
Abstract

Case report
A 1-year old infant, first born to non-consanguineous parents, presented with global delay and increased tone for six months. There was no history of seizures, irritability, skin or hair changes, abnormal odour, neuroregression, vision, nor hearing problems. The mother had an antenatal exanthematous febrile illness. The perinatal period was uneventful and family history was unremarkable. Examination revealed microcephaly, retrognathia, sacral Mongolian spots, hypertonia, brisk deep tendon reflexes, and Babinski's sign. Fundal examination showed tessellated fundi. The rest of the systemic examination was unremarkable. Brain-stem evoked response audiometry, and two-dimensional echocardiography were normal. A clinical diagnosis of global developmental delay secondary to structural (including intrauterine infections), metabolic, or genetic insults was considered.
Brain magnetic resonance imaging (MRI) showed hyperintense signals in the periventricular and deep cerebral white matter, multiple subcortical cysts, and adjacent gyral abnormalities involving the frontal and temporal lobes, suggesting vacuolating myelinopathy (Fig. 1). Congenital cytomegalovirus (CMV) IgG titres were raised in both the infant and mother (infant: IgG 250, IgG avidity 60.2, IgM 0.15 (normal > 1); mother: IgG avidity 92.56). Polymerase chain reaction for CMV DNA from blood was positive in the infant. Oral valganciclovir, physical therapy, and early intervention programs were initiated. At the 6-month follow-up, the child significantly gained milestones in all domains.
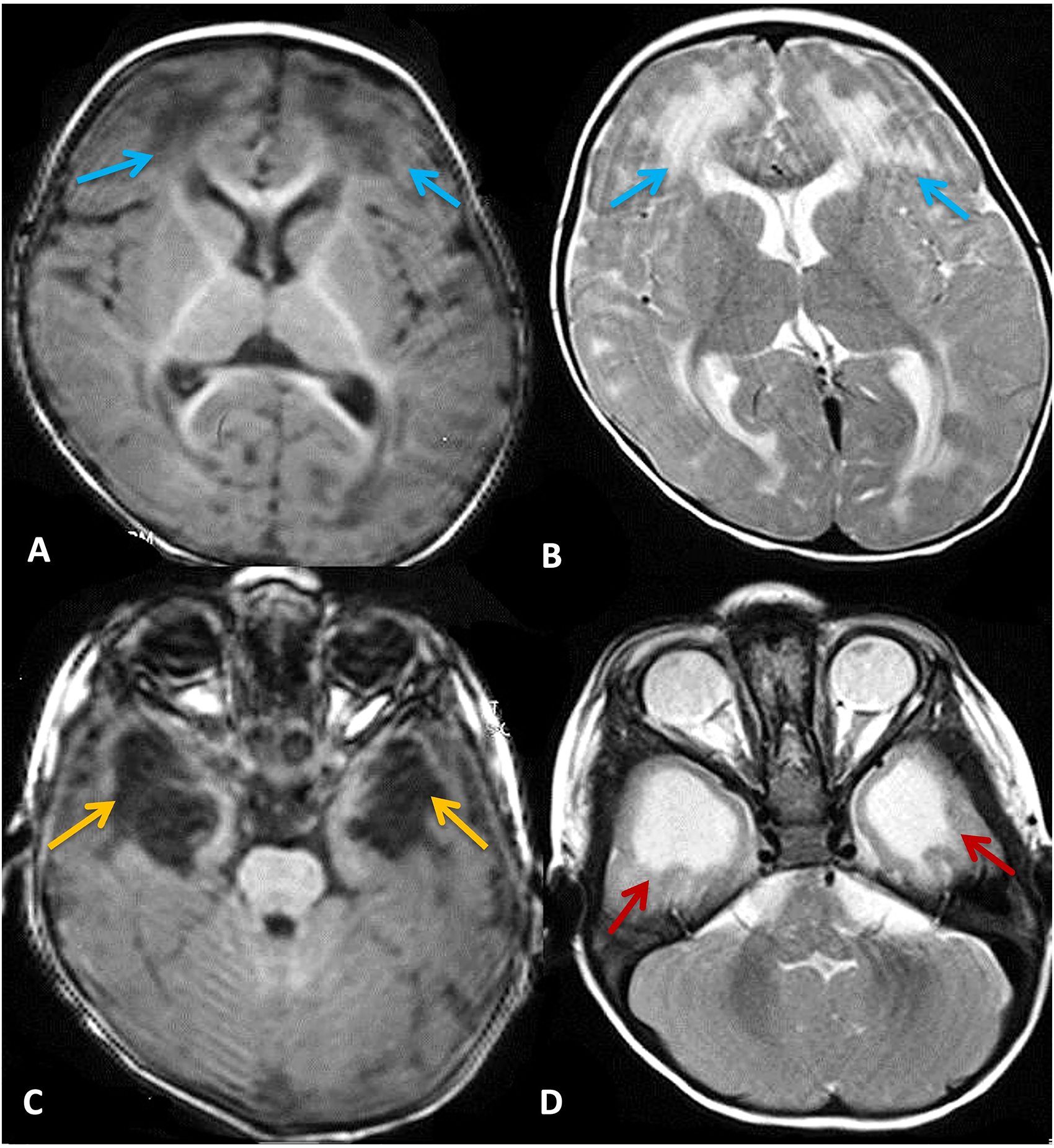
Cystic leukoencephalopathy in congenital cytomegalovirus infection. Note: MRI brain showing areas of T2/FLAIR hyperintensities in periventricular and deep white-matter of both cerebral hemispheres. The lesions showed increased diffusion in cerebral white-matter (bright on ADC, dark on DW1) (blue arrows). The corpus callosum, basal ganglia, thalami are relatively spared. Multiple subcortical cysts of varying sizes with adjacent gyral abnormalities are seen involving the frontal and temporal lobes (yellow arrows). There is associate dilatation of bilateral temporal horns of lateral ventricle (red arrows). The rest of the ventricular system is normal. Findings are suggestive of vacuolating myelinopathy. See online figure for colour rendering.
