
Abstract
Our retrospective cohort study of the effects of radiotherapy delay on the oncological outcome of breast cancer patients showed a prolonged radiotherapy waiting interval was associated with a statistically significant increase in the 3-year breast cancer-specific mortality. This research should stimulate setting up protocols geared towards minimizing delays.
Introduction
Breast cancer, despite being among the most researched malignancy in the world, each passing day brings additional questions. Breast cancer is the most common malignancy of women, and specifically is the most common cause of cancer death in women of Trinidad and Tobago, being evaluated as 46.6 per 100,000, among the highest in the world. 1 A disease classically found in older women has become increasingly prevalent in younger groups. 2
An essential step after conservative surgical management is most commonly adjunctive radiotherapy. Its benefit is supported by the Early Breast Cancer Trialist Collaborative Group (EBCTCG), which noted an absolute reduction of local recurrence by 19% when compared with none (7% vs. 26%), and an absolute reduction in mortality of 5%. 3
Despite the absence of any international standard optimal maximal delay period, there is evidence that prolonged delays may have deleterious effects on recurrence rates and survival. This is crucial where a shift toward minimalistic oncologic resection is the norm. 4
Materials and methods
Ours was a retrospective cohort study of patients operated consecutively for histologically confirmed breast cancer, using either conservative or ablative techniques, examined between 2010 and 2017 in our tertiary level institution. A total of 108 patients who had had surgery for breast cancer were retrieved from operative logbooks at the Eric Williams Medical Sciences Complex main operating theatre. Waiting periods for radiotherapy were stratified. Data were sorted into two groups of patients; those who required chemotherapy postoperatively and those who did not. Postoperative adjuvant chemotherapy regimes for primary breast cancer typically have a duration of 4–6 months; those who received neoadjuvant chemotherapy were considered as a separate subset. Groups were stratified for postoperative radiotherapy initiation within 5, between 6 and 9 and over 10 months. We added a maximal observation time for the last group at 3 years, as evidence suggests the majority of recurrence occurs in the first 2–3 years postoperatively. 3
Local recurrence was defined as clinically detected lesions within the ipsilateral breast, at the site of incision or chest wall on clinical examination or by radiological means, at least 6 months after curative surgery. Metastatic disease was defined as confirmed radiographic evidence of dissemination on chest radiography, bone scintigraphy, CT imaging and/or positron emission tomography.
Inclusion criteria were females aged between 18 and 75 years after oncologic resection of confirmed breast cancer with histologically proven clear margins. The objective in these patients was the intention to cure with adjuvant therapy.
Exclusion criteria included those patients where the procedure was done other than for cure, such as wound control, refusal or incompletion of radiation therapy.
Our study was granted ethical approval by the University of the West Indies (UWI) ethical committee for CREC-SA.0075/11/2019 on the 22nd November 2019. The North Central Regional Health Authority (NCRHA) subsequently granted ethical approval for the use of its medical records on the 8th January 2020.
Currently, it is estimated that approximately 40% to 50% of primary breast cancer patients will go on to have adjuvant radiotherapy. We used the Raosoft® sample size calculator to determine the sample size. This calculator demonstrated that our desired number of patients achieving adjuvant radiation should be at least 55 to be able to achieve an adequate power value that would reduce the risk of a type 2 statistical error.
We evaluated the records to acquire independent variables such as demographics, concomitant comorbidity, procedure type, pathology type, and delay between operation and adjuvant therapy (chemotherapy or radiotherapy). Dependent variables included local and distant recurrence, and disease-specific and all-cause mortality. Data were entered onto a questionnaire without any direct identifiers and filled out in a secure room at the medical records department where no public access is allowed.
Collected data were analyzed using the Statistical Package for the Social Sciences (SPSS version 25.0) software. Descriptive data were presented using frequencies and percentages for categorical data and means with standard deviations for continuous variables. Comparisons were done using Fisher's Exact and χ2 tests for categorical data. Binary logistic regression was used for exploring predictors of key dichotomous outcomes. Kaplan–Meier survival analyses were used for censored outcomes and the log-rank test was used for comparisons. Cox-Regression analyses were used to estimate hazard ratios for time-dependent outcomes, with adjustment for potential confounders. Odds and hazard ratios were reported with 95% confidence intervals and a P-value of <0.05 were used to indicate statistical significance.
