
Abstract
Introduction
The incidence of incisional hernia (IH) after laparotomy varies from 5% to 17%; depending upon the time lapsed and the type of initial surgery.1,2 Giant incisional hernias (IH larger than 10 cm, GIHs) are a special entity and are commonly repaired with a non-absorbable mesh placed in the retromuscular plane, with the hernia sac (HS) as a barrier between the mesh and abdominal contents. 3 A common problem in long-standing GIHs is a combination of wide separation of recti, inability to close the anterior rectus sheath primarily, and a thin, poorly vascularised, stretched overlying skin. In such a scenario, it is a challenge to provide an anterior cover to the mesh which prevents the mesh from directly coming in contact with skin, minimising the risks of mesh infection, exposure and explantation. 4 For this, a sandwich mesh repair has been employed, by placing the non-absorbable mesh between two layers of peritoneum derived from the overstretched HS. 5 We open the sac at the lateral border, instead of in the middle, to avoid the probability of dense adhesions to the central part of the scar, especially in a recurrent GIH. This also allows us to utilise the whole length and width of the sac for it to ‘sandwiching the mesh’. We present the results of our simple modification called ‘Flip-HS sandwich mesh hernioplasty.
Patient and methods
Our prospective interventional study was conducted in the Department of Surgery of a Tertiary Teaching Hospital in Central India from 1 December 2016 to 30 June 2021. The study was cleared by the institutional ethical committee and informed consent was obtained from all individual patients. A detailed preoperative history, along with body mass index (BMI), and routine biochemical and haematological parameters were noted. Associated co-morbidity such as diabetes, obesity (BMI > 25) or smoking were also noted. Abdominal computed tomography of all the patients was done to assess the size of the defect. Patients who met the following criteria were included in the study: adult patient (>18 years of age) and GIH (index or recurrent, > 10 cm defect). Patients were taken for surgery under antibiotic cover with Piperacillin + Tazobactam and Metronidazole.
Operative technique
A skin incision was made at the summit of the defect, and the HS was dissected till the base of the defect. A finger breadth opening was made on the lateral border of the sac, and a finger passed into the peritoneal cavity to assess adhesions of the sac with intraperitoneal contents. By extending this incision over a finger, the HS was opened eccentrically at one border of the defect, performing any required adhesiolysis under vision. This creates two unequal HS flaps: one larger with the cut edge A and one smaller with the cut edge B (Figures 1 and 2).
The medial edge of the rectus sheath was identified on both sides, and incised (points C and D) to reach and develop the retrorectus plane (E1 and E2) for a sufficient extent to place a mesh of the requisite size (Figure 2).
The cut edge of the smaller flap (B) was fixed by interrupted sutures. using polypropylene 1/0 at 2cm intervals, to the under surface of the larger flap (point F). Thus, peritoneal closure of the defect was achieved, which prevents the viscera from coming in contact with the mesh (Figures 3 and 4).
An appropriately sized polypropylene macro-porous mesh (>75µ), of sufficient size to extend at least 5 cm beyond the defect all around, was placed in the retrorectus plane (E1) on the side bearing the larger flap of the HS (Figure 3).
Multiple slits were made in the larger hernial flap, near its fixed margin, beyond the point F (Figure 4). The length of these slits varied from 1 to 2 cm to even 3 to 4 cm. This depended upon available space to make a slit of maximum length, while minimising damage to vasculature of the flap (seen by transillumination). So, depending upon the vascular pattern of the flap, the size of the slits may vary in the same patient.
After the mesh emerged from the retrorectus space (E1), and close to the larger flap, the mesh was cut into strips corresponding to the number and size of slits made in the flap. These were passed through the incisions in the flap (point G, Figure 5) to pass to the opposite side of the hernial defect. These strips of polypropylene mesh were sutured to each other by polypropylene 2/0 suture to reconstitute a single sheet (Figures 6 and 7), which was spread over the defect and passed into the retrorectus plane of the opposite side (E2) (Figure 3).
Now, the under surface of the large HS flap was sutured to the incised margin (point C) of the opposite anterior rectus sheath with polypropylene 2/0 suture (Figure 8). The remaining part of the flap was then ‘flipped’ back, and its cut edge (point A) was sutured to the incised margin of the anterior rectus sheath of its original side (point D, Figure 8). This flipped part of the larger flap prevents the mesh from coming in contact with the skin. Thus, the HS was fashioned to sandwich the mesh (Figure 8).
Suction drains were placed in the retrorectus plane deep to mesh and in the subcutaneous plane. Finally, the redundant, thinned out skin was excised, and its incision was closed with interrupted 3/0 nylon sutures.
Patients were allowed oral feeds as guided by bowel activity. Parenteral antibiotics were continued for 5 days, and then oral cefuroxime was administered till sutures were removed, usually on the 14th post-operative day. Antibiotics were changed as needed, based on culture and sensitivity tests and clinical response. Drains were removed when the output was <20 ml serous fluid/day.
