
Abstract
Our was an observational follow-up study where the aim was to assess the baseline high-sensitivity C-reactive protein levels in 50 smear-positive pulmonary tuberculosis patients in association with socio-clinico-radiological profile and microbiological conversion. Smear and culture conversion of sputum samples at the end of intensive phase of anti-tubercular treatment were recorded. Baseline serum high-sensitivity C-reactive protein estimation was done by ELISA. Mean high-sensitivity C-reactive protein levels at baseline, smear/culture converted and delayed converters were 68.1 ± 22.2 mg/l, 66.7 ± 22.0 mg/l and 91.6 ± 6.7 mg/l, respectively; high-sensitivity C-reactive protein levels were significantly higher in delayed converters as compared to sputum converters. Significantly higher baseline high-sensitivity C-reactive protein levels were seen in patients with bilateral chest X-ray lesions, cavitations, evening rise of temperature, haemoptysis and dyspnoea as compared to those without these features. high-sensitivity C-reactive protein, being a non-specific inflammatory marker could be an adjunct tool for TB prognosis.
Introduction
Tuberculosis (TB), one of the oldest global diseases, is still a major cause of ill health. Not only is tuberculosis one of the top 10 causes of death worldwide, it is also the leading cause of death from a single infectious agent. 1 Most cases can be cured and transmission curtailed with timely diagnosis and good adherence to treatment. Patients having active pulmonary tuberculosis (PTB) with positive sputum smears are the main source of infection, 2 because the droplets expelled are laden with infectious bacilli. One untreated infectious tuberculosis patient is likely to infect 10 to 15 persons annually. 3 Sputum smear conversion is defined as the change of initial sputum smear-positive status to smear negative after treatment. Smear conversion rate (SCR) at two months of intensive phase (IP) of antitubercular treatment (ATT) is an important operational indicator of a TB control programme to check its ability to retain patients on treatment as well as to provide evidence for treatment response. 4 Absence of infectivity is best documented by demonstration of culture conversion. 5 However, culture reports take a long time to arrive, and this makes it a poor tool for use in infection control. On the other hand, smear microscopy, although less sensitive than culture, is simpler and faster. 2 There are no well-established host-derived biomarkers predictive of clinical outcome which will, in turn, help identify cases at higher risk of poor outcome (i.e. delayed conversion or treatment failure). Also many patients cannot provide sputum samples for microbiological examination after a few weeks of treatment, as the volume and quality of sputum decreases. A blood-based marker would, unlike sputum, still remain available throughout. The high-risk patient thus identified could then be intensively monitored. This would help clinicians in adjusting treatment protocols to improve outcome.6,7
C-reactive protein (CRP) is an acute phase protein, acting as part of the innate immune response by binding to ligands such as phosphocholine on dead or dying cells and to bacteria. This leads to the activation of complement C1q and the classical complement pathway, which in turn promotes phagocytosis. CRP is mostly produced in the liver in response to Il-6, Il-1β and TNFα secretion. Its rate of production is reflected by its serum level, as it is well preserved but has a relatively short half-life of 19 h. CRP therefore acts as a biomarker of disease activity. 8
Recently, immunoturbidimetric assays have improved analysis of very low levels of CRP through newer kits with sensitivity up to 0.1 mg/L, which is why it is used as a prognostic marker of chronic inflammation in patients with cardiovascular diseases, diabetes, etc. 9 Various studies have shown high-sensitivity C-reactive protein (hsCRP) to have higher sensitivity for pulmonary TB as compared to other inflammatory markers.9–12 hsCRP, being such a non-specific marker, is less helpful if used alone for diagnosis and prognosis of TB, but preferably included as an adjunct marker in multiple biomarker signature. 12
The aim of our study was to correlate the baseline serum hsCRP levels in smear-positive pulmonary TB patients with their socio-clinical and radiological profile.
