
Abstract
Cutaneous leishmaniasis is spreading in Ethiopia and outbreaks have been recorded at new foci. In the Ankesha-Guagsa district, from September 24 to 28, 2020, 39 suspected cases were screened, and amastigote stages were identified in lesion samples of 34 (87.2%) cases.
Introduction
Cutaneous leishmaniasis (CL) is a growing health problem in Ethiopia; it continues to spread 1 and is now endemic in 80 districts in the country with 20,000 to 30,000 incidence cases and 29 million people at risk. 2
In Ethiopia, CL is caused by L. aethiopica, transmitted by the bite of sand flies in highland areas. 3 It is a disfiguring protozoan disease, with the potential of long term psychological and social consequences, especially in young women (gender stigma). The disease presents in three clinical forms: localized cutaneous leishmaniasis (LCL), mucocutaneous leishmaniasis (MCL) and diffused cutaneous leishmaniasis (DCL). 4 However, the outcome of infection depends on the differences in species of Leishmania parasites and the host's specific immune response. 5 Hence, species specific diagnosis and treatment is essential as the spectrum of disease and its response to treatment vary according to the species. 6 Some authors suggest, however, that outcome is determined more by patients’ immunogenic background than by the species type involved. 7
Although the disease is non-fatal, attention given to prevention and control has been poor compared to visceral leishmaniasis (VL). 8 Because of this neglect, CL continues to spread to new areas distant from the Siltie district in 2007; 10 thus, the outbreaks in the Dega Damot 9 and now in 2020 the Ankesha- Guagusa districts of the Amhara Region.
Materials and methods
After alert of a suspected outbreak on September 20th, between September 24th to 28th, 2020, 39 suspected cases were screened and referred to the nearby health facility in Ankesha-Guagusa district. On the next day, using standard case definitions, all had skin slit samples smeared on a new frosted microscopic slide and left to dry in the air, and then stained with a 1:10 diluted Giemsa solution for 10 min for microscopic examination. A structured questionnaire was developed to assess the sociodemographic characteristics of suspected cases.
Our investigation protocol was approved by the Institutional Review Board of the Amhara Public Health Institute before clinical and laboratory investigations. Each suspected case was requested to give written prior consent. All positive cases were treated accordingly.
Results
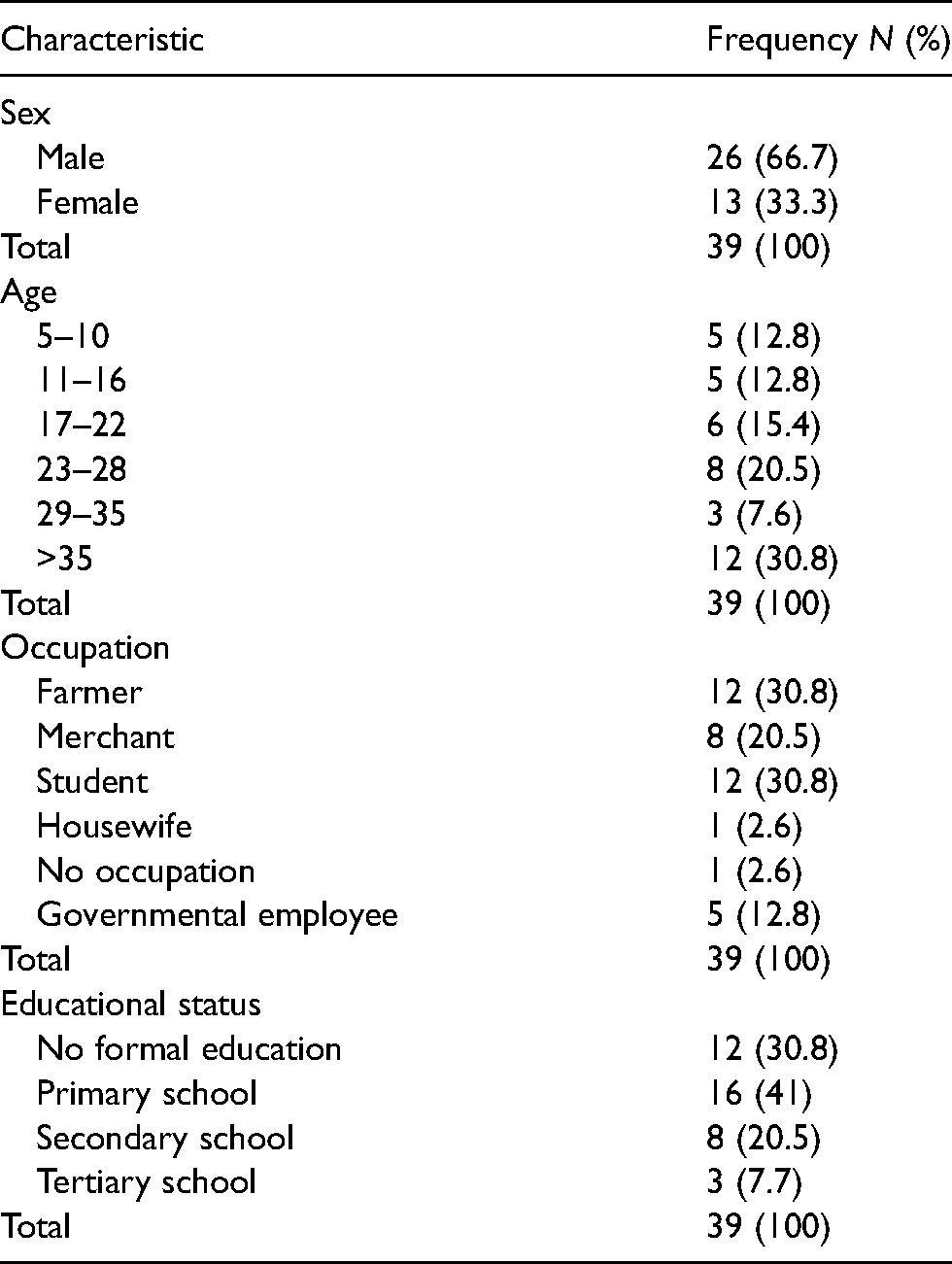
Of the 39 cases, 26 (66.7%) were males. Most (12, 20.8%) were above 35 years of age. Equal numbers were farmers and students (12, 20.8%). Respectively, 16 (41%) had primary school education, and 12 (20.8%) had had no formal education (Table 1).
