
Abstract
The primary goal of breast conservation surgery (BCS) is to achieve tumour-free margins. However, it is known that in 20% patients, a tumour-free margin may not be obtained. Positive margins frequently lead to re-operation and are the strongest predictors of local recurrence. We therefore evaluated the performance of ultrasound (US) and frozen section (FS) in predicting the margin status of lumpectomy specimens of ultrasound-detectable breast carcinoma patients undergoing BCS. In our prospective study on 54 patients who underwent lumpectomy, the margins were analyzed by ultrasound and frozen section. Patient-wise and margin-wise diagnostic parameters were calculated for both modalities.
Keywords
Introduction
BCS is the standard of care for patients with early breast cancer, and even for some locally advanced breast cancers responding favourably to neoadjuvant chemotherapy (NACT). The primary goal of BCS is to achieve tumour-free margins. However, this may not be obtained on postoperative histopathological evaluation of lumpectomy specimens, which is the current gold standard for predicting the status of margins. 1
Positive margins lead almost inevitably to complications.2–4 Visual inspection and palpation of the lumpectomy specimen is a universally applied intra-operative method for predicting tumour-free margins. Despite its inaccuracies, this method is a commonly used method of intraoperative margin evaluation. 5 Besides being inexpensive and rapid, it does not require any specialized machinery or trained personnel other than the surgeon. The absence of a foolproof tool has also allowed many surgeons to continue with this method as the only tool for margin assessment during BCS. The absence, however, of a foolproof tool obliges a search for such a tool.
A host of modalities for intraoperative assessment of margins have been evaluated. These include specimen radiography (SR), 6 US,7–9 touch imprint cytology (TIC), 10 FS,11–13 micro-computerized tomography (micro-CT), 14 ex vivo MRI imaging,15,18 FDG-PET scan, 16 optical coherence tomography (OCT), 17 radiofrequency spectroscopy by MarginProbe Device, 18 bioimpedance spectroscopy: ClearEdge Device, 19 Raman spectroscopy combined with autofluorescence microscopy, 20 ultraviolet-photoacoustic microscopy (UV-PAM) and microscopy with ultraviolet surface excitation (MUSE). 21
While some of these should be considered investigational or too costly for routine use at present, SR, USG, TIC, and FS have been evaluated by multiple studies and found to be at least moderately accurate in predicting the status of the lumpectomy margins.
TIC and FS analysis have shown promise but are not widely utilized as the requirement of a trained pathologist is obligatory and the increase in operative time is prohibitive. The installation and running costs of a cryostat are problematic in low and medium-income countries (LMICs).
Intraoperative ultrasonography of the lumpectomy specimen has the potential to offset these limitations, especially for breast cancers initially detected on ultrasound. It is widely available, has minimal running costs, is rapid, and can be performed by surgeons in the operating room itself after minimal training.
Materials and methods
Our prospective cross-sectional study included patients with ultrasound-detectable breast carcinoma amenable to BCS either primarily or post-NACT between September 2021 and March 2025. The study was approved by the Institute Ethics Committee (IEC: AIIMS/Pat/PGTh/July 20/24).
Patients were evaluated according to the standard protocol and staged by the 8th AJCC manual. Patients with breast cancers not detectable on ultrasound (either primarily or after NACT) and patients who had multiple islands of residual tumours following NACT (found on imaging) were not included. All patients underwent wide local excision (WLE) of the tumour using palpation guidance with a > 1 cm margin (except where skin formed the anterior margin). The lumpectomy specimen was oriented with silk sutures [Fig. 1]. The status of the margins was assessed with ultrasonography [Fig. 1(a)] performed by a radiologist and then sent for frozen section analysis. The status of the margin was recorded in predesigned proforma and was mentioned to the surgeon once results of both modalities were available. Any margin < 2 mm on US was recorded as positive on ultrasound, while for FS, positive margins were defined as “ink on tumour”. If a margin was found to be involved using any modality, it was re-excised, and re-excised margins were again evaluated with the modality with which the lumpectomy margin was reported positive. The final margin status on haematoxylin and eosin (H & E) stained sections was considered the gold standard and results of ultrasonography and frozen section were compared against H&E section results. Statistical analysis was done using SPSS software (Version 24.0, Armonk, NY: IBM Corp.). Continuous variables were expressed as mean with standard deviation. Categorical variables were expressed as frequencies or percentages. The χ2 test was used to determine an association between the two categorical variables. A p-value < 0.05 was considered statistically significant. We calculated the patient-wise and margin-wise sensitivity, specificity, positive predictive value, negative predictive value, and accuracy for both modalities.