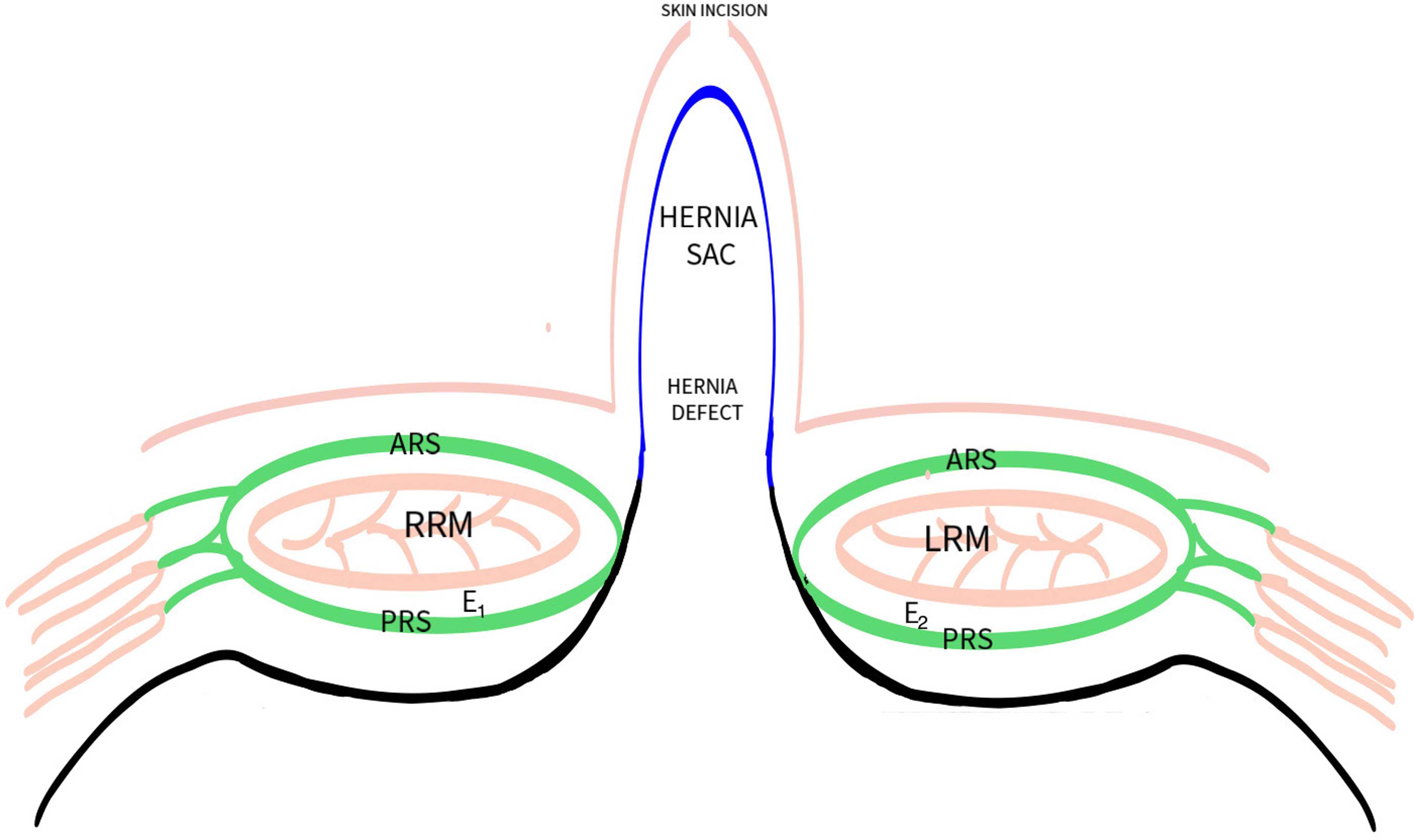
Schematic diagram showing anatomy of giant incisional hernia (GIH) (cross section).