Material and methods
Our study was by observational follow-up, conducted in the Departments of Microbiology, Medicine and DOTS centre, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi from November 2018 to April 2020. Patients with any symptoms and signs suggestive of TB, including cough >2 weeks, fever > 2 weeks, significant weight loss, haemoptysis, any chest radiographical abnormality were considered as presumptive pulmonary TB. 13 Case record forms where detailed patient history and investigations were recorded, and informed consent was obtained. Ethical clearance was obtained from the Institutional Ethics Committee-Human Research of the University College of Medical Sciences.
Smear-positive pulmonary tuberculosis patients aged ≥16 years before treatment initiation were included in the study. Patients with concomitant inflammatory conditions such as rheumatoid arthritis, inflammatory bowel disease, HIV, pregnancy, burns, malignancy, cardiac conditions such as myocardial infarction, serious illness with multi-organ dysfunction and category II patients who had taken ATT in the previous six months before the date of recruitment, and post-operative cases, were excluded from the study.
Collection and processing of sputum specimens were performed at baseline before treatment initiation and were repeated at the end of the intensive phase of ATT. Direct smears were made, and Zeihl Neelsen (ZN) stained along with RNTCP (Revised National Tuberculosis Control Program) smear grading, from baseline and follow-up sputum samples and cultures, were inoculated on Lowenstein Jensen (LJ) media according to RNTCP guidelines. 13 The NALC-NaOH method was used for sputum decontamination and digestion. 13 ZN staining and MPT64 antigen test (SD BIOLINE TB Ag MPT64 rapid test kit, Republic of Korea) were used for confirming suspected Mycobacterium tuberculosis growth on LJ media. 14 Smears and culture converters were those patients whose specimens were negative at the end of IP, whereas delayed smears or culture converters were those patients whose sputum remained smear and culture positive at the end of IP.
Biosafety cabinet II along with personal protective equipment were used for processing the specimens and cultures. Five per cent phenol was used for discard, and 1% sodium hypochlorite was used for spills.
Peripheral venous blood (3 ml) was collected which was centrifuged and sera were stored at −20℃ till further testing. Sera from 20 healthy controls, matched for age and sex, were obtained to estimate baseline control levels of serum hsCRP, measured by ELISA (XEMA CRP ULTRA ELISA kit. The principle of this test is a sandwich enzyme immunoassay where specimen antigen is captured between specific murine monoclonal antibodies coated onto the microwell surface and second murine monoclonal antibodies to human CRP, labelled with peroxidase enzyme. Enzymatic activity bound to the microwell surface is quantified by addition of chromogen–substrate mixture, stop solution and photometry done at 450 nm where the optical density is directly related to the level of analyte in the specimen.
Data analysis was done by SPSSv23. Serum hsCRP levels were measured as mean and standard deviation. Independent sample ‘t’ test was used when comparing two groups for continuously distributed data. Wilcoxon Test and Chi-squared test were used for group comparisons for non-normally distributed and categorical data, respectively. Fisher’s exact test was used in case the expected frequency in the contingency tables was found to be <5 for >25% of the cells. Linear correlation between two continuous variables was explored using Pearson’s correlation and Spearman’s correlation for normally and non-normally distributed data, respectively. p < 0.05 was considered statistically significant.
Results
The age of 50 smear-positive TB patients ranged from 16 to 62 years (mean 33.8 ± 11.7). The largest proportion of cases (34%) was in the age group of 21–30 years. Males made up 68% (Figure 1).