Results
One-hundred and eight patients were included. Only 85 clinical files were available; a further 15 were excluded for failing to complete their adjuvant regime, for having a positive resection margin and for being outside the specified age range.
Median age was 57 years (range 29–73). Ethnicity included East Indian 34 (48.6%), African 24 (34.3%), Chinese 2 (2.9%) and others 10 (14.3%). Comorbidity is shown in Table 1:
Distribution of comorbidities among the cohort sample.

It is important to note that stage was not ideal as a parameter, as according to the AJCC/TNM staging 8th ed, IHC receptor status is incorporated into the overall staging and this could not be done for all patients in our institution. The immunohistochemical evaluation of specimens was very limited as our laboratory was not consistent in providing details with every case.
Local recurrence was defined as ipsilateral at the site of incision in addition to recurrent lymphatic disease after definitive surgical and adjuvant treatment; this occurred in 11 (15.7%) of patients. Distant metastases related to the finding of hematogenous dissemination at sites such as bone, liver and lungs, was noted in 14 (20%). All-cause mortality (i.e., death within the follow-up period regardless of cause) was seen in 21 (30%) and the breast cancer-specific mortality was 13 (18.6%).
Table 2 shows the association between key breast cancer clinical factors and locoregional recurrence. There were statistically significant associations between locoregional recurrence and grade, tumor stage and lymph node status. There was no significant correlation between average waiting times for those who received radiotherapy in those with recurrence over against those without (9.0 vs. 6.9 months, P = 0.086).
Outline of patient and tumor characteristics.
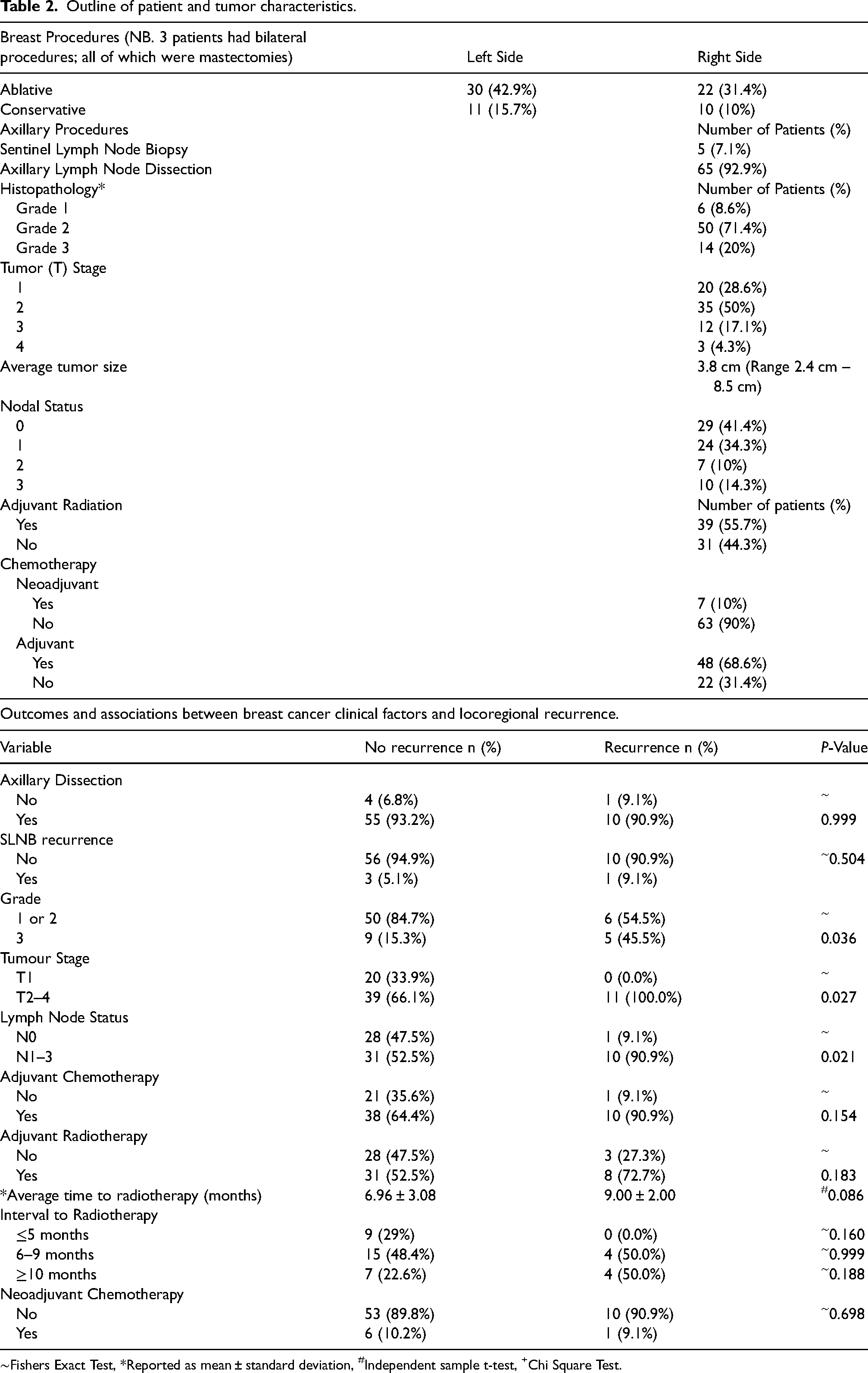
∼Fishers Exact Test, *Reported as mean ± standard deviation, #Independent sample t-test, +Chi Square Test.
