
Abstract
Intraoperative choledochoscopy is on the rise. Simulated training is essential for proper handling of the instrument during laparoscopic bile duct exploration. The article describes a low budget innovative choledochoscope for simulated training in low resource setting.
Introduction
Intra-operative choledochoscopy is a well-established procedure for removal of bile duct stones. 1 But it is plagued with several limitations including operator dependency, prohibitive cost and technical issues. 2 Factors related to operator dependency include a) inadequate endoscopic training, b) the steep learning curve and c) lack of simulated training models 2 , which currently exist of 3-dimensional printed (3DP) and ex-vivo models of the complex hepatobiliary system. All of these, however, primarily include the need for an original choledochoscope3,4, whose cost (US$ 3000) with the cost of the 3DP (1000 US) together makes this unafforable.5 Taking these issues into consideration and also the undisputed need of choledochoscopy simulated training, we devised a low budget choledochoscope simulating the original choledochoscope for training of residents. We describe such a training model.
Model
The innovative choledochoscope is made from a Ch20 polyvinyl chloride (PVC) drainage tube from an abdominal drainage kit, a Ch5 infant feeding tube and a 6-LED 5mm borescope camera available commercially (Figure 1). The tip of the infant feeding tube is cut to act as instrument channel. The 5mm borescope camera along with the infant feeding tube is inserted within the drainage tube after distending the tube with a hot blower. The infant feeding tube and camera are sealed within the inner side of the drainage tube using polyvinyl solvent cement. The tube is then covered with black insulation cover of a laparoscopic hand instrument to impart an original look.
The complete assembly is connected to a laptop to act as the simulated choledochoscope for training. This whole assembly costs only US$40.
A standard laparoscopic endo-trainer mounted with a Ch32 Romo abdominal drain with a side hole (the ‘choledochotomy’ site), cut into a 7 cm length serves as the common bile duct. Both ends are plugged with cotton after insertion of crushed peanuts serving as biliary calculi.
The innovative choledochoscope is inserted through the side hole of the simulated bile duct and the fragmented peanut is localized. Thereafter a 4-wire 5mm Dormia basket, inserted through the infant feeding tube, is used to capture the peanut and extract it through the side hole (Figure 2).
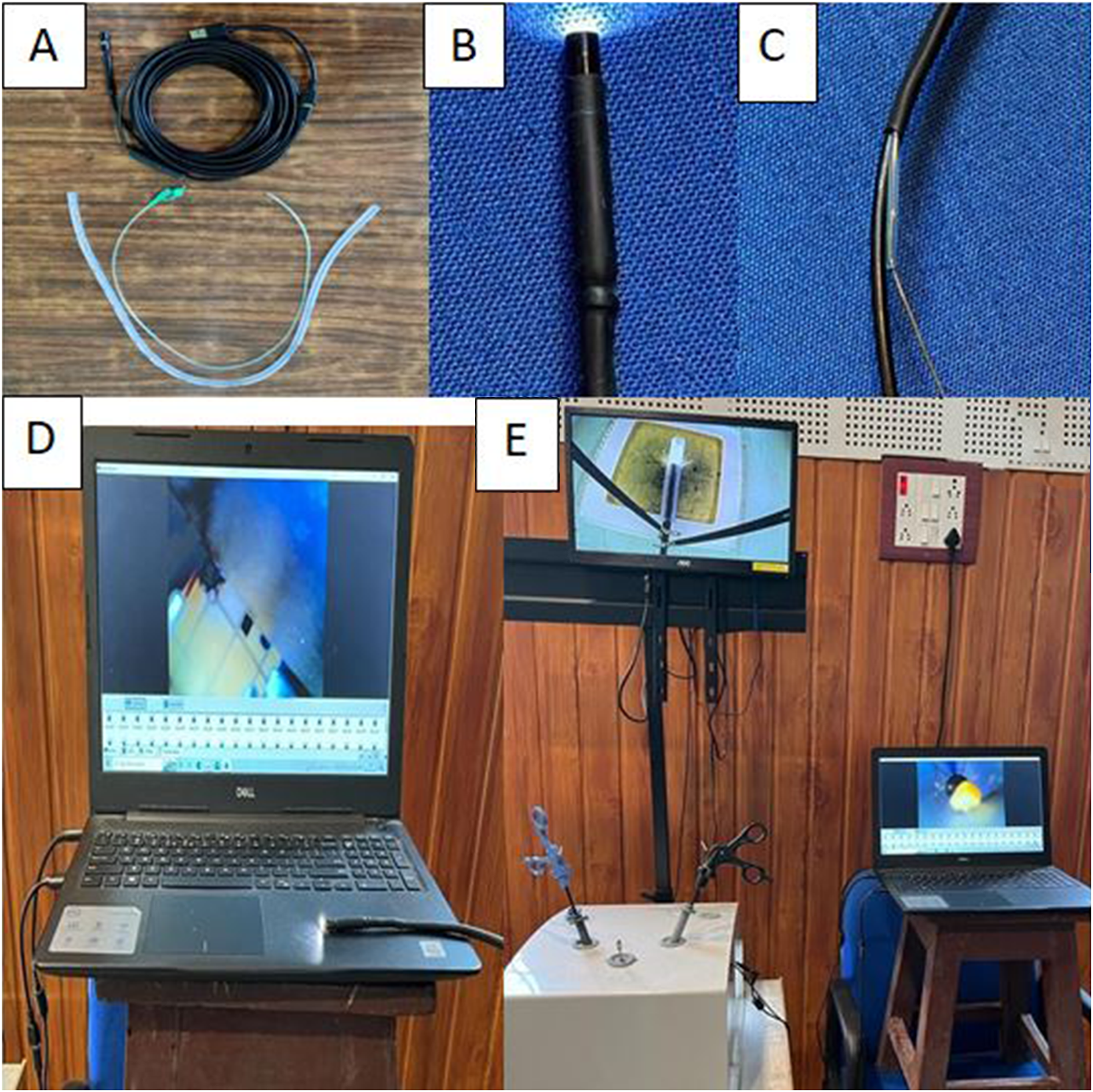
Innovative choledochoscope A. Borescope, 20 F abdominal drain, 5F infant feeding tube. B. Tip C. End with working channel D. innovative Choledochoscope attached to Laptop C. The training assembly.