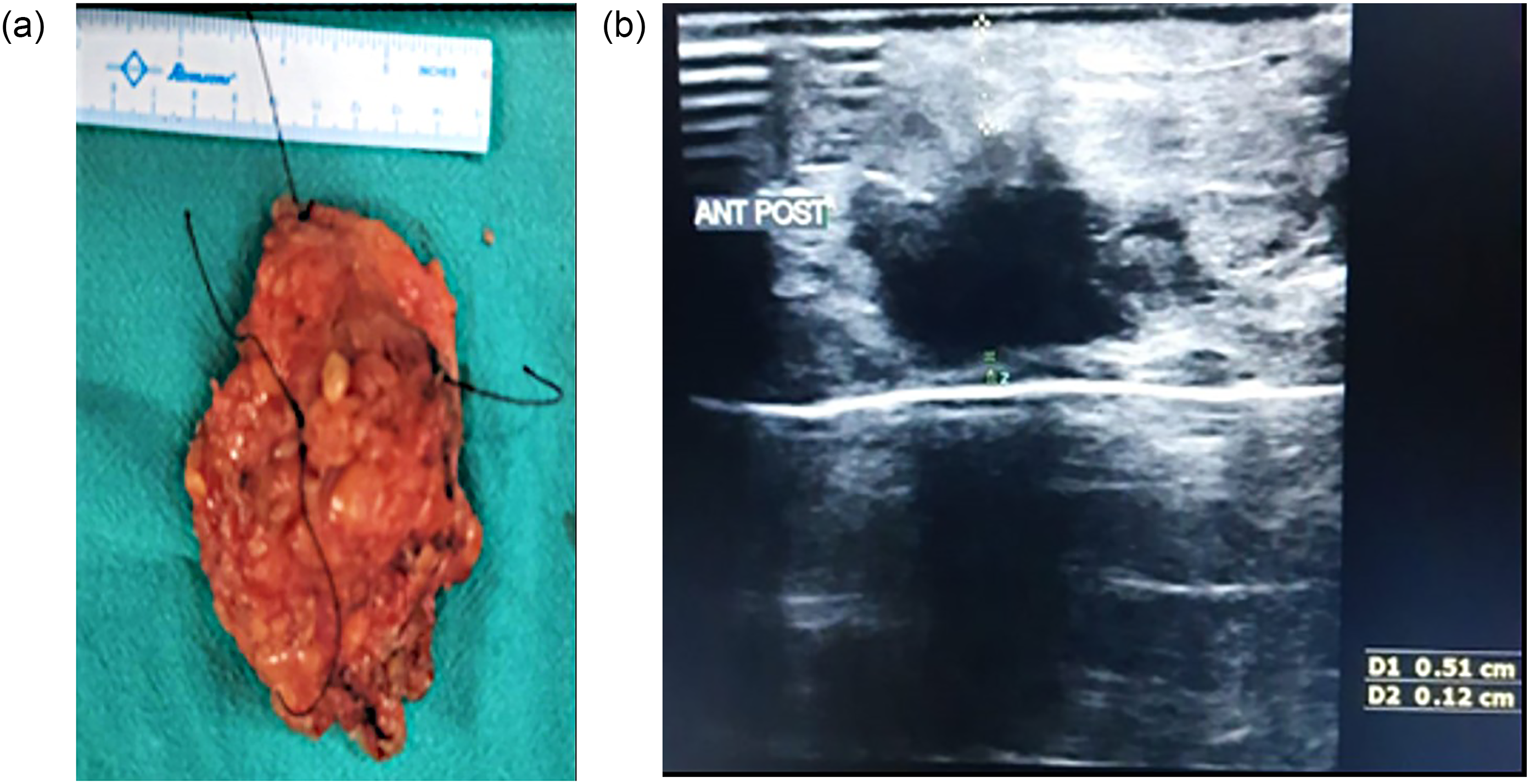
Figure 1a: Resected lumpectomy specimen marked with sutures. Upon inspection and palpation, the deep margin appeared to be close. Figure 1b: Ultrasound image of the lumpectomy specimen showing deep margin of 12 mm, which was reported as negative on frozen section as well as HPE.
Results
A total of 54 consecutive patients with ultrasound-detectable breast carcinoma were included. Of these, 20 (37.0%) had received neoadjuvant chemotherapy to facilitate BCS. The clinico-pathologic profile of patients is presented in Table 1. The mean margin width reported on H&E sections (excluding the anterior margin) was 1.4 ± 0.9 cm.
