
Abstract
Cleft lip and/or palate (CLP) is among the most common congenital anomalies worldwide. While primary surgical repair is essential, comprehensive CLP care also depends on equally important secondary services such as speech therapy, audiologic support, orthodontic care, and revision surgeries. In many low- and middle-income countries (LMICs), these services remain limited or inaccessible, resulting in suboptimal long-term functional, aesthetic, and psychosocial outcomes. Our narrative review searched across PubMed and Embase databases to identify the availability, delivery models, and outcomes of secondary CLP services in LMICs. We found 17 relevant studies and mapped existing evidence, identified key gaps, and explored barriers related to workforce shortages, training, infrastructure, and financial constraints. Our findings highlight the urgent need to strengthen multidisciplinary CLP care pathways beyond primary surgery. Investments in sustainable local capacity, tele-health enabled service models, task-sharing, and community-based interventions are crucial to achieving equitable, high-quality CLP outcomes in resource-limited settings.
Keywords
Introduction
Cleft lip and/or palate (CLP) is among the most common congenital anomalies of the face, affecting approximately 1 in every 500–700 live births. 1 CLP compromises nearly all facial functions except vision; impacting feeding, dentition, speech, and hearing. Optimal management requires not only surgery, but speech therapy, hearing aid, and management of otitis, orthodontic care, psychological support, and basic child care, including secondary surgery if required. 2
In low- and middle-income countries (LMICs), access to secondary CLP care is often non-existent, constrained by insufficient human resources, infrastructural limitations, and economic barriers, leading to suboptimal long-term outcome. 3 Our narrative review aims to examine the extent and nature of these failings and to explore potential solutions.
Methods
A systematic literature search was performed in PubMed, and Embase electronic databases using the