
Abstract
Respiratory distress syndrome (RDS) is common and is a leading cause of death in pre-term infants. The purpose of our study is to describe the demographics and incidence of adverse events in very low birth weight (VLBW) pre-term infants with RDS treated with surfactant at George, a level 2 Hospital in the Western Cape Province of South Africa. This was a retrospective observational study. We conducted an electronic folder review of infants with a birth weight of 800–1200 g treated during the study period 2017–2019 at George Regional Hospital. Outborn infants and those with congenital abnormalities were excluded. The total number of patients included in the study was 66. The mortality rate was 25.8% (17/66). The incidence of bronchopulmonary dysplasia was 6% (4/66). Our study showed that the outcomes of VLBW infants treated with surfactant at level 2 hospitals are comparable to South African central hospitals.
Introduction
The neonatal mortality rate for South Africa is currently 12/1000 live births and has remained stagnant for the past decade. 1 Neonatal deaths account for >70% of the under 5 mortality rate. 1 Prematurity-related causes accounted for 49.2% of neonatal deaths in South Africa in 2018. 2 The proportion of early and late neonatal deaths occurring at a tertiary institution ranged from 14.6–18.9% nationally in 2019. 2 This highlights the fact that a majority of neonatal deaths occur outside tertiary institutions.
The Eden district in the Western Cape (WC) is outside the main urban hub of the province and has no tertiary hospital, the closest tertiary neonatal unit being over 400 km away. In the year 2019, this district recorded 1415 infants born with a birth weight lower than 1.5 kg, this represented 10.8% of the total live births. Survival for this group was 91.6%, according to the Perinatal Problem Identification Programme. 1
Respiratory Distress Syndrome (RDS) is related to immaturity of the lungs and insufficient endogenous surfactant. Exogenous surfactant administration combined with non-invasive or invasive mechanical ventilation is now the mainstay of treatment. This has significantly improved the outcome. 3
Surfactant is a combination of lipids and proteins that lines the alveoli and lower airways. It lowers the surface tension at the alveolar membrane. This prevents alveolar collapse and improves lung compliance, resulting in rapid oxygenation and decreased work needed in breathing. 3 Surfactant treatment has been shown to result in significant improvements in oxygenation, less pulmonary air leaks and interstitial disease compared to controls. 4
The method known as the Intubation Surfactant Extubation (INSURE) method combined with continuous positive airway pressure (CPAP) was found to be the most effective way of administering surfactant.5–8
The neonatal viability criteria as defined by the Western Cape Policy Document for secondary hospitals allow for the administration of surfactant in infants with a birth weight >800 g. 9 Level 2 Hospitals around the Western Cape have access to non-invasive mechanical ventilation and surfactant. They also have access to short-term mechanical ventilation. 9 One of the General Paediatric consultants at George Regional Hospital (GRH) has a qualification in Neonatology, but the unit is staffed and functions as a level 2 facility.
A recent study explored the availability of resources for the provision of respiratory neonatal care across low- to middle-income countries and found that there was huge variation across counties. 10 Some 63% had CPAP available, but mostly in the most well-equipped government hospitals. 10
However, a majority of countries (74%) reported that CPAP was available in <10% of cities with populations of >150,000. 10 This highlights the need to improve access to resources in order to decrease the neonatal mortality rate. By studying the outcomes outside tertiary centres, evidence grows to advocate for improved access.
Alternative, less invasive, methods such as nebulisation, administration though a Laryngeal mask airway and introduction by thin catheter in a spontaneously breathing patient are currently under investigation. Preliminary evidence from these trials shows that these also result in decrease in mortality and incidence of chronic lung disease,11–14 and a systematic review in 2017 suggested they were even superior. 14
Beractant as a surfactant at a dose of 100 mg/kg was administered using the Less Invasive Surfactant Administration technique; those infants already mechanically ventilated were given via their endotracheal tube. The INSURE method was used in some infants.
Our institutional guideline recommends surfactant for infants with a FiO2 requirement >35–45% on CPAP. A repeat dose is recommended in 6–12 h if the oxygen requirements or the work of breathing are increased. The indications for starting mechanical ventilation were a FiO2 > 0.6 or respiratory acidosis (pH < 7.25) after surfactant administration and optimisation of CPAP.
