
Abstract
Endoscopy remains the gold standard investigation for assessing the severity of corrosive digestive injuries. Our prospective observational study aimed to validate the ‘Med-Tu chart’ for the evaluation of corrosive injury, where endoscopy is not available, and found it to have an acceptable diagnostic accuracy in detecting the severity of corrosive ingestion.
Introduction
A nationwide study conducted in the United States demonstrated that their emergency department received c. 40,844 visits related to corrosive ingestion. 1 The incidence is expected to be much higher in low-income countries including India owing to lower literacy rates, a lack of knowledge about the effects of consumption, and insufficient containment of corrosives that result in inadvertent intake. According to a recent study on suicide poisonings, corrosives were responsible for 13% of suicide poisonings in India. 2 The incidence of corrosive ingestion is higher among the younger age group, aged 15–30, contributing to 80%. 3
According to an annual survey by the American Association of Poison Control Centers, sodium hypochlorite, a component of home bleach, was the most often consumed caustic material. 4 Acid consumption, on the other hand, is more common in poorer nations owing to its widespread use in household cleaning products.3–6
Upper gastro-intestinal endoscopy (UGIE) is the most effective diagnostic tool for evaluating the severity of corrosive injuries. Using the presenting symptoms, signs, and routine blood investigations, the ‘Med-Tu’ chart was developed to grade the severity of corrosive ingestion and has shown acceptable predictive performance. As endoscopy is the gold standard for corrosive injury, this chart is helpful in remote places where there is lack of endoscopic equipment and expertise, especially in lower income countries. Our study aimed to validate a scale for grading the severity of corrosive injuries based on presenting symptoms, if it can be related to severity of injury.
Materials and methods
Our prospective observational study was conducted from October 2020 to June 2022. Approval was granted by both the Postgraduate Research Monitoring Committee (PGRMC) and the Institute Ethics Committee (JIP/IEC/2020/150), and was enrolled with the Trials Registry - India (CTRI) under the CTRI/2020/10/028247 identifier.
All patients of both genders aged >18, with a history of ingestion of corrosive substances, either accidental or intentional, were included. Patients presenting 48 h after ingestion, severely injured patients unfit for UGIE, those already with clinical or radiological signs of gastro-intestinal perforation, and those with supraglottic or epiglottic burns with oedema were excluded.
Our sample size was calculated with an expected agreement of the severity of corrosive ingestion between the Med-Tu chart and UGIE as 75% at a 5% level of significance and 80% power and was shown to be 90. Informed consent was taken from all study participants, and patients were given full freedom to withdraw from the study at any point. All patients were interviewed thoroughly, their physical examination findings recorded, and blood and radiological tests performed. Age, gender, degree of education, occupation, income, intent for ingestion of corrosive, nature and quantity of the corrosive consumed, and any associated comorbidity were recorded for each patient.
Symptoms and signs documented were asymptomatic, oropharyngeal/oral pain, epigastric pain, vomiting, and nausea, haematemesis, dysphagia, drooling of salivary secretion, melaena, respiratory distress, and vocal cord injury. Using the ‘Med-Tu chart’, the severity of the corrosive injury was determined, and patients’ injuries were classified as either low grade or high grade. 7 The Med-Tu chart takes into account three factors: drooling of saliva, total leucocyte count, and buccal mucosal lesions. 7
UGIE was performed within 48 h of ingestion of a corrosive substance. The endoscopic Zargar scoring system assessed the severity of the corrosive injury. Zargar grade 2B or above injuries on UGIE were considered high grades, whereas those of grade 2A or below were considered low grades. The Med-Tu chart findings were correlated with the findings on endoscopy.
All patients underwent a follow-up endoscopy either 6 weeks following the initial event or at the onset of symptoms suggestive of stricture of the gastrointestinal tract, whichever was earlier. The delayed sequelae were recorded as normal endoscopy, oesophageal stricture, or gastric stricture. Where a proximal oesophageal stricture prevented visualization of the distal upper gastro-intestinal tract, a radiological contrast scan was performed.