Age and gender distribution of smear-positive pulmonary TB cases (n = 50).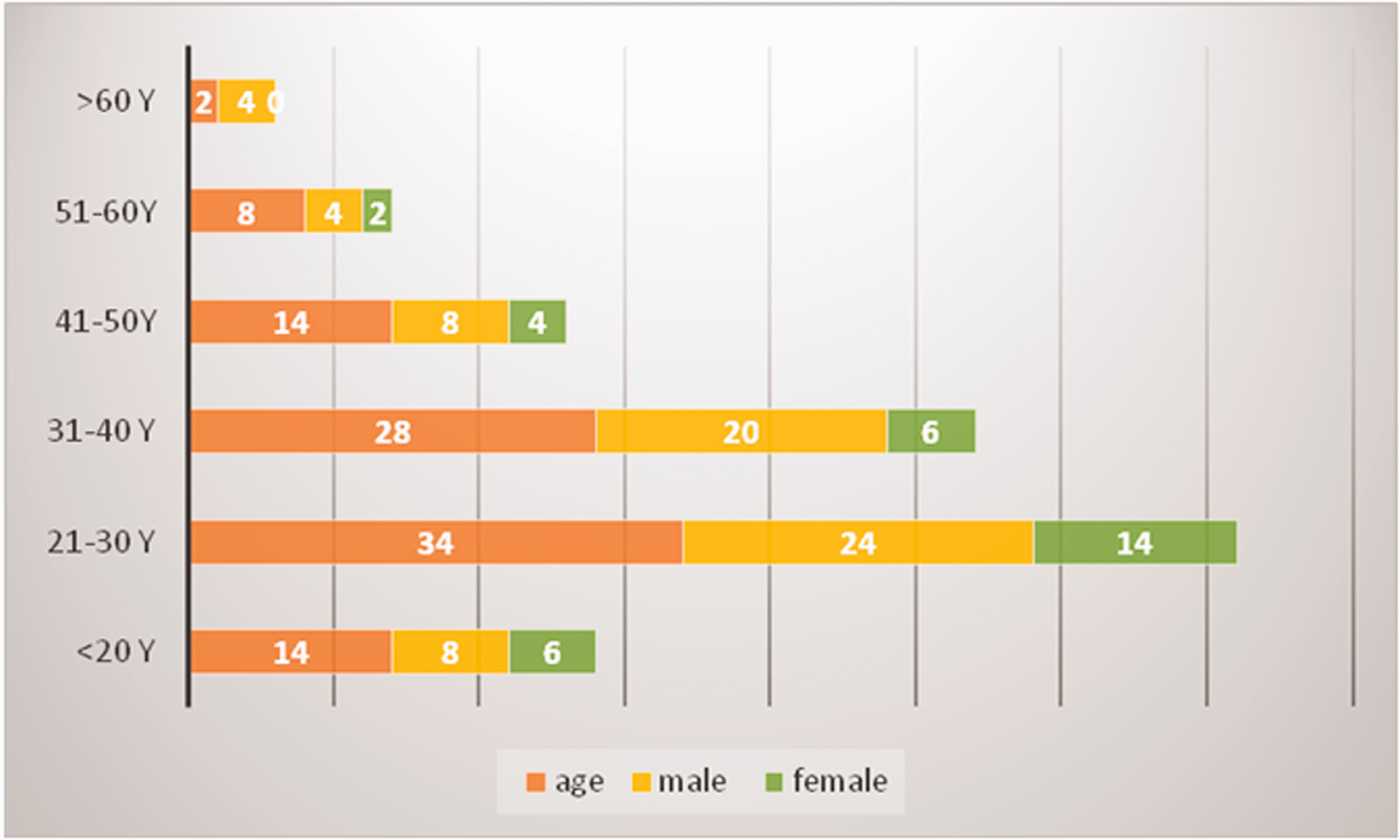
Smear and culture conversion were shown by 94% of the pulmonary TB cases at the end of the intensive phase of ATT.
Mean baseline serum hsCRP levels in various groups of smear-positive pulmonary TB cases (n = 50).
