
Abstract

Case report
A 7-day old full-term male neonate weighing 3200 g with uneventful antenatal and birth history was referred for persistent mild respiratory distress (RD) since the second day of life. Chest radiography showed complete ‘white-out’ in the left thorax. He received multiple antibiotics on the presumption of pneumonia without any improvement. Repeated sepsis screen and blood cultures were negative.
On examination, the Downes score was 2/10, the left hemithorax appeared slightly flat with decreased air entry. The remaining general and systemic examinations were normal and dysmorphic features were absent. A repeat chest radiograph showed persistent opacification with ipsilateral crowding of the ribs and contralateral compensatory lung hyperinflation (Fig. 1a). Echocardiography showed a small hypoplastic left atrium with absent left pulmonary artery (Fig. 1b). Considering the possibility of left lung agenesis, a chest CT scan with pulmonary angiography was performed, which showed an absence of the left lung parenchyma and a rudimentary blind-ending left bronchus and absent left pulmonary artery suggestive of a type 2 pulmonary aplasia (Fig. 1c). Antibiotics were stopped and the neonate was discharged on the tenth day of life, with tachypnoea (respiratory rate of 60–65/min) with minimal chest retraction but maintaining peripheral oxygen saturation of 90% to 92% in room air, accepting breast feeds well and gaining weight. His parents were counselled concerning the maintenance of general hygiene, regular immunisation and early consultation for fever or increasing RD in order to prevent and treat any infections in timely fashion.
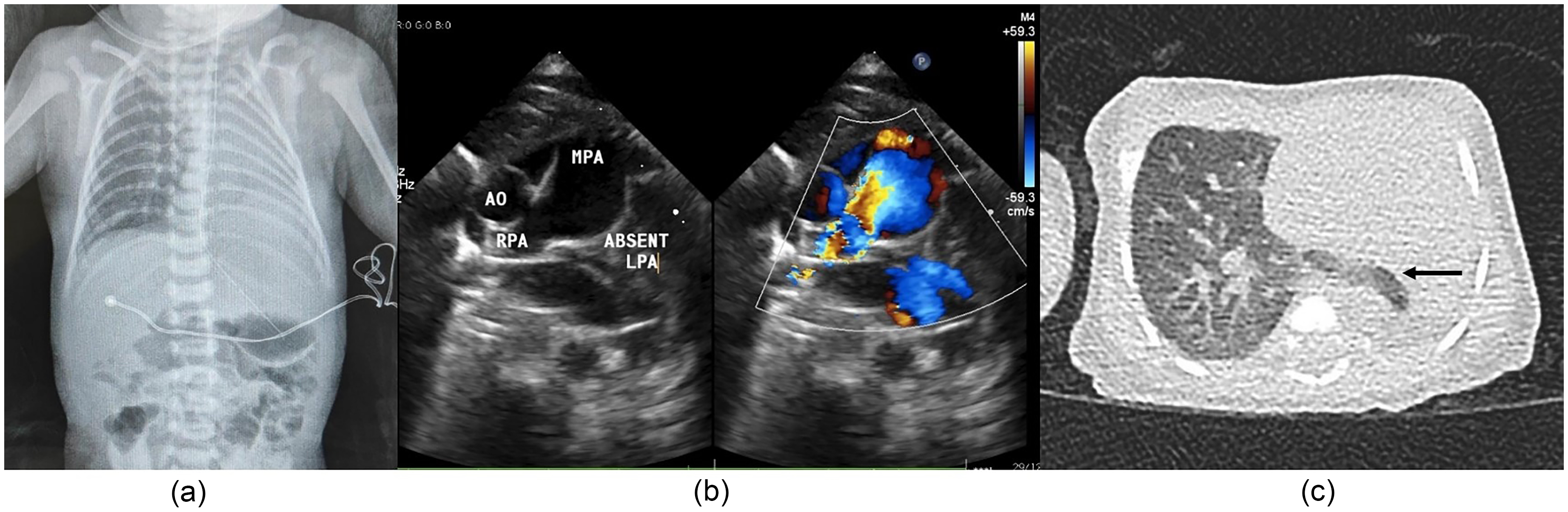
(a) Chest radiograph showing opacification of left hemithorax with crowding of ribs and contralateral compensatory lung hyperinflation; (b) parasternal short axis view echocardiography showing absent left pulmonary artery; (c) CT chest scan showing left lung agenesis with rudimentary bronchus.
Discussion
The common causes of unilateral radiological thoracic opacification in term neonates include pneumonia, collapse and pleural effusion. 1 Bedside echocardiography showing an absent pulmonary artery clinches the diagnosis 2 preventing undue prolongation of hospitalisation and exposure to antibiotics.
Pulmonary aplasia is a rare congenital anomaly with an incidence of 12 cases per million live births. 3 Embryonically, it results from failure of one or both lung buds to develop from primitive foregut at the 4th week of foetal life. Associated congenital malformations include respiratory tract anomalies (tracheal stenosis, oesophageal atresia, bronchogenic cyst and congenital diaphragmatic hernia), cardiac anomalies (patent ductus arteriosus, tetralogy of Fallot and anomalies of great vessels) and other deformations such as microphthalmia/anophthalmia, cleft palate, facial and limb defects, cleft palate, facial and limb defects.
Lung agenesis may be associated with syndromes such as VACTERL, Di George, Trisomy 21, Goldenhar and Mardini Nyhan syndromes.4,5
Pulmonary aplasia may be unilateral or bilateral, the latter being generally incompatible with life. Unilateral disease more often affects the left side (70%) and nearly 50% of cases present in the neonatal period with mild to severe RD depending on the presence of associated anomalies.
Babies with unilateral lung agenesis, in the absence of other congenital anomalies and minimal RD, may survive till adulthood with minimal or no symptoms. The overall mortality in unilateral disease is 30%.4,5
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The authors received no financial support for the research, authorship and/or publication of this article.
Patient consent statement
Patient's legal guardian provided consent to publish this report and the images.