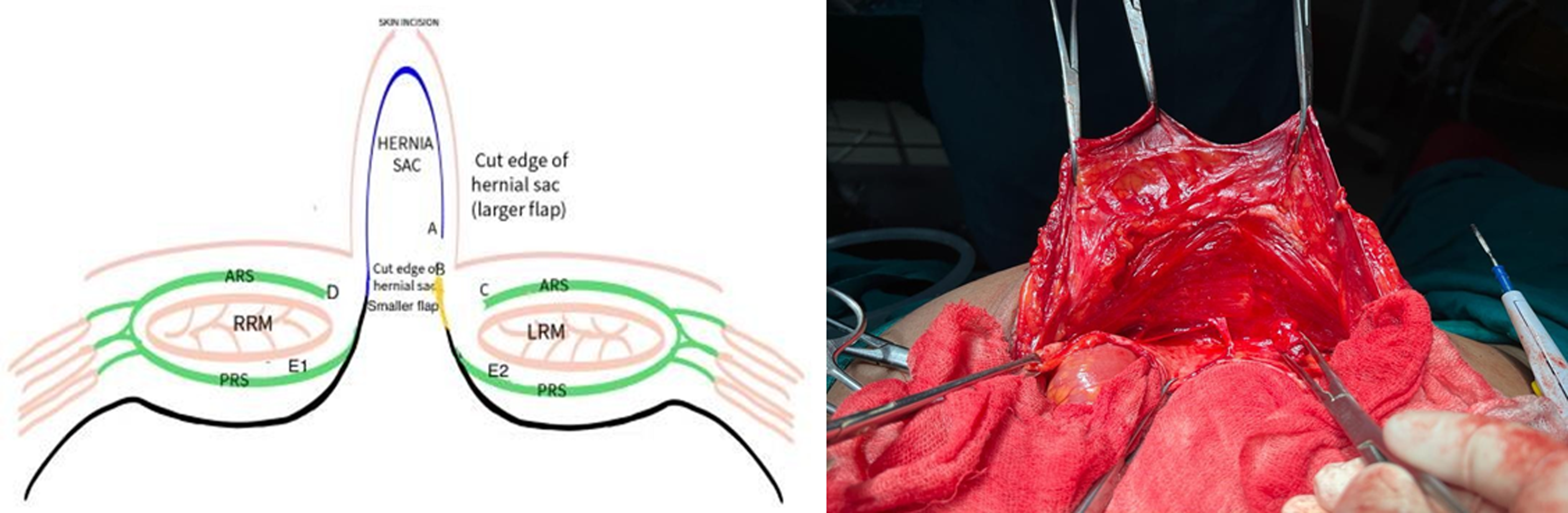
Schematic diagram showing eccentrically cut hernia sac (HS) with development of retromuscular plane.
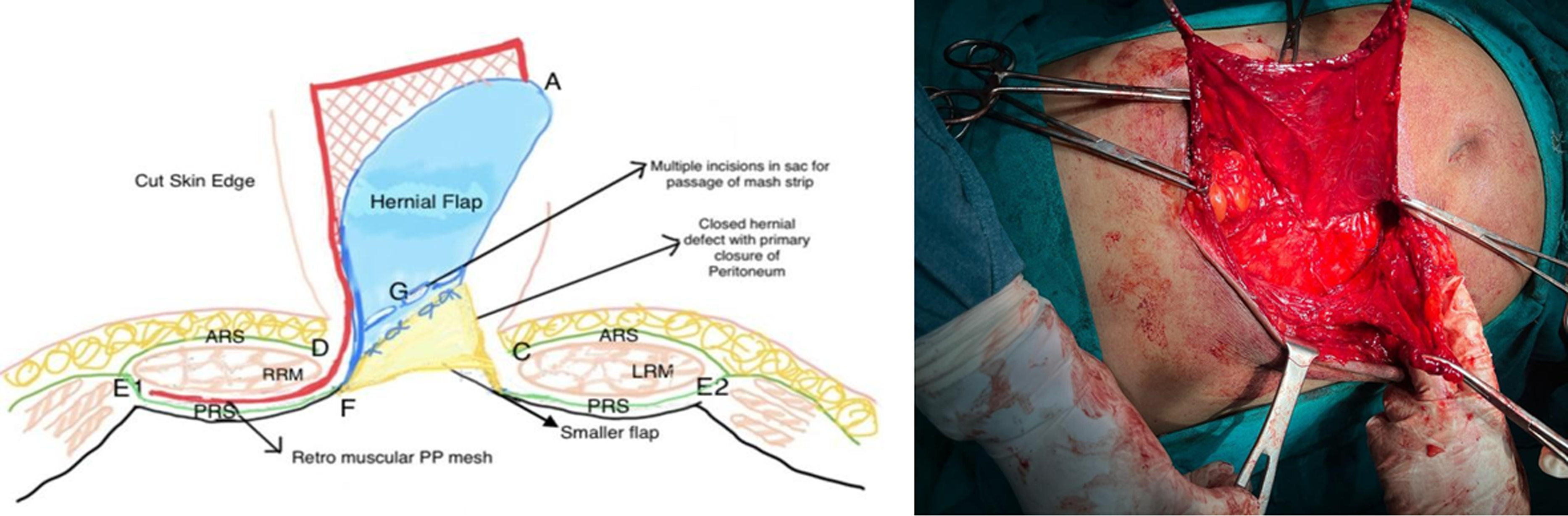
Diagram showing primary fascial closure of hernial defect F and placement of PP mesh in sublay plane E1. F suturing of cut edge of smaller hernia sac (HS) B with under surface of larger HS flap (primary closure of hernia defect).