Clinicopathological profile.
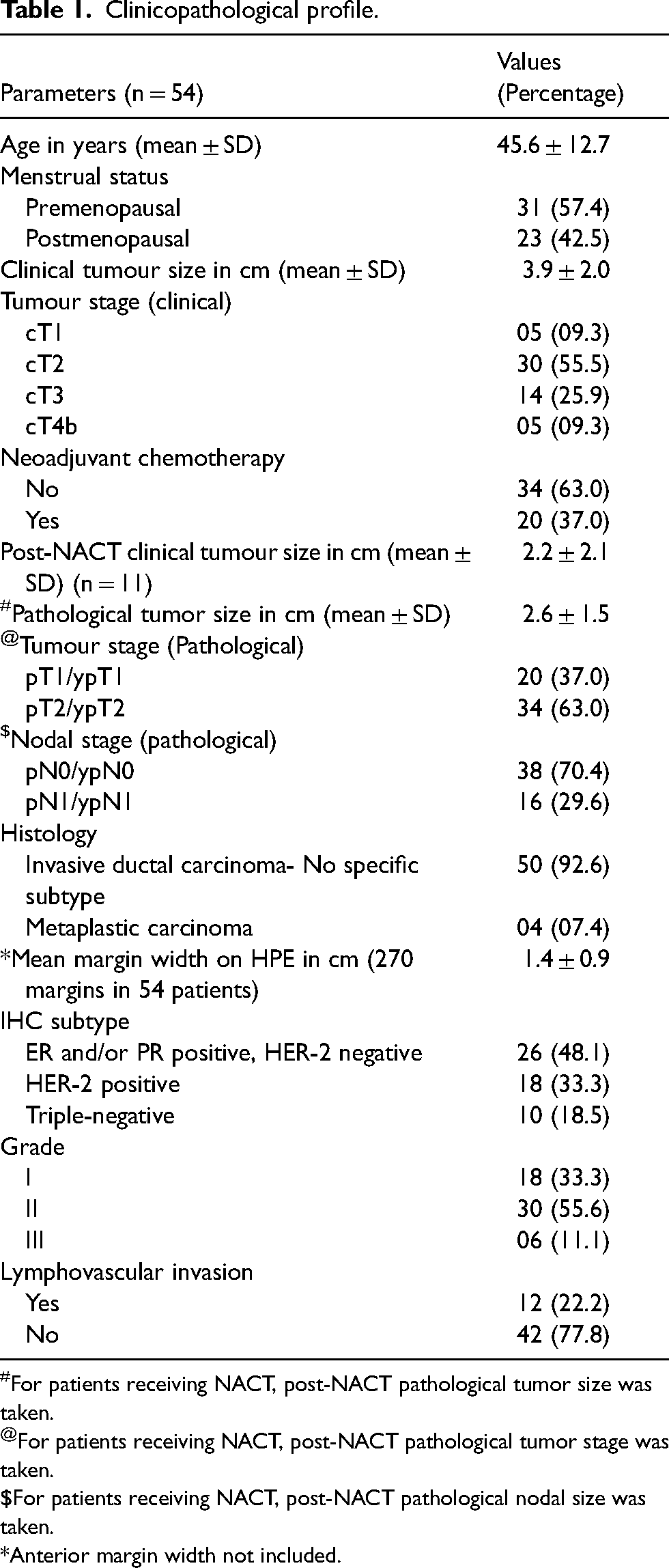
For patients receiving NACT, post-NACT pathological tumor size was taken.
For patients receiving NACT, post-NACT pathological tumor stage was taken.
For patients receiving NACT, post-NACT pathological nodal size was taken.
*Anterior margin width not included.
Patient-wise diagnostic parameters (Table 2) were calculated for all 54 patients for US, but it could only be done for 53 for FS because one margin in a patient turned out to be false positive and the other false negative. We also calculated the margin-wise diagnostic parameters. We did not include the results of anterior margins for these calculations; five margins for each of the 54 patients were analyzed (Table 3).
Patient-wise diagnostic parameters.
