
Abstract
Systemic lupus erythematosus is an autoimmune connective tissue disorder that has well established cutaneous features and typically affects women. However, isolated bilateral periorbital involvement is a rare clinical presentation of systemic lupus erythematosus, which may often delay the diagnosis and treatment. We report such a case in a 20-year-old male.
Case report
A 20-year-old man presented with bilateral periorbital swelling with erythema and crusted lesions on both the eyes for four months. He denied any history of head or ocular trauma, pruritus, fever, fatigue, arthralgia, myalgia, oral symptoms, dyspnoea or visual disturbance. Neither were photosensitivity, use of topical or oral medications, cosmetics, wearing spectacles and contact lenses reported. Systemic examination did not reveal any abnormality: in particular, no lymphadenopathy was palpated. Slit-lamp examination of the eyes showed no significant abnormality (Figure 1). Differential diagnoses considered were contact dermatitis, discoid lupus erythematosus (DLE), dermatomyositis, Sjøgren’s syndrome and lymphoproliferative disorders. Routine laboratory investigations were within normal limits except for an elevated erythrocyte sedimentation rate. Chest radiography was within normal limits. Antinuclear antibodies were positive with a homogenous pattern (1:160 IU/mL; N < 1:80 IU/mL). Further, anti-double strand DNA showed strong positivity. Based on these details, a diagnosis of SLE was made. Treatment with oral hydroxychloroquine (400 mg/day for a month and then 200 mg/day for three months) and oral prednisolone (30 mg/day for a week) was commenced. After one week, there was a partial regression of eyelid oedema and erythema, which disappeared completely within three months (Figure 1). At six months’ follow-up, there were no signs of recurrence or systemic involvement.
(a) Clinical image showing marked oedema and erythema with crusting on both the eyelids; (b) clinical image showing complete regression of oedema with postinflammatory hyperpigmentation.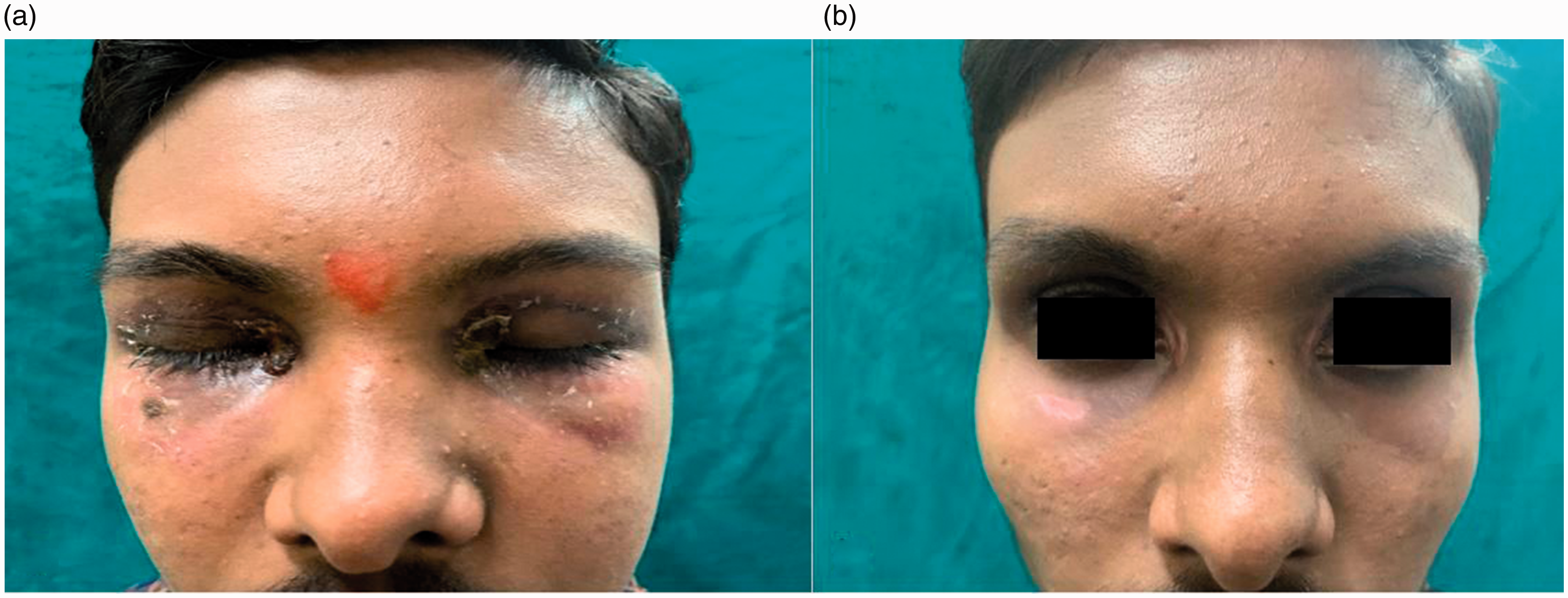
Discussion
Periorbital oedema may be a presenting manifestation or may appear in the course of various diseases. Among connective tissue diseases, it has been found to be the sole manifestation of dermatomyositis and DLE in a few studies. However, its association with SLE as the only cutaneous manifestation is quite uncommon, 1 with an incidence of 1:1000; it is seen in SLE in 48:1000. 2 In one study 3 of 553 patients, 25 patients had periorbital oedema and erythema as cutaneous manifestations of lupus. Of these, six patients were diagnosed as SLE during follow-up, and all of them had unilateral eyelid involvement. 3 Interestingly, our patient was male with the involvement of both periorbital zones, which is a rarely reported finding.
The three common subtypes of cutaneous lupus erythematosus (CLE) include SLE, subacute cutaneous lupus and DLE. Although the manifestations of CLE are well established, a subset of patients may present with atypical cutaneous manifestations. 4 CLE involving the eyelid has been occasionally encountered by ophthalmologists and is well known to present as erythematous scaly plaques, with an atrophic surface and associated madarosis. Most of these patients showed unilateral eyelid involvement, and common misdiagnoses were eczema or contact dermatitis, with low autoantibody positivity and high incidence of anti-SSA and SSB positivity. 3
SLE is characterised by the production of a variety of auto-antibodies owing to the presence of autoreactive B and T cells. 5 The anti-dsDNA is considered a specific marker for SLE and observed in 70–98% of patients. 6 Our case was diagnosed as SLE based on the ANA pattern and the presence of anti-double strand DNA. However, the patient did not meet the Systemic Lupus International Collaborating Clinics criteria. Histopathology by biopsy of the skin lesion was refused because of a fear of unaesthetic scarring.
Strict photoprotection, cessation of smoking and vitamin D supplementation are recommended in patients of SLE. Topical calcineurin inhibitor is preferred over topical steroids. Hydroxychloroquine is the drug of choice for the cases of LE with periorbital oedema.
We thus wish to alert fellow clinicians that periorbital oedema may be the only presenting manifestation of SLE.
Supplemental Material
sj-pdf-1-tdo-10.1177_0049475521993244 - Supplemental material for Bilateral periorbital oedema revealed as systemic lupus erythematosus in a young male
Supplemental material, sj-pdf-1-tdo-10.1177_0049475521993244 for Bilateral periorbital oedema revealed as systemic lupus erythematosus in a young male by Sudha V Damarla and Brahmaiah Upputuri in Tropical Doctor
Footnotes
Ethical approval and informed consent
Written informed consent have been obtained from the patient for the publication of the information and images
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.