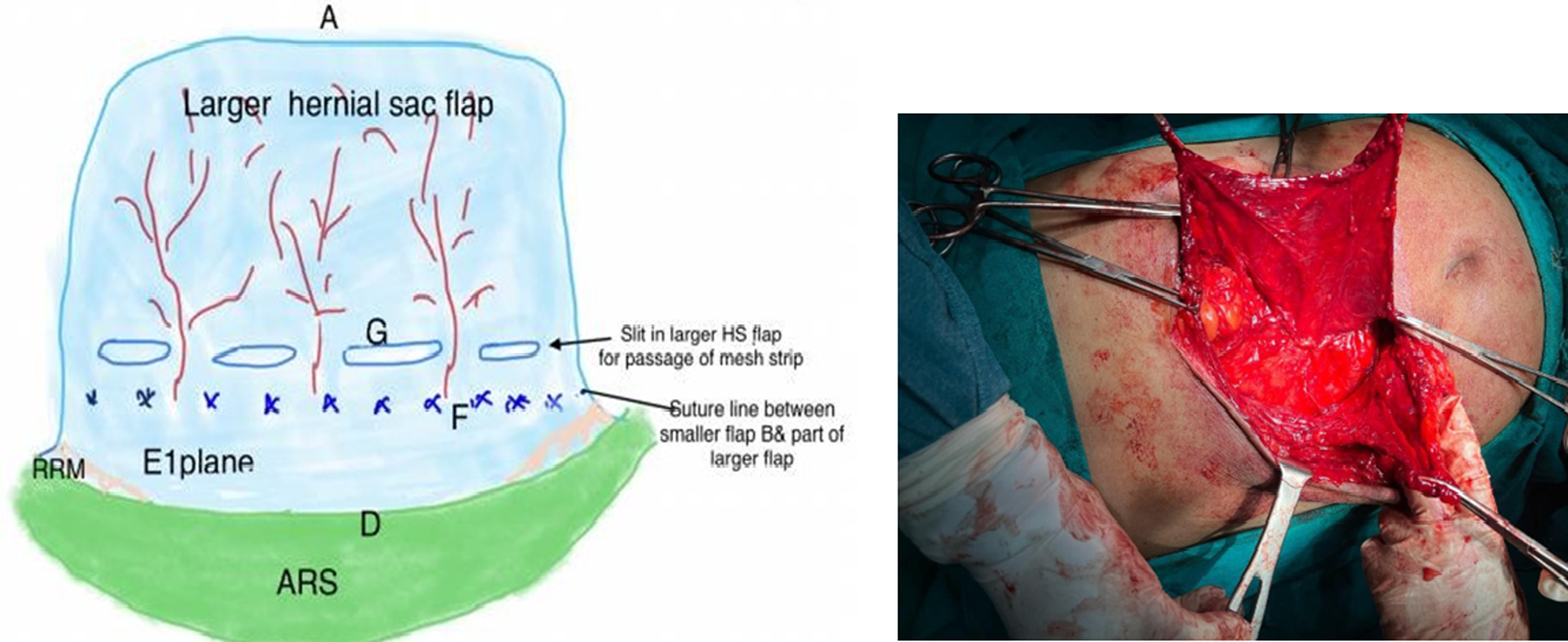
Diagram showing multiple slits G in the larger hernia sac (HS) flap (longitudinal view).
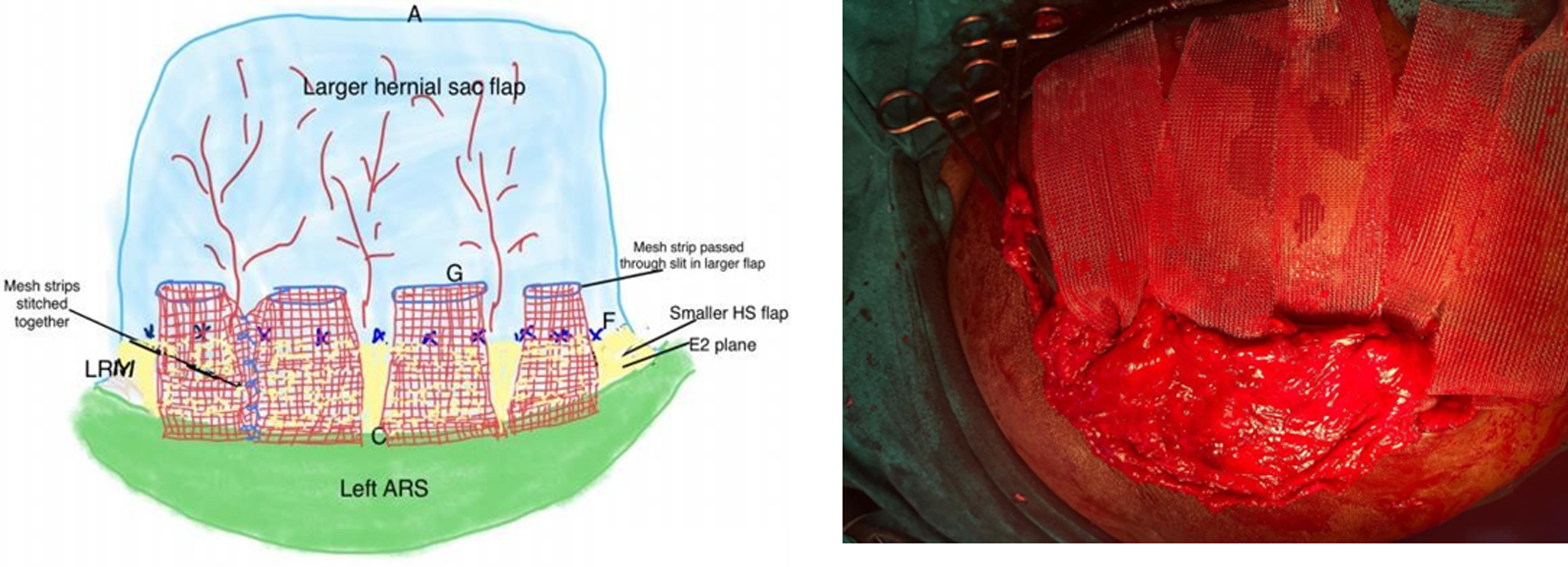
Diagram showing cut (multiple) mesh strips crossing over through the incisions G in larger hernia flap.