There was no significant association between demographics, family and social history, and cancer-specific death (Table 3). Of note, there were positive associations between higher grade and breast cancer-specific death. Of those who had cancer-specific death, 50% of those patients with grade 3 breast cancers died, as compared to 12% of those with grades 1 and 2 cancers after 3 years of observation (P = 0.003).
Association between breast cancer clinical factors and breast cancer-specific death.
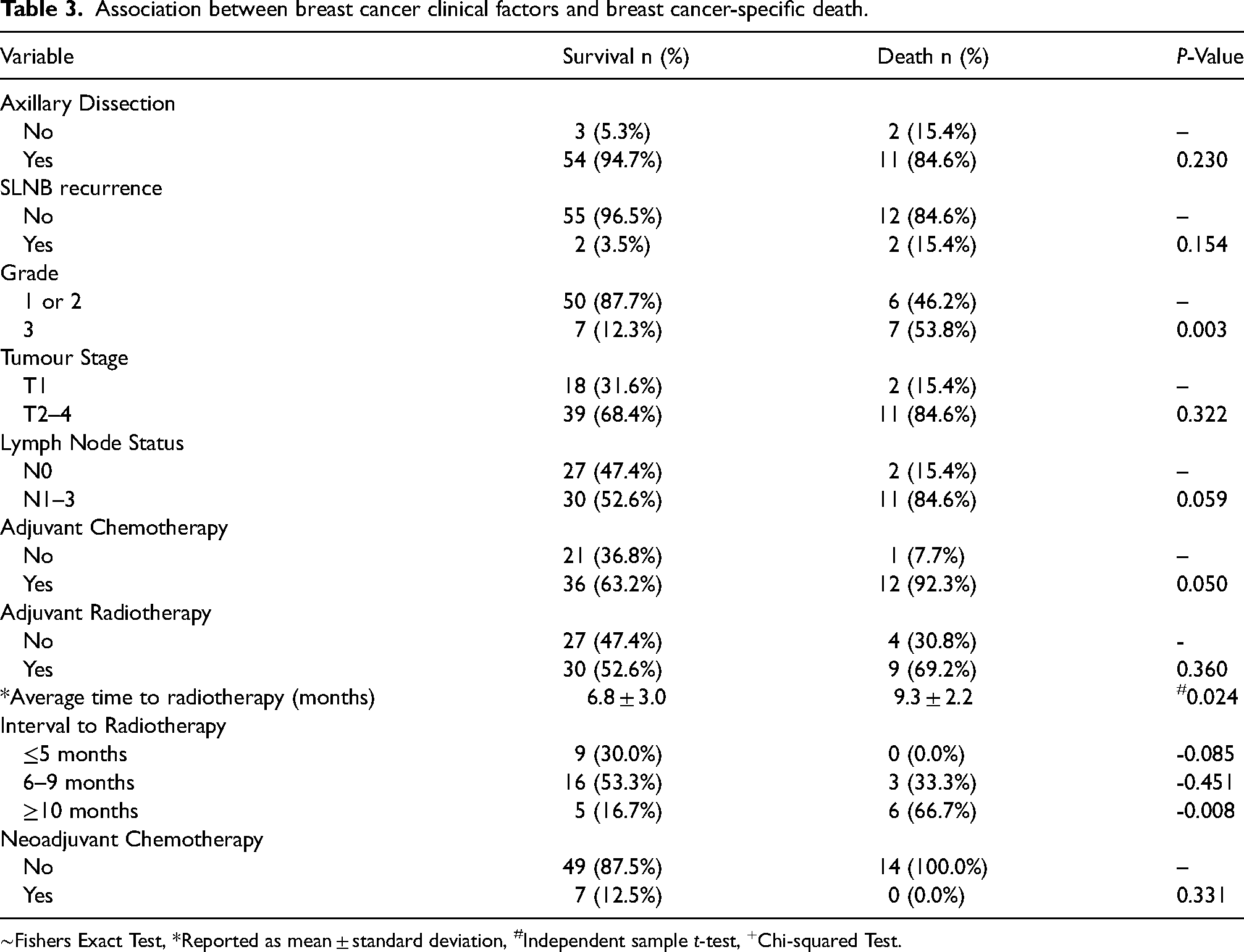
∼Fishers Exact Test, *Reported as mean ± standard deviation, #Independent sample t-test, +Chi-squared Test.
In the subset of patients who received radiotherapy, those who died had an average wait time of 9.3 months versus 6.8 months in those who survived (P = 0.024) There was a non-statistical trend toward having had adjuvant chemotherapy and a higher lymph node stage as significant risk factors for death.
Binary logistic regression analysis with and without adjustment for association between surgery type and breast cancer-specific death demonstrated conservative surgery as significantly associated with increased odds of cancer-specific death in the unadjusted model, (OR 18.76 (3.56–98.97), P-value 0.001). Even after adjustment for confounders of grade, nodal disease, adjuvant chemotherapy and radiotherapy delay, this positive association persisted.
Discussion
The rationale for whole breast irradiation, even with clear margins after resection, partly came from the works from Holland et al. 5 Irradiation of the myocardium in breast cancer is an important consideration when planning postoperative adjuvant therapy. A significant proportion of our population possesses cardiac risk factors. According to the Pan American Health Organization (PAHO), in Trinidad and Tobago, heart disease and hypertension accounted for 62% of all cases of premature death in women between 30 and 69 years. 6 This was reflected in a considerable proportion of our demographic in this study, making radiation therapy in left-sided breast cancer a matter of serious consideration. This was an important point in our patient population as those who had a history of ischemic heart disease were advised to have a mastectomy and avoided the use of adjuvant radiation without jeopardizing treatment decisions and remained oncologically safe. These patients had T2 cancers without evidence of nodal positivity or lymphovascular invasion and were all over the age of 65 years.