Indications for HFOV are a high pCO2 or oxygen index not responding to mechanical ventilation. The guideline applies to all level 2 facilities as outlined in an internal circular. 9 To date, there has been little published data on outcomes of infants treated with surfactant outside tertiary centres, and to compare with their results.
Methods
We conducted a retrospective descriptive study between January 2016 and December 2019 based on folder reviews of electronic patient records at GRH, a level 2 Hospital in the Eden district of the Western Cape. Ethics approval was obtained for both the GRH Ethics Committee and the Human Research Ethics Committee at the University of Cape Town. There was no need for individual infant informed consent. We included inborn infants with a birth weight of 800–1200 g. We excluded outborn infants and infants with congenital abnormalities.
Our pharmacy could provide a complete accurate record of folder numbers of all patients given surfactant during the study period. Each physical patient file was scanned and uploaded including the nursing notes, patient results sheets and any prescription charts.
We then conducted an electronic folder review of patients treated with surfactant during the study period and collected the data on the case report form (Annexure B). The case report form results were then recorded on a coded data sheet to protect identifying information and ensure confidentiality of patients. The data regarding the use of antenatal steroids were incomplete in the infant folders, and there was limited access to maternal records and thus this was excluded from the analysis.
Data were then analysed using the Statistical Package for Social Sciences (SPSS) and were found to have a skewed distribution. Therefore, we reported the median and the interquartile range for the demographic data and the outcomes of interest. Due to the limited sample size and the distribution we conducted Pearson's χ2 test on SPSS to test for independence. Thus a descriptive analysis was done.