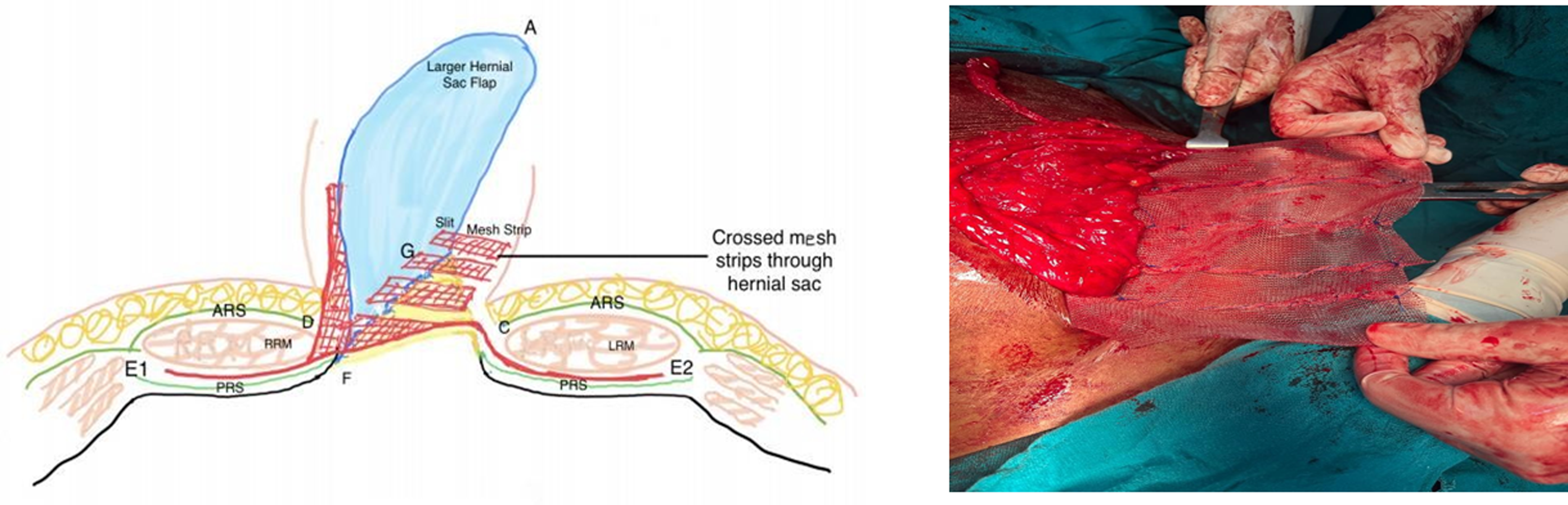
Cut (multiple) mesh strips crossing over through the incisions in larger hernia flap and reconstitution of PP mesh.