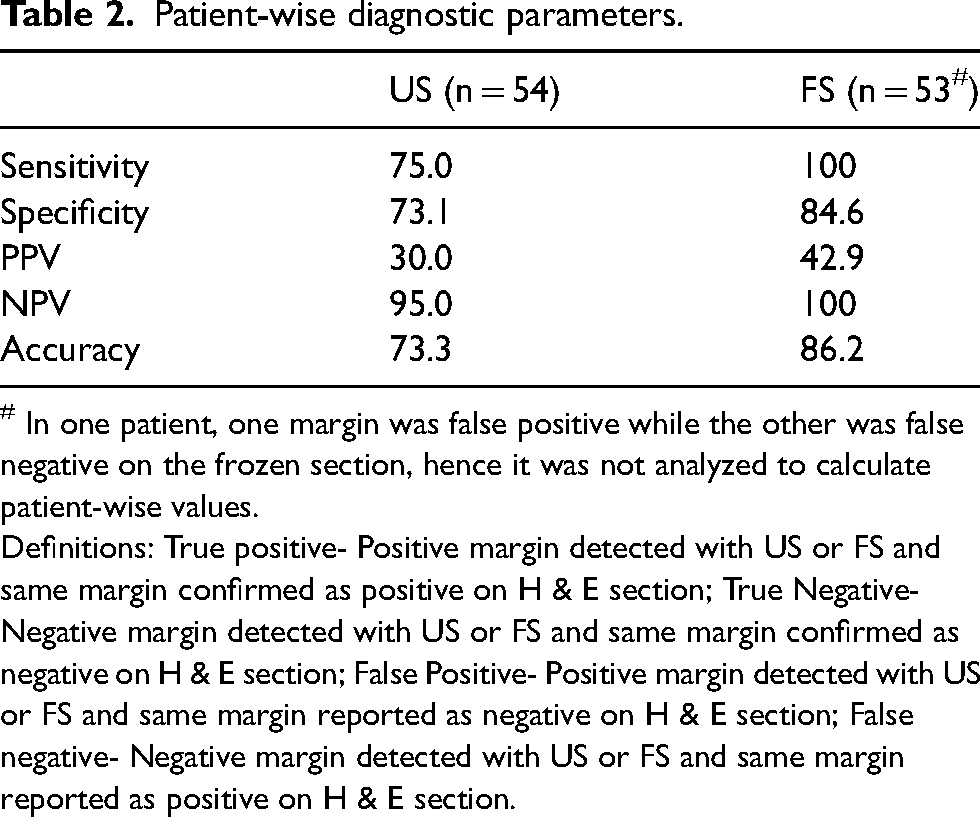
# In one patient, one margin was false positive while the other was false negative on the frozen section, hence it was not analyzed to calculate patient-wise values.
Definitions: True positive- Positive margin detected with US or FS and same margin confirmed as positive on H & E section; True Negative- Negative margin detected with US or FS and same margin confirmed as negative on H & E section; False Positive- Positive margin detected with US or FS and same margin reported as negative on H & E section; False negative- Negative margin detected with US or FS and same margin reported as positive on H & E section.
Margin-wise diagnostic parameters (n = 270).
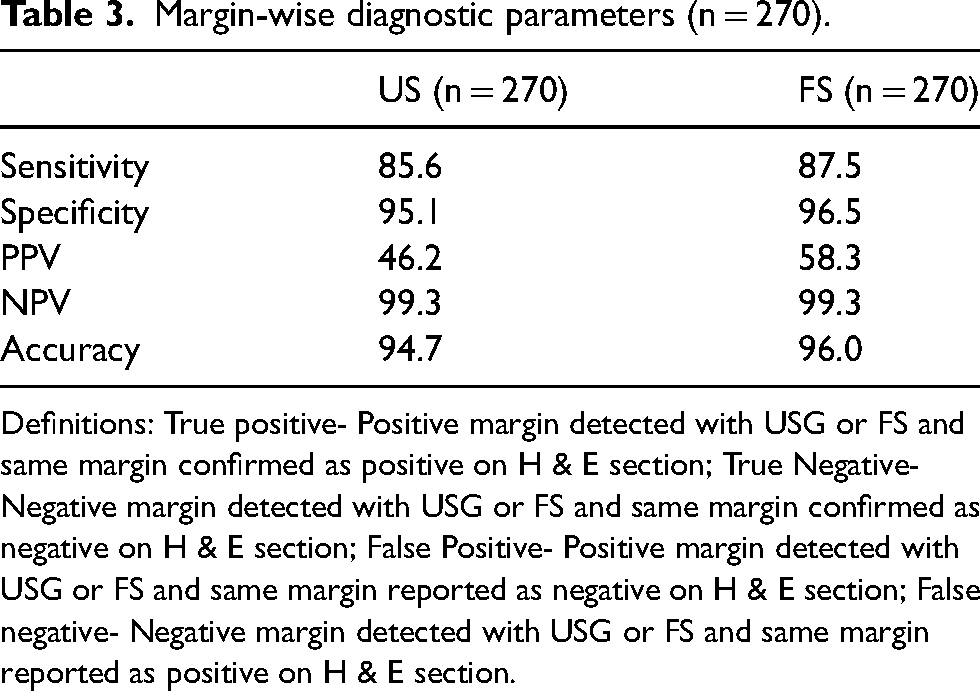
Definitions: True positive- Positive margin detected with USG or FS and same margin confirmed as positive on H & E section; True Negative- Negative margin detected with USG or FS and same margin confirmed as negative on H & E section; False Positive- Positive margin detected with USG or FS and same margin reported as negative on H & E section; False negative- Negative margin detected with USG or FS and same margin reported as positive on H & E section.