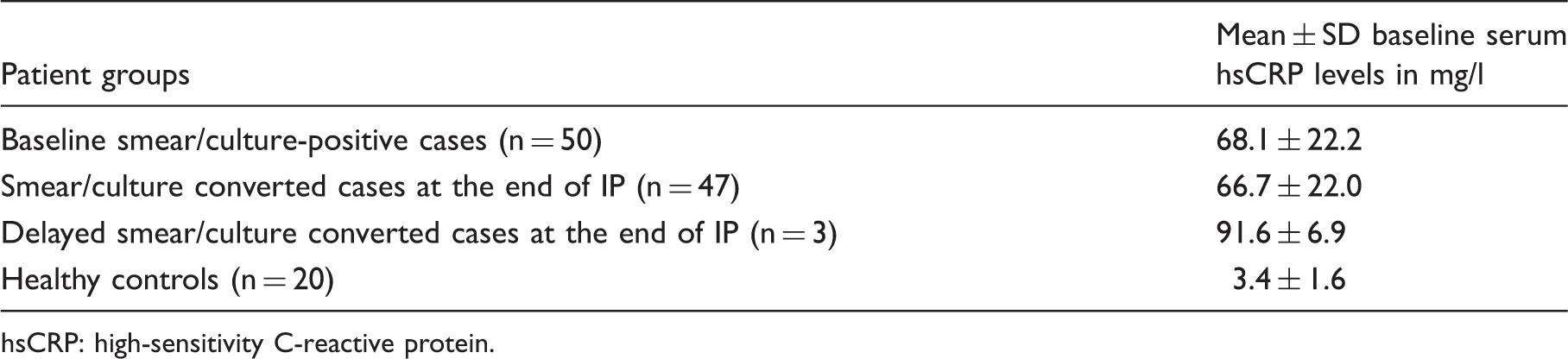
sCRP: high-sensitivity C-reactive protein.
Comparison of baseline serum hsCRP levels among the six age groups, gender, treatment category and socioeconomic classes (n = 50).
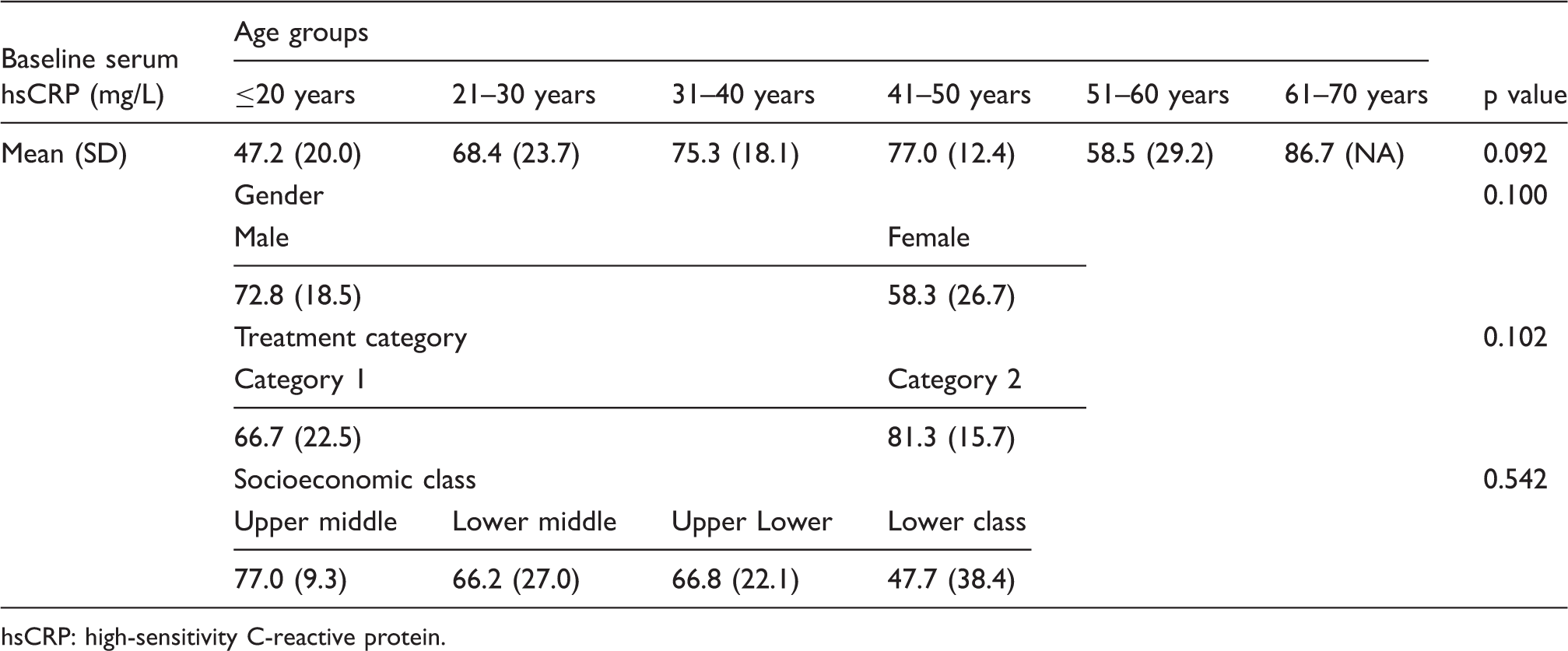
sCRP: high-sensitivity C-reactive protein.
Association between baseline serum hsCRP levels and clinic-radiological findings of smear-positive pulmonary TB patients (n = 50).
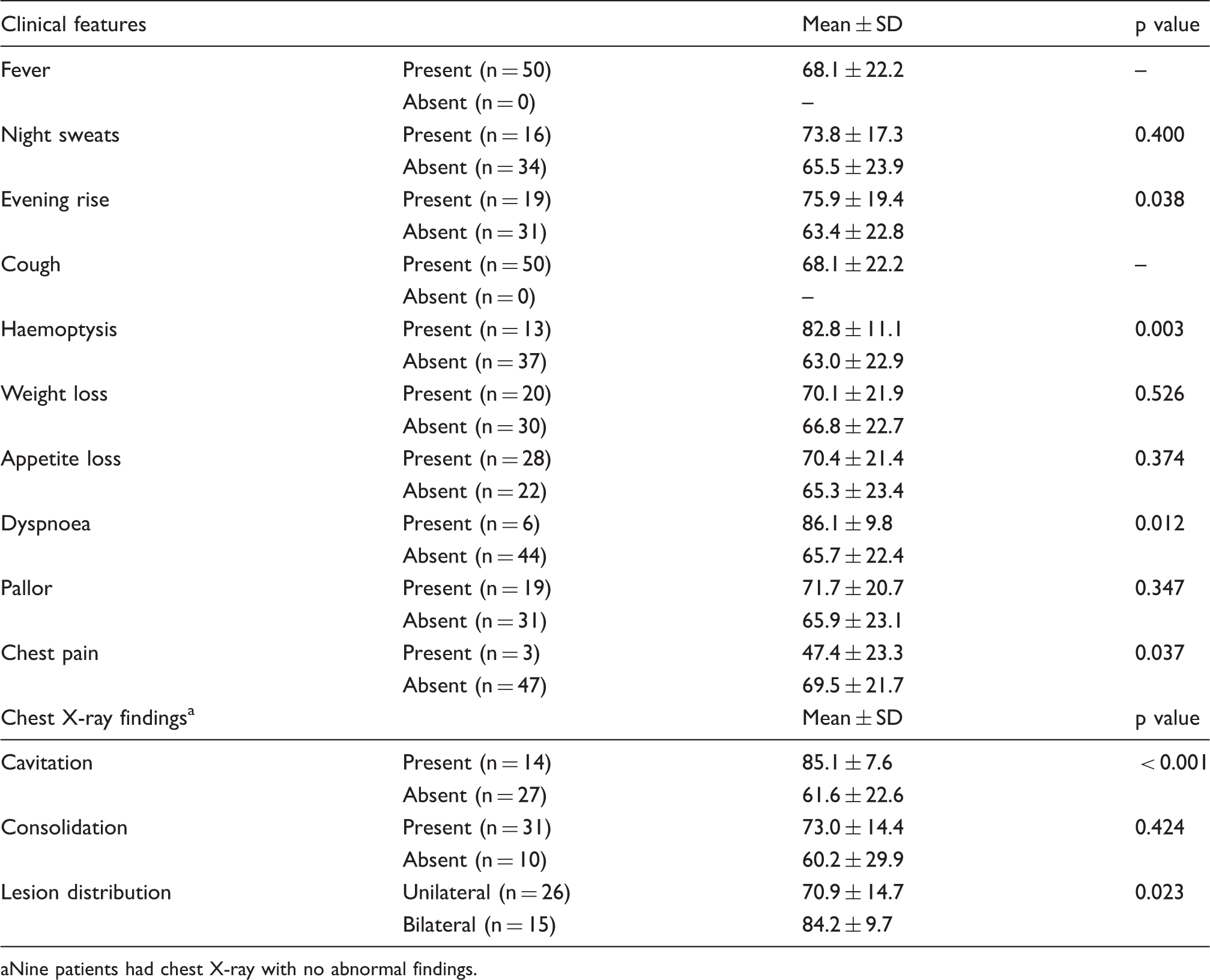
Nine patients had chest X-ray with no abnormal findings.
Association between baseline serum hsCRP levels and additional socio-clinico-demographic findings in smear-positive pulmonary TB cases (n = 50).
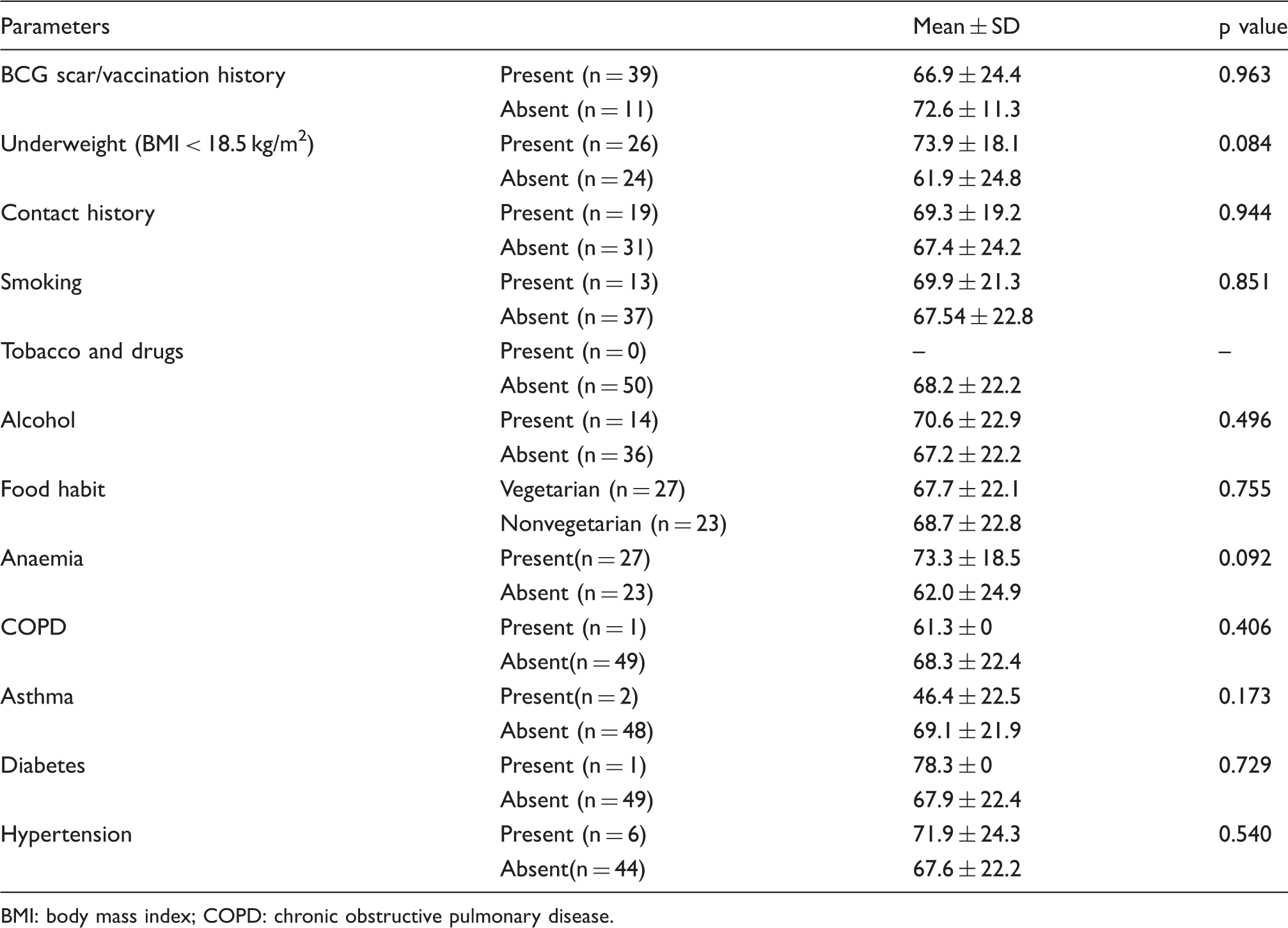