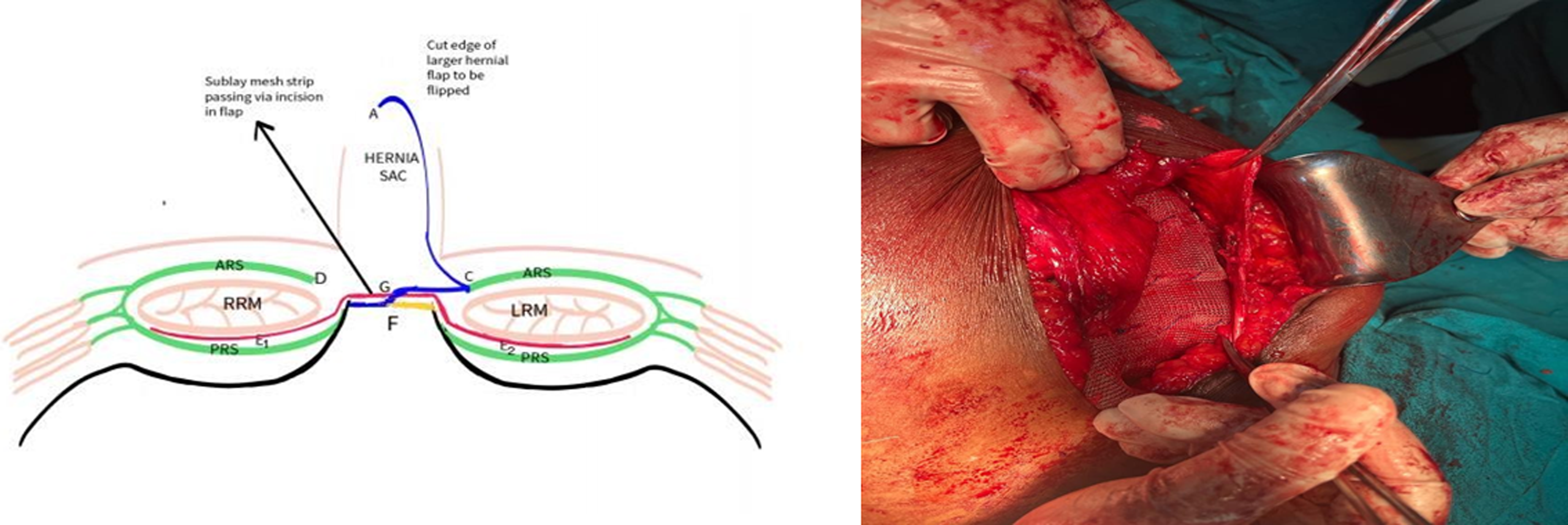
Schematic diagram showing placement of sublay PP mesh (red coloured) and flipping of larger hernia sac (HS) (blue coloured) (cross section).
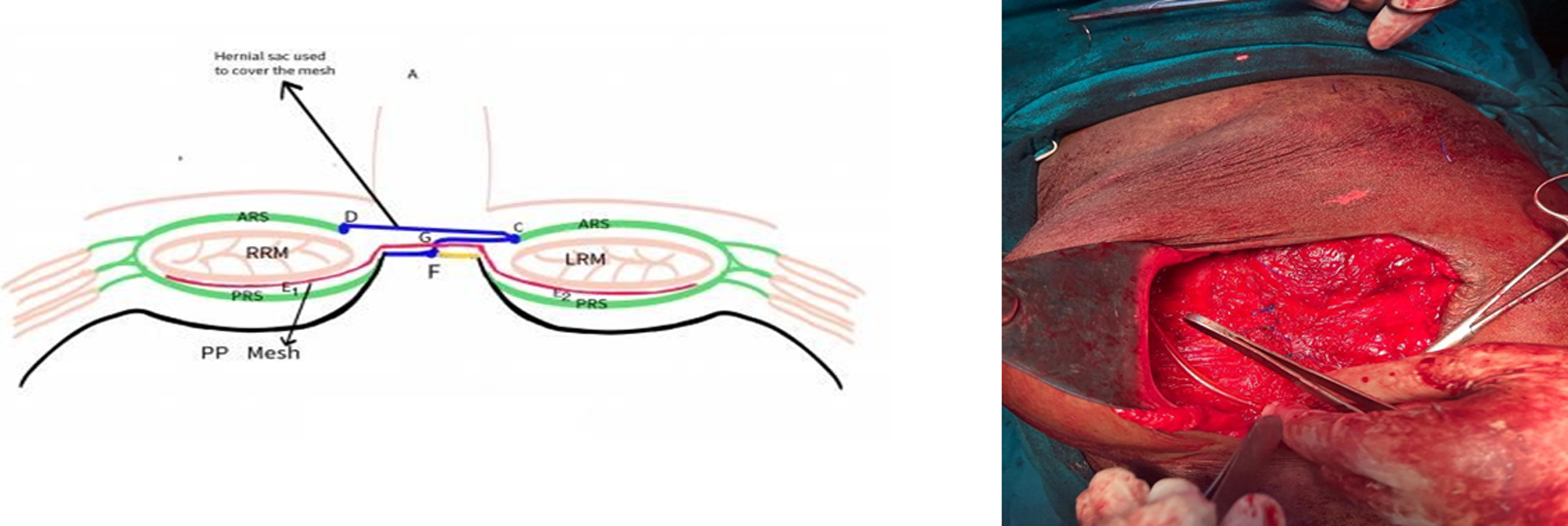
Schematic diagram showing covering of mesh on both the sides (sandwich) by flip-flap hernia sac (HS) (cross section).