The primary outcomes were mortality and the incidence of adverse events; namely pulmonary air leak including pneumothorax, pneumomediastinum, pneumopericardium and pulmonary interstitial emphysema and pulmonary haemorrhage as evidenced by blood suctioned from the trachea post intubation.
Bronchopulmonary dysplasia was defined as need for supplementary oxygen at 36 weeks post menstrual age if born before 32 weeks or at 56 days post menstrual age if born after 32 weeks. Secondary outcomes were the duration of mechanical ventilation, number of days on supplementary oxygen, number of days admitted and the number of doses of surfactant required.
Results
A total number of 124 patients was identified, of whom 35 were excluded owing to birth weight out of range, 4 because of congenital abnormalities and 19 being out-born.
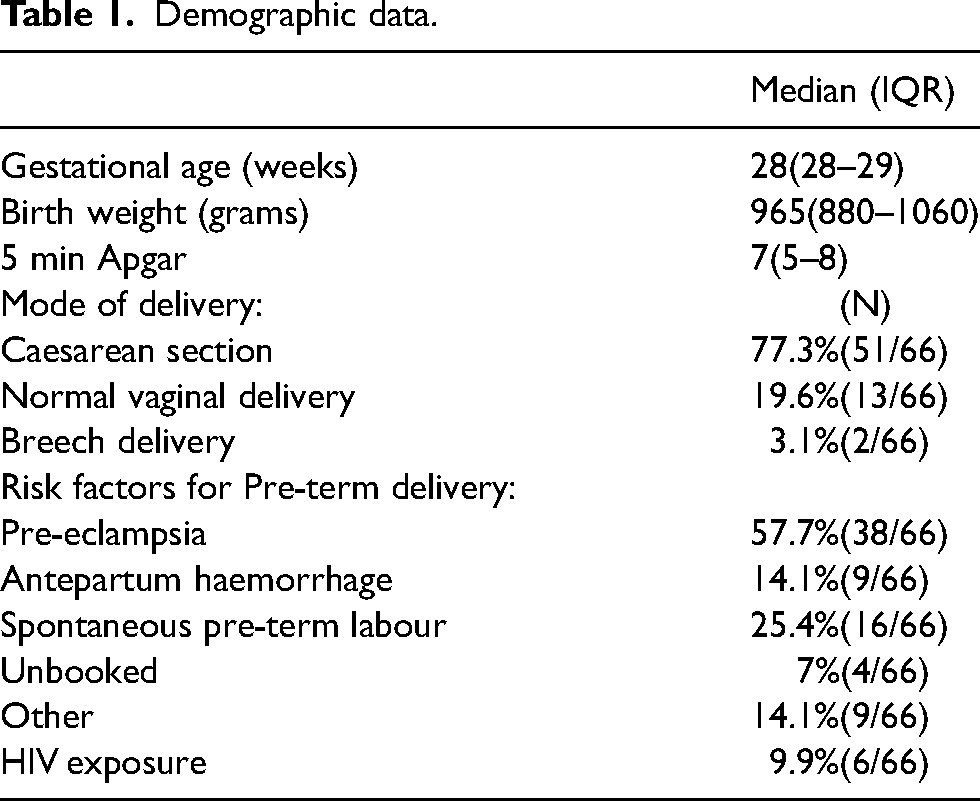
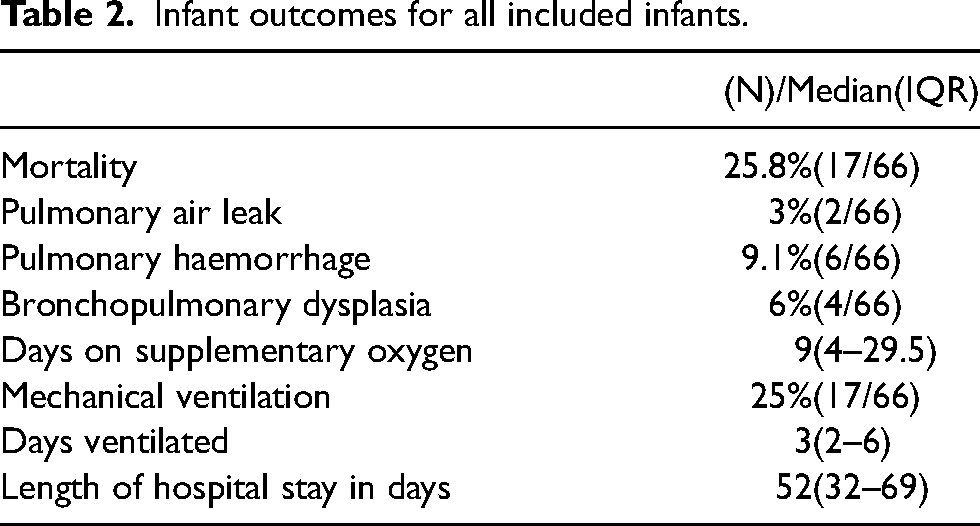
This left a total of 66 patients that were included in the analysis. Patient demographic data are represented in Table 1, and the patient outcomes data for the entire cohort are outlined in Table 2.
Demographic data.
Infant outcomes for all included infants.
Some 44 (66.7%) received a single dose of surfactant. The median time to first dose was 5 h (interquartile range [IQR] 2–16). A second dose of surfactant was given to 22 patients. The median age at second dose was 18 h (IQR 8–26). Mechanical ventilation was required in 11 (50%) who received a second dose compared to (7/44, 15.9%) who received one dose (p = 0.003).
The total number of days on oxygen was 8 days (IQR 4.5–19.5) for those who received a single dose of surfactant, and the median total days admitted was 28 days (IQR 7.5–55).
Of the 31 patients with a birth weight >1000 g, 12/31, 39.1% required mechanical ventilation (p = 0.012), and of the 35 patients with a birth weight <1000 g, (5/35, 14.3%) (p = 0.012) did so. A comparison of their outcomes is found in Table 3.
Infant outcomes by mode of ventilation and birth weight.
