to perform a focused parathyroidectomy using an endoscopic approach based on our previous experience 4 and patient was cured of his disease.
Conclusion
In the era of affordable biochemical testing, patients with bone pain, renal diseases and acute pancreatitis should be screened for PHPT so that early diagnosis can be made. A greater awareness amongst general population and treating physicians is required.
Footnotes
Ethical approval
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional and/or national research committee and with the 1964 Helsinki declaration and its later amendments or comparable ethical standards.
Informed consent
Informed consent was taken from the patient.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.