Discussion
FS had excellent patient-wise sensitivity of 100%, NPV of 100%, and a very acceptable specificity of 85%, because there were no false negatives. The margin-wise sensitivity (87.5%), specificity (96.5%), and NPV (99.3%) were also more than acceptable.
In comparison, the patient-wise sensitivity, NPV, and specificity of ultrasound were 75%, 95%, and 73.1%, while the margin-wise sensitivity, NPV, and specificity were 85.6%, 99.3%, and 95.1% respectively.
The most important concern while performing a BCS is to avoid positive margins during lumpectomy. Positive margins create anxiety in the patients, and confidence in the surgeon is often then lost. Furthermore, reoperation puts an extra burden on an already stressed healthcare delivery system and may also impact the cosmetic outcome.
Hence, the most important diagnostic parameter in our study was the NPV of US and FS. Having a high value of NPV means that there are fewer false negatives. 22 US had a patient-wise NPV of 95% and a margin-wise NPV was 99.3% which was comparable to the values of FS (patient-wise NPV of 100% and a margin-wise NPV was 99.3%). The PPVs, both patient-wise and margin-wise, were low for both USG and FS, meaning that false positive rates would be higher using both these techniques.
A meta-analysis of the diagnostic accuracy of intraoperative techniques for margin assessment in breast conservation surgery including 35 studies found frozen section to be more accurate than ultrasound (pooled sensitivity, specificity, and area under the receiver operating characteristic curve of 86%, 96%, and 0.96 for frozen section versus 59%, 81%, and 0.78 for intraoperative ultrasound). 23 An older systematic review found frozen section to be an accurate modality, but consumed 20–30 min of extra time, while at a margin width of 2 mm, US had a 99.6% accuracy, with only a 4% second operation rate. 24
There is considerable evidence demonstrating the viability, dependability, safety, and cost-efficacy of the FS in margin assessment, although it is still not the standard of care. We routinely use FS at our institute and have little doubt about its accuracy. The only problem that we face is the prolonged waiting time for the FS results, which adds to the operative time and cost. Specimen ultrasound requires five minutes, is widely available, and has minimal operating cost. Although all US examinations were performed by a single experienced radiologist in the radiology department, US of specimens can be done in the operating room by surgeons with minimal training.25,26
Various authors have employed different US margin widths to predict negative margins. Two recent studies reported excellent accuracy of US in predicting a negative margin when the margin width was ≥10 mm, one of those even reported a better accuracy of US than FS.27,28 Other studies have used a margin of 2–5 mm to evaluate the accuracy of US in predicting margin status.29–31 To the best of our knowledge, there are no published studies that have considered a margin narrower than 2 mm as a negative margin.
Conclusions
We conclude that US can be successfully used as a tool for margin assessment in patients undergoing BCS for US-detectable breast carcinomas.
Footnotes
Author contributions
Study concept and design: CKJ, SSP, JA, PPB
Acquisition of data: JA, SB, US
Analysis of data and interpretation: JA, SSP, CKJ
Drafting of the manuscript: CKJ, JA, SSP
Critical revision of the manuscript: PPB, SSP, US
Consent for publication
Written informed consent was obtained from all included patients for the publication of any potentially identifiable images or data included in this article.
Consent to participate
Written informed consent was obtained from all included patients.
Data availability
The datasets generated and analysed during the current study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and was approved by the Ethics Committee of All India Institute of Medical Sciences, Patna (AIIMS/Pat/IEC/PGTh/July20/24) on September 09, 2021.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Prior presentation
A part of this study was presented as an abstract at the Sri Lanka Surgical Congress 2024.