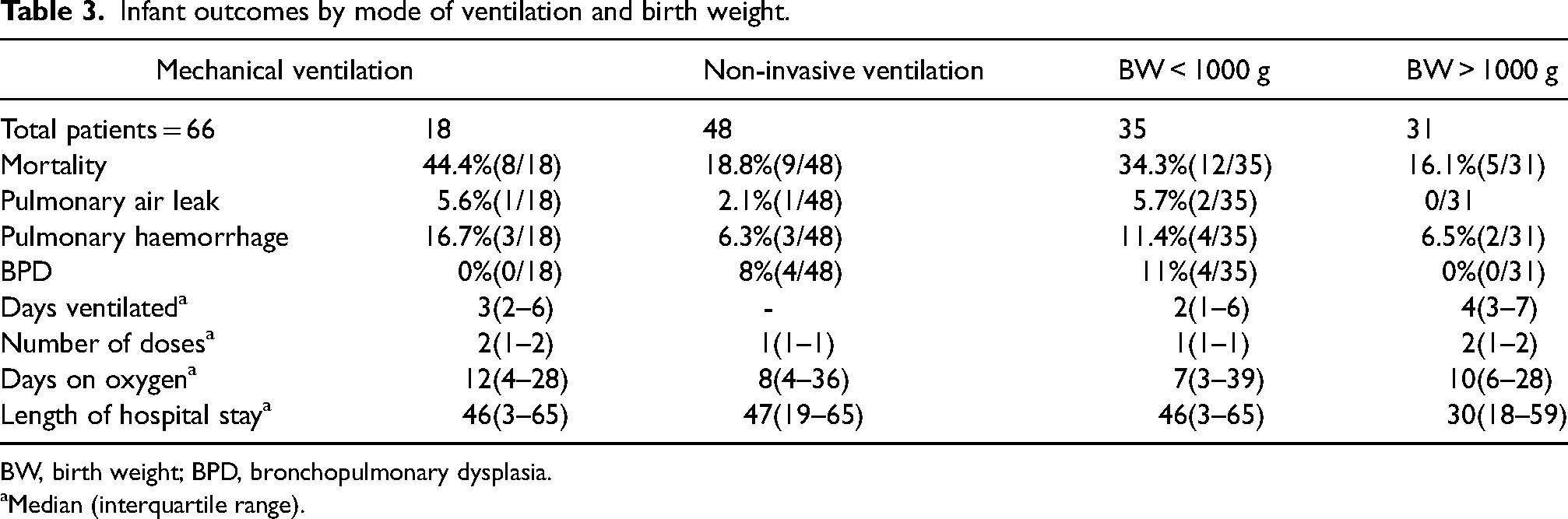
BW, birth weight; BPD, bronchopulmonary dysplasia.
Median (interquartile range).
There were 17 patients who demised, with a median birth weight of 900 g (IQR 880–1010), and a median gestational age of 28 weeks (IQR 27–29). Fatalities who required mechanical ventilation were (8/17, 47%) compared to (10/49, 20.4%) of survivors (p = 0.034).
The median number of days alive in hospital for the participants who died before discharge was 3 days (IQR 2–12 days). The incidence of pulmonary haemorrhage was (6/17, 35.3%) in those who demised while none of the survivors had a pulmonary haemorrhage (p < 0.001).
Discussion
Our study confirms that surfactant can be given safely at level 2 hospitals. Most of the research done in developing countries thus far has been conducted in tertiary institutions. We found that there was a comparable incidence of mortality with published data from local tertiary institutions, bearing in mind that more unwell patients and complex cases tend to be seen in tertiary centres. The incidence of BPD and pulmonary air leaks was similar to findings in tertiary centres.
Level 2 hospitals in the Western Cape all have access to surfactant, CPAP and mechanical ventilation. Therefore, the services provided are standardised across the level 2 facilities. George Regional Hospital has access to the same package of resources as other level 2 facilities. The policy is for in-utero transfer if the pregnant woman presenting with pre-term labour if possible. A recent study done at a tertiary hospital in Cape Town showed that inborn infants had better outcomes and this was used to advocate for in utero transfers of at-risk patients. 15
At level 2 Hospitals, there is a capacity for short-term ventilation for infants with a birth weight >1000 g. George Regional Hospital in selected cases can ventilate infants with a birth weight >800 g, this would typically be offered to inborn infants that were exposed to antenatal steroids. This was done in order to increase equity as GRH is the facility furthest level 2 hospital from tertiary facilities and emergency transfers can often be challenging. 9 The distance from GRH to the nearest tertiary hospital is over 400 km. This may influence the outcomes in this category of infants.