Immediate outcomes measured were surgical site occurrence (SSO), that is, surgical site infection (SSI), haematoma, wound dehiscence, mesh exposure, seroma formation; and late outcomes recurrence of IH and the need for mesh explantation. Follow-up for any recurrence was done by clinical examination and abdominal ultrasonography at 1, 3, 6 and 12 months; and afterwards according to patient convenience.
Result
During the study period, 21 GIHs (9 men and 12 women) were operated by this technique. The age ranged from 27 to 65 years (mean 44.2 years) (Table 1). The average size of the hernia defect was 243.09 cm2 (110 cm2–306 cm2) and the average width was 14.09 cm (10cm–18cm). The overlying skin was thinned out in all patients while 4/ 21 had skin ulcerations. The commonest index surgery (15/21) was emergency laparotomy. Obesity (18/21) and diabetes (17/21) were the commonest comorbidities. 4/21 were recurrent IHs (Table 1).
Demographics of patients and outcomes.
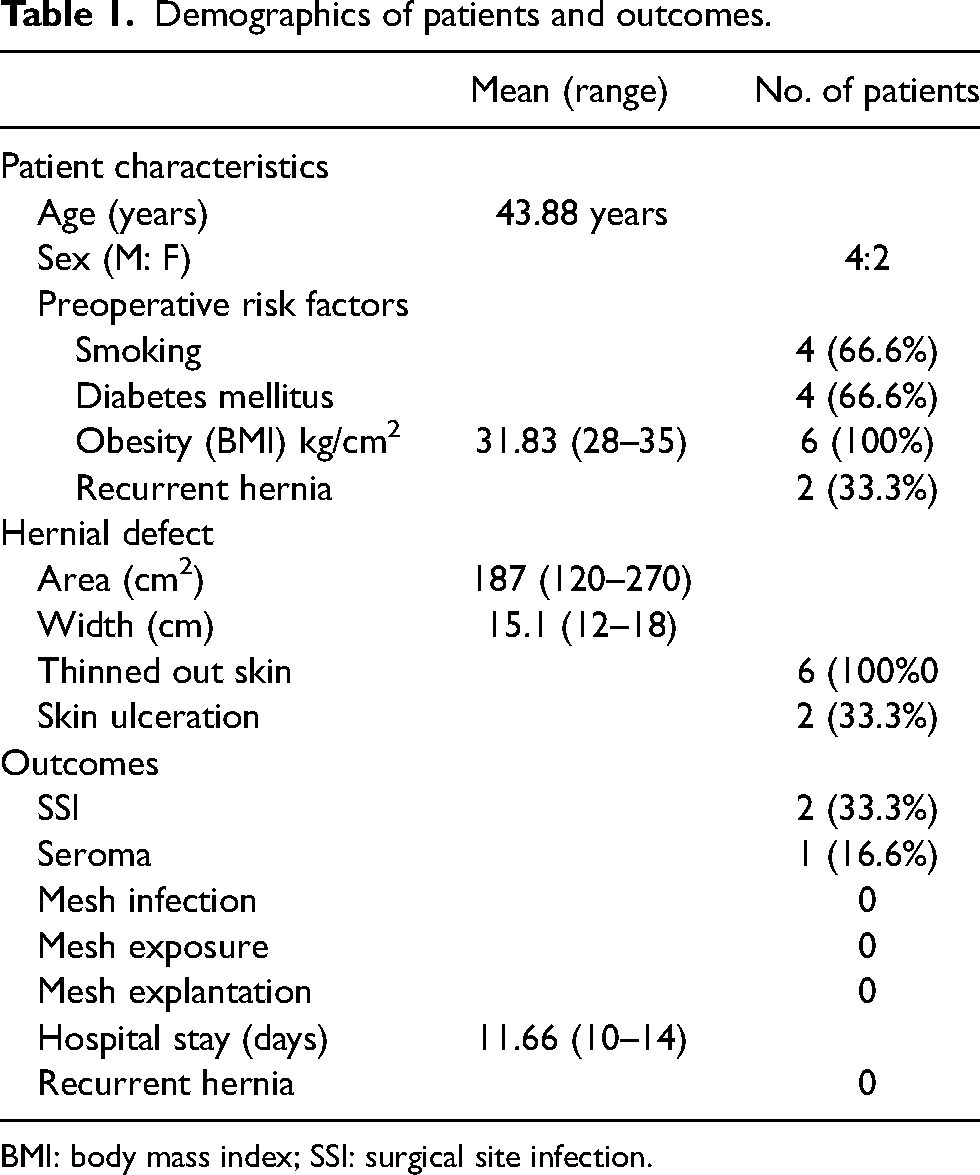
BMI: body mass index; SSI: surgical site infection.
Adhesions of the HS with intraperitoneal contents and previous scar tissues were found in all the cases and required meticulous dissections. There were no iatrogenic bowel injuries. The mean operative time was 102 min (range: 90–120 min).