The data on categorical variables were expressed as frequency and percentages. The quantitative data were expressed as mean with standard deviation. The association between the socio-demographic factors, symptoms, and oral cavity examination with the endoscopic severity was assessed using the χ2 or Fisher's exact test. The diagnostic accuracy of the Med-Tu chart compared with endoscopic severity was assessed using sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV). The measure of agreement between Med-Tu chart severity grading and the UGIE severity grading was done using κ statistics. The comparison of leucocyte counts with endoscopic severity was done using an independent student t-test. Statistical analysis was conducted using SPSS 19.0 (IBM Corporation, Armonk, NY, USA) software.
Results
A total of 105 patients were screened, 92 meeting the inclusion criteria being included for the study. Two patients did not consent to participate.
The baseline characteristics of the study population were compared. The majority of patients were young females and belonged to a lower middle socio-economic class. The youngest was 18 years old, and the oldest 92. The average volume (SD) of corrosive ingested was 61.3 (±52.7) ml. Most (53/90, 58.8%) had consumed strong acids, the remainder alkali.
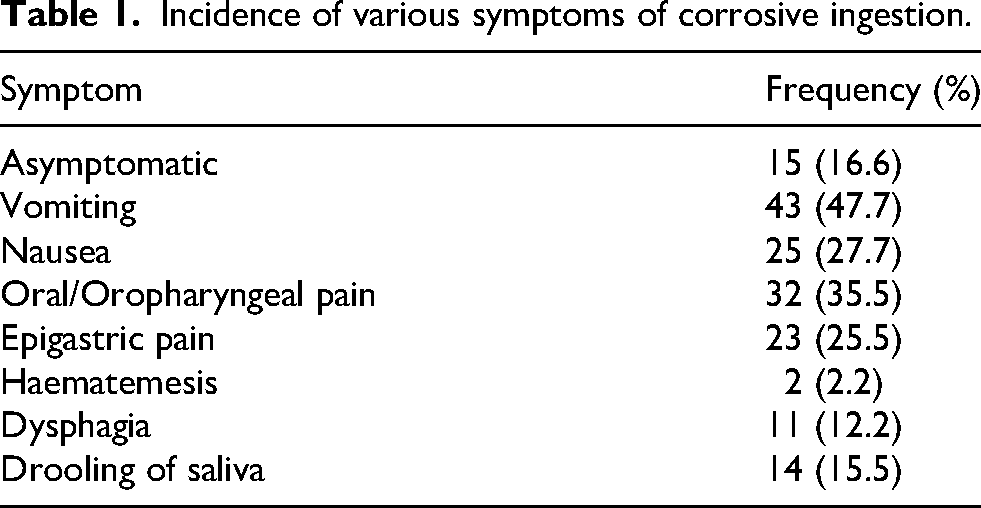
Symptoms were varied, depending on the strength and volume of corrosive consumed. Symptomatology is shown in Table 1. Whilst 67 (74.4%) had no lesions, 20 had grade 1 and three grade 2 lesions. The presence or absence of oral cavity lesions was predictive of the severity of corrosive ingestion (p-value < 0.001).
Incidence of various symptoms of corrosive ingestion.
The mean leucocyte count was 104.2 (±37.6) ×109/L. In high-grade ingestions, the mean leucocyte count was 136.0 (±34.3) ×109/L, whereas, in low-grade injuries, it was 97.9 (±35.1) ×109/L. On analysis using an independent student t-test, this was noted to be predictive of the severity of corrosive ingestion.
All patients’ injuries were graded on the Med-Tu chart, which graded 12 high-grade and 78 low-grade injuries. All patients with corrosive ingestion were subjected to endoscopy within 48 h of consumption. On comparing the Med-Tu chart with endoscopy findings, 12/15 high-grade lesions (as seen on gold standard endoscopy were detected as a high grade by the Med-Tu chart, whereas three cases of high-grade injury were falsely labelled as low grade by the Med-Tu chart.
On subgroup analysis for acid ingestion, 10/12 high-grade lesions (as seen on endoscopy) were detected as high grade by the Med-Tu chart, whereas two cases of high-grade injury were falsely labelled as low grade by the Med-Tu chart. In contrast, for alkali ingestions, 2/3 high-grade lesions (as seen on endoscopy) were detected as a high grade by the Med-Tu chart, whereas one was falsely labelled as a low grade by the Med-Tu chart.