A recent retrospective study done in South Africa found no significant difference in outcomes comparing infants with a birth weight less than 1500 g treated with either Poractant alfa or Beractant. 16 Poractant alfa and Beractant were both previously available in the public sector. Poractant alfa was removed due to costs and the evidence to support its use in the public sector was deemed to be insufficient. The patients included in our study were all treated with Beractant as the study period fell after the above-mentioned changes in procurement.
Our study outcomes were in keeping with a recent study by Boshoff et al. of very low birth weight (VLBW) infants treated with surfactant at a tertiary hospital (see Table 4 for comparisons). 16
Comparison with data from Boshoff et al. 16
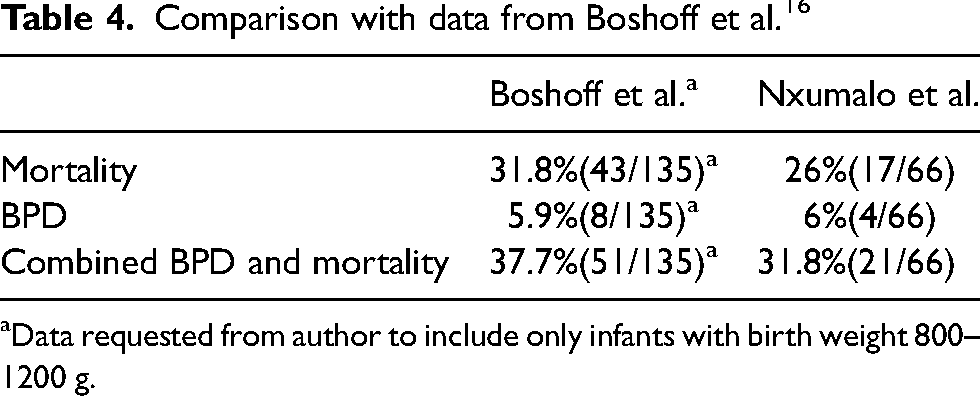
Data requested from author to include only infants with birth weight 800–1200 g.
The primary outcome in both studies was mortality and the incidence of adverse events. The published study included infants that were of VLBW, we contacted the author to provide data only for infants with a birth weight 800–1200 g.
The incidence of death in our study 17/66 (25.8%) was lower than the incidence of death in the aforementioned study 43/135 (31.8%), as well as a study done at a central hospital in Johannesburg 241/633 (38.1%).16,17
The median number of days on mechanical ventilation for cohort 3 (2–6) was higher than the outcomes of a recent study done at a central hospital in South Africa 1 (IQR 0–2). 16
One of the limitations in the study was the relatively small number of patients that could be included. The retrospective nature of the study made it prone to misclassification bias from the variable amount of detail available in the patient records.
The study was performed at a regional hospital where there were a limited number of deliveries of VLBW infants. We utilised a convenience method of sampling with limited exclusion criteria in order to include as many participants as we could. This may introduce bias as the small sample size may not be a true reflection of the population but rather a reflection of the patients who were admitted during the study period.
Access to maternal records was limited and the majority of mothers had not had an early ultrasound. Therefore, we used the consensus gestational age in our study. This was estimated by taking the Ballard score, the foot length and the last day of the Mother's last normal menstrual period into consideration.
Our study period was selected to include the earliest electronic case records available at the study site. This was done to mitigate the effects of missing data and incomplete or lost case records.
Conclusion
Regional hospitals have limited capacity for ventilatory support of pre-term newborns. This study showed that adverse outcomes in very pre-term infants with RDS treated with surfactant at a regional Western Cape hospital were similar to outcomes at central hospitals in South Africa.
We recommend further research be done to explore how the incidence of adverse events can be reduced in VLBW infants. Future studies are needed to explore the long-term outcomes, including neurodevelopmental outcomes of VLBW infants treated with surfactant at level 2 hospitals. This would require a well-designed cohort study with adequate follow-up.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The investigators are not affiliated with any drug company nor have we received any external funding. The statistical support was paid by the University of Cape Town Department of Paediatrics and Child health. This research is intended for submission as a mini-dissertation for the MMed in Paediatrics and Child health at the University of Cape Town. Any intellectual property emanating from this research project will belong to the University of Cape Town.