SSI was common (8/21, 38%, Table 1) but all patients could be managed by opening a few sutures, draining the collection, irrigation with povidone-iodine solution and applying Mupirocin dressings. Only one of the seven patients with a seroma required aspiration. Secondary suturing was required in one of the eight patients with SSI, which was done on the 16th post-operative day before discharge from the hospital.
Wound dehiscence, mesh infection or mesh exposure were not seen in any patient. Mesh removal was not required during the entire study period. There were no readmissions or reoperations or recurrences of the hernia. There was no mortality. One patient, a known case of chronic obstructive pulmonary disease, needed post-operative ventilatory support and was discharged from the hospital after 16 days. The mean hospital stay was 7.7 days (6–16 days) and the mean follow-up was 22.3 months (7–48 months).
Discussion
The optimum treatment of GIH is challenging. Our technique of ‘Flip-flap’ HS sandwich mesh hernioplasty provides a simple effective alternative to conventional HS sandwich mesh hernioplasty in selected cases. Conventionally, the HS is cut open in the middle with two equal flaps, one placed below and the other above the mesh to complete the sandwich mesh hernioplasty.5–8 However, we make a small opening at the lateral border of the sac to look for adhesions and then decide which border of the HS would be safe to incise. This allows us to separate safely all adhesions with omentum, bowel loops, skin and subcutaneous scar tissue. Another advantage is ‘full’ utilisation of every bit of this HS flap – when two equal halves are made; the lower/ inner flap may be found larger than the defect leading to part of it being sacrificed and the upper or outer defect found smaller and inadequate to cover the mesh fully. Our technique allows the largest possible single sheet of HS, to utilise every inch of HS obtained and the mesh (in the form of strips) can be crossed over through the flap in any direction: horizontal, vertical or oblique – and can be tailored according to need. This resonates with the contemporary tailored approach to hernia surgery and is highlighted in contemporaneous hernia guidelines. 9 This technique is preferred for GIHs with previous surgical scars, and with thinned out, ischaemic, ulcerated overlying skin; where the risk of perforating the flap at multiple sites during dissection is high.
In the originally described sandwich technique, Matapurkar et al. did not extend the mesh beyond the defect; hence they did not require any manipulation to bring the upper or outer HS flap anterior to the mesh. 5 Subsequent publications inserted the mesh in the retrorectus space beyond the defect, hence they incised the base of upper or outer HS flap to allow the lateral part of the mesh to be placed posterior to it, thus theoretically compromising the blood supply of the upper or outer HS flap.6–8 We made incisions in this outer HS flap near its fixed margin; these were used to pass strips of mesh to the opposite side of defect. We are aware of the theoretically limited vascularity of this single HS flap when compared to that of two equal flaps. Hence, we avoided suturing it continuously with the edge of defect, and protected its blood vessels using transillumination when making incisions for passage of the mesh strips. In our technique, the mesh lies beneath the skin, separated from it only by a layer of the HS. For the cases requiring secondary suturing due to wound dehiscence and SSI, none had a visible exposed mesh but was covered by hernia sac. This implies that the single HS flap, with its slits; was surviving, and functioning as an effective barrier.
Sandwich technique of using autologous HS allows placing the mesh in a sublay retrorectus position with optimal mesh overlapping: enveloped in a fascial cover separated deep from intra-peritoneal content and superficially from the subcutaneous tissue. Additionally, it is noted that when peritoneal collagen fibre regenerates, it results in a thick tissue which is similar to aponeurosis. In a sandwich mesh repair, this aponeurosis buttresses the mesh and provides strength to the repair.10,11 Such deeper and superficial cover of the mesh with suture lines in different planes and lines prevents complications such as mesh migration, bowel adhesions, erosions, fistula formation, chronic wound sinus formation and mesh infection.
The SSI rate of 38% might appear high but many of our patients had significant comorbidity such as obesity, diabetes, smoking and repeat surgery in presence of thinned out ulcerated overlying skin. SSO are known to be a common complication in such a scenario. 12 All our cases responded to opening of skin sutures and ordinary dressings. Such a favourable resistance of the macroporous polypropylene mesh, with pore diameter >70 µ, is well known, as it allows contact of bacteria (measuring one micron in diameter) with granulocytes and macrophages (diameter of 15–20 microns). 13 This also explains the successful use of polypropylene mesh for contaminated and dirty strangulated hernias. 14 The sublay retrorectus mesh placement also helps in protecting the mesh.15,16
Several new techniques have been devised for optimal closure of large hernial defects, which is a testimony to the fact that there is no simple, easy method for managing such defects. These include minimal invasive techniques, totally extraperitoneal repairs, hybrid techniques and novel myofascial release techniques. 17 However, these require special training or equipment, and may use a special mesh, which increases the cost and complexity of such surgery manifold. Our ‘flip-flap’ technique is easy to teach, and uses routinely available instruments and meshes, which makes it an appealing and cost-effective alternative.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.