There is no standardization concerning starting radiotherapy postoperatively. 7 A delay over 7 weeks may allow replication of clonogenic cells at the Tumour bed, with the ability to become radioresistant. 8 Such delay constituted a statistically significant loss in survival even adjusted for chemotherapy requirement, age, stage, period of diagnosis and grade.9–11
Our study was retrospective, looking at patients under a single management team in a single health care institution with a limited catchment area, resulting in a small sample size. There were some inconsistencies in the documentation of pertinent findings regarding adjuvant therapy and surveillance in the records available for analysis. A portion of medical records of the patients was not located as they are paper-based and there is no electronic database that records this information and they were excluded from the study. Documented local recurrences in the follow-up period may have included second primary cancers in addition to true local recurrences.
Local recurrence is a well-established harbinger of poorer oncologic outcomes as well as increased health care expenditure, thereby steepening the burden on our already limited resources. Therefore, an earnest attempt must be made in the management plan for each patient to lower this risk as much as possible. Prolonged delays before instituting adjuvant radiotherapy increase both local recurrence rates and risk of death. Re-organizing resources can often result in the deployment of limited resources more efficiently.
Footnotes
Acknowledgements
The authors would like to sincerely thank the Department of Clinical Surgical Science of the University of the West Indies, as well as the Ethical Committee of the North Central Regional Health Authority for their support in the production of this research paper.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.