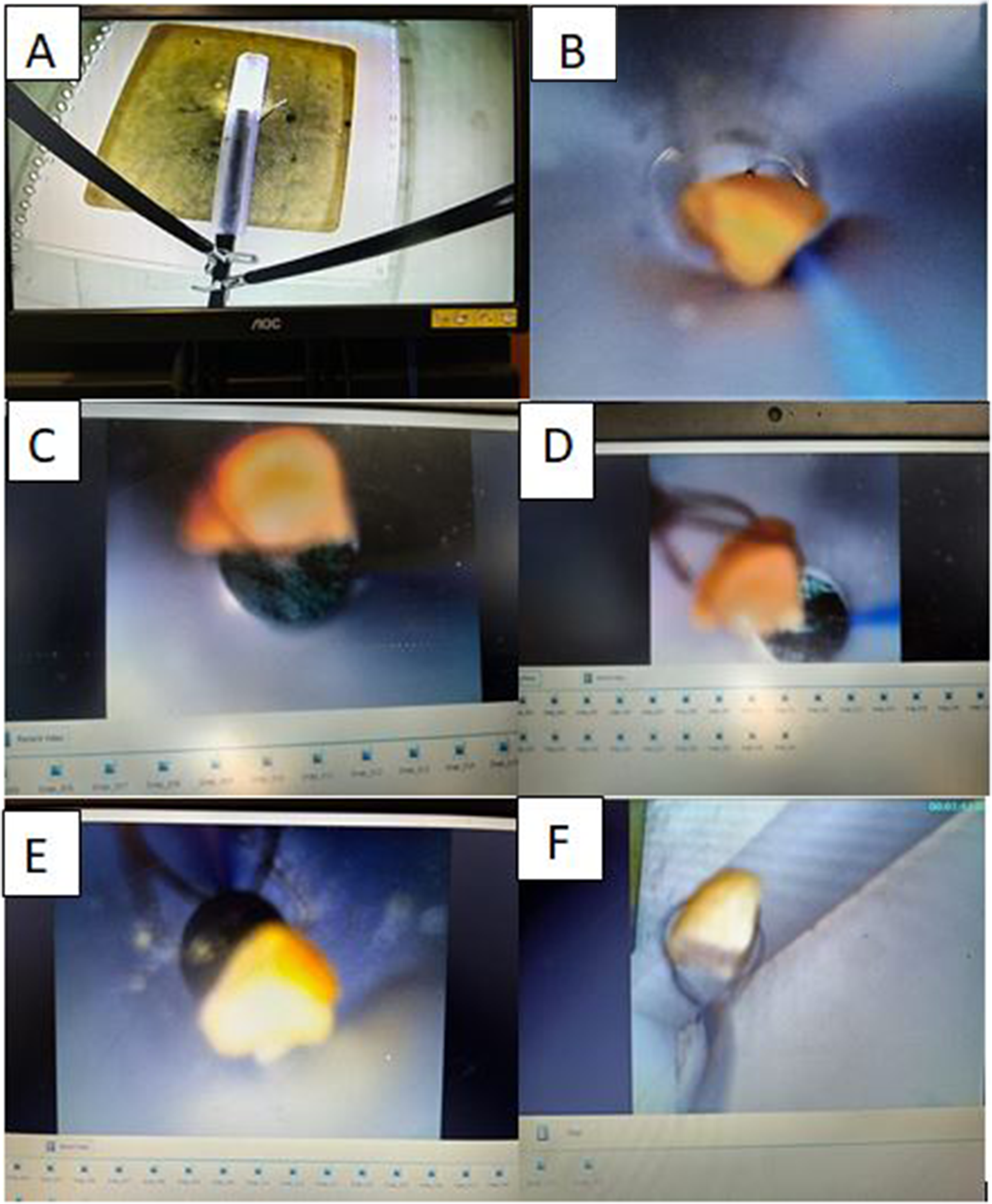
A. Innovative choledochoscope inserted into similated bile duct mounted in an endotrainer. B & C. localization of simulated bile duct stone. D & E. caging the simulated stone with Dormia basket F. Extracted simulated stone with dormia basket.
Conclusion
Our simulation based learning module developed for trainees appears to show superior instructive benefit to physical three-dimensional printed models or freehand double-bending direct per-oral cholangioscopy technique. 3 A further validation (knowledge, attitude and practice, (KAP) study) is in progress.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article