BMI: body mass index; COPD: chronic obstructive pulmonary disease.
There was a strong statistically significant positive correlation between ESR levels and baseline serum hsCRP levels (rho = 0.63, p ≤ 0.001) as shown in Figure 2.
Scatter plot for depicting correlation between ESR values and baseline serum hsCRP levels in smear-positive pulmonary TB patients (n = 50).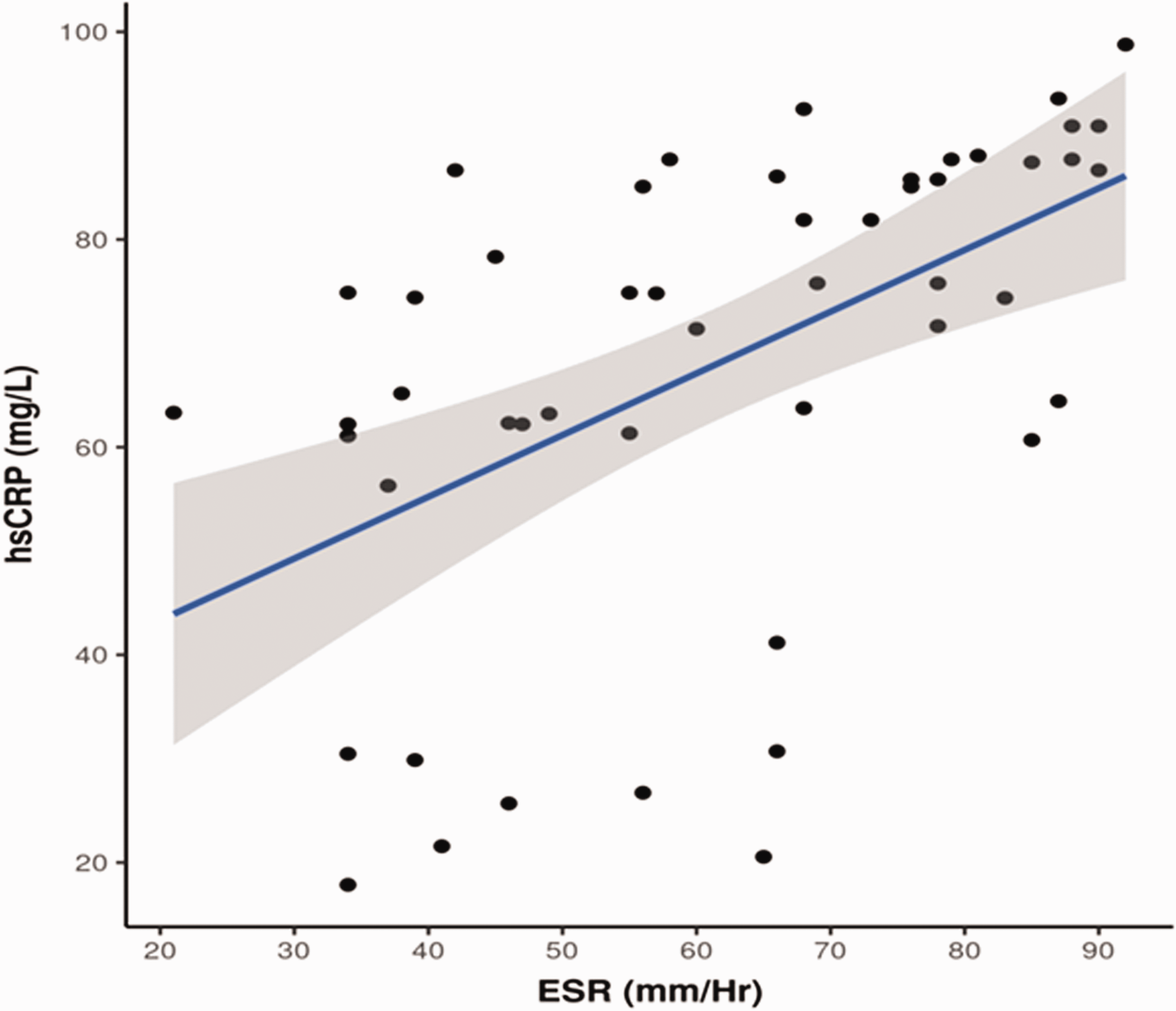
Discussion
The diagnosis and management of tuberculosis in resource poor countries remain challenging. A measure of treatment success is the attainment of sputum conversion. 16 SCR at the end of IP shows the patient’s response to ATT. 4
The difference in serum levels of hsCRP between smear and delayed converters was statistically significant. Similar significant associations were found with radiological findings (especially cavitation, and bilaterallesions) evening rise of temperature, haemoptysis, dyspnoea, advanced disease, fever and weight loss.17–19 These data reveal that the rise in serum CRP levels was related to tubercular parenchymal lung damage. In tuberculosis control, this finding may be relevant because patients with significant parenchymal involvement may have advanced stages of disease with increased risk of poor outcome.
Thus, the baseline serum hsCRP levels may also be of use as an additional surrogate marker for severity of pulmonary tuberculosis in the patient.
Conclusion
The hsCRP, although non-specific, is a valid maker for inflammatory response which can be easily performed even in resource limited settings. Thus, it could be of great use in risk stratification and treatment monitoring as an adjunct tool. This needs to be validated by further studies with a larger sample size and varied TB cohorts.
Footnotes
Authors’ contributions
BK contributed in the concept, design, definition of intellectual content, clinical studies, experimental studies, data acquisition, article preparation, article editing and article review. SKS contributed in the design, definition of intellectual content, literature search, clinical studies, experimental studies, data acquisition, data analysis, statistical analysis and article preparation. RA contributed in design, definition of intellectual content, clinical studies, data acquisition, article editing and article review. PH contributed in design, definition of intellectual content, experimental studies, data acquisition and article review. NPS contributed in design, definition of intellectual content, experimental studies, data acquisition and article review. AK contributed in design, definition of intellectual content, experimental studies, data acquisition and article review.
The manuscript has been read and approved by all the authors, that the requirements for authorship as stated earlier in this document have been met, and that each author believes that the manuscript represents honest work.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.