The Med-Tu chart's diagnostic accuracy compared with the gold standard UGIE had 80% sensitivity, 100% specificity, 100% PPV and 96% NPV in detecting high-grade injuries (Table 2). The measure of agreement was 0.87 using kappa statistics. On subgroup analysis of acid ingestions, this chart had 83.3% sensitivity, 100% specificity, 100% PPV, and 95.3% NPV in detecting high-grade injuries. In contrast, the sensitivity, specificity, PPV, and NPV were 66%, 100%, 100%, and 97%, respectively, for detecting high-grade injuries in alkali-consumption patients. The measure of agreement was 0.88 for acid ingestions and 0.78 for alkali ingestions using κ statistics. All patients were followed up with a repeat endoscopy at 6 weeks. Some 5 (7.6%) had strictures following corrosive ingestion, but 25 were lost to follow-up. Strictures were found in 3/53 acid ingestions and 1/37 strong alkali (household cleaner).
Comparison of Med-Tu chart, upper gastro-intestinal endoscopy, and stricture development in patients with corrosive poisoning.

Discussion
Corrosive ingestion is, alas, quite common and may be catastrophic. Its management depends on the severity of injury and prognosis depends thereon. Drooling of saliva, burn over the buccal mucosa, and raised leucocyte counts were found to be independent predictors of high-grade injury. The Med-Tu chart first observes whether these signs exist. This determines which area of the chart that the patient falls into. A leucocytosis higher than the bold value in the chart shows that the patient is likely to have a high-grade (2b or more) injury. The misclassification rate was only 3.3%. The measure of agreement using κ statistics was 0.87. This is partly in agreement with a previous study, which noted that most corrosive ingestions (80%) occurred between the ages of 15 and 30 years. This variation is most probably due to the relatively smaller sample size. This population's mean (SD) age was 23.4 (±7.2) years. 3 Approximately 37% of cases were reported to occur in young adults aged 19–39 years, with a mean (SD) age of 44.6 (±20.9) years. 8 However, studies from the United States have shown that children are more affected there. 9 Most corrosive ingestion is noted in females.
In our study, the presence or absence of epigastric pain, dysphagia, drooling, and haematemesis were associated with the severity of corrosive ingestion (p < 0.05). We found that there are very few studies which have correlated symptoms with grade of injury. We found symptoms such as drooling of saliva, oral injuries, leucocytosis, and dysphagia as being correlated elsewhere with severity of injury.10,11 However, to the best of our knowledge, we could find no previous study which noted epigastric pain and haematemesis as predictors of high-grade injuries. Since the latter was seen in only two of our patients, a larger population study is required to use it as a predictor.
Children with cheek, lip, and oropharyngeal burns have a significant higher risk of having visceral burns, and dangerous ones at that, compared to children without, 11 as indeed we too found. Leucocytosis was inconsistently found predictive of severe injury following corrosive ingestion,7,8 whilst we found a statistical significance.
Our study has a few limitations: we did not include children, who form a significant proportion of cases of corrosive ingestion. Hence, we cannot confirm the Med-Tu chart as useful in this group. However, strong alkali is known for its notoriety elsewhere. Multiple trained surgeons assessed the endoscopic severity. Though a standardized classification system (Zargar grading) was used in our study, inter-observation variation exists in the interpretation of endoscopic findings we used. Only 72% of patients underwent follow-up endoscopy, owing to restrictions during the COVID pandemic.
Conclusion
We conclude that the Med-Tu chart has an acceptable diagnostic accuracy in detecting the severity of overall corrosive ingestion in adults with good agreement for acid and a fair deal for alkali ingestion compared to the gold standard UGIE. It is recommended as an initial tool to assess the severity of corrosive injuries, particularly acidic. However, it needs further studies for its application in alkaline injuries, and in children. Most corrosive ingestion was suicidal in intent; a good social support system is mandatory to help and reduce the number of victims of suicidal poisoning.
Footnotes
Acknowledgments
NONE
ORCID iDs
Ethics approval and patient consent to participate
The above study was approved by Institute Ethics Committee.
Patient consent for publication
Consent was taken directly from the patients.
Role of the authors
USK contributed to conceptualization, methodology, and software. YYK contributed to data curation and writing – original draft preparation. USK contributed to supervision. HKT contributed to software and validation. OS contributed to writing – reviewing and editing.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Clinical trial registry number
CTRI/2020/10/028247
Institute ethics committee
(JIP/IEC/2020/150).