Sociodemographic characteristics of cutaneous leishmaniasis suspected cases in ankesha -guagusa district from September 24–29/2020.
Parasites were confirmed in 34 (87.2%), of whom the majority (33, 84.6%) were localized. Most of these (17, 43.6%) had a microscopy result of 1+ and (6, 15.4%) had 4+ (Table 2).
Prevalence of cutaneous leishmaniasis from clinically suspected cases in ankesha-guagusa district from September 24–29, 2020.
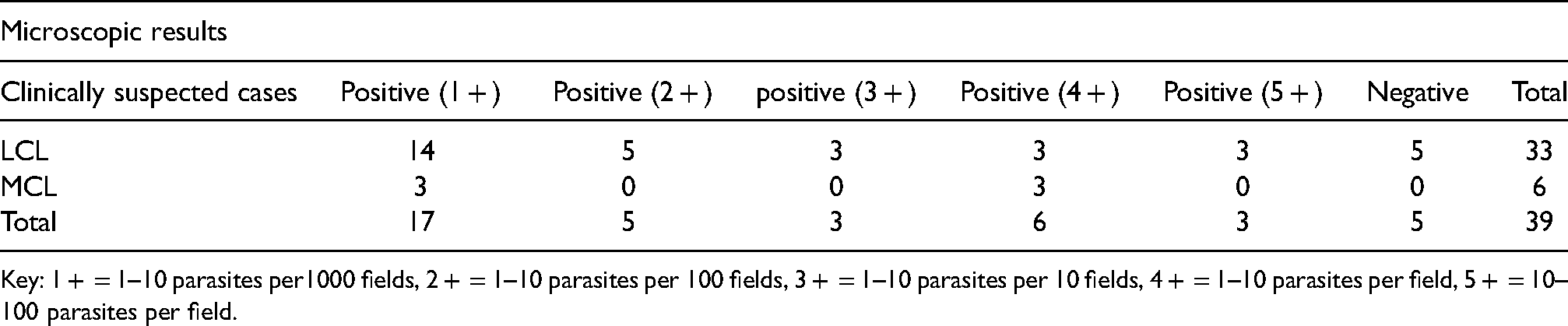
Key: 1 + = 1–10 parasites per1000 fields, 2 + = 1–10 parasites per 100 fields, 3 + = 1–10 parasites per 10 fields, 4 + = 1–10 parasites per field, 5 + = 10–100 parasites per field.
Discussion
In the Amhara Region, there is no active surveillance to find suspected cases and no strategies designed for implementation of vector control CL cases who present to the health facilities are treated and passively surveilled. The first line drug for CL is sodium stibogluconate, but no published reports on the results of any of the three methods, namely, conservative, topical or systemic exist Consequently, no firm recommendation can be made. The rocky hyrax is the reservoir host for CL; rock stone is used in practically in buildings. The equable temperature (between 11o and 25°C) and land scape favor breeding sites.
The limitation of our investigation is that we were unable to perform more advanced laboratory diagnostic tests such as a PCR to identify specific causative agents. Nonetheless we definitely demonstrated a worrying outbreak of CL which has not to date been addressed.
Conclusions
In this investigation, more than 50% of the affected suspected cases were males and majority of the suspected cases were LCL. Therefore, further study will be done to have full information.
Footnotes
Acknowledgements
We would like to acknowledge cutaneous leishmaniasis suspected cases who gave for sample and Ankesha-Gugsa district hospital laboratory staff who gave space for the laboratory work.
Declaration of conflicting interests
The authors in this outbreak investigation declared they have no competing interests.
Funding
Since this is an outbreak investigation, there was no funding for this investigation.