Congenital CMV infection is a major cause of cystic white matter degeneration, particularly in LMICs. Neuro-imaging is the best single predictor of neurological outcomes in infants with congenital CMV infection, while leukoencephalopathy with anterior temporal cysts is a significant predictor of congenital CMV infection.1–3 The other features noted in CMV are dilated ventricles, enlarged subarachnoid spaces, and gyral abnormalities such as polymicrogyria. Although the exact pathogenesis of the temporal lobe involvement is not established, the in-utero CMV infection causes the release of proinflammatory cytokines that inhibit the development of dendrites in cortical neurons. 4 For the assessment of white matter abnormalities (WMAs), diffusion-weighted imaging should be done with conventional MRI.
Alarcón et al. 1 reported that in infants with isolated WMAs, temporal-pole WMAs have a higher risk of severe hearing loss or moderate/severe neurodevelopmental disabilities. They also reported that the absence of temporal-pole WMAs had a negative predictive value, suggesting a low risk of poor outcomes in infants with congenital CMV. The radiological progression of these WMAs includes gliosis and malacia. Hoffmann et al. 4 studied the effect of CMV infection on temporal lobe development using volumetric measurements of fetal MRIs. Their study revealed a notable reduction in temporal lobe/whole brain volume ratios among the CMV-infected fetuses despite the absence of evident neuroimaging anomalies. Besides congenital CMV, common differentials for cystic leukoencephalopathy are mitochondrial respiratory chain disorders, megalencephalic leukoencephalopathy, Aicardi-Goutières syndrome, and vanishing white-matter disease. 1
Congenital CMV is one of the leading infectious causes of neurodevelopmental disabilities and sensorineural hearing loss and the low- and middle-income countries (LMICs) suffer the highest burden.5,6 The neurological damage is primarily caused by the destruction of brain parenchyma by the CMV itself. In a systematic review and meta-analysis by Ssentongo et al., 5 the estimated pooled birth prevalence of CMV in LMICs is 1.42% (0.97%–2.08%, 95% CI), three times higher than in high-income countries. The contribution of congenital CMV to neurodevelopmental disabilities in poorer countries is significant due to higher birth rates and additional health challenges faced by affected children. 6 Recognition of temporal lobe WMAs and cysts may be a novel guide for diagnosing congenital CMV in addition to other commonly known neuroimaging markers.
Footnotes
Authors contributions
All the authors contributed equally to the study design, writing, editing, drafting, critical revision, and final approval.
Data availability
No datasets were generated during the study.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical publication statement
We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that this report is consistent with those guidelines.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Patient consent statement
Written informed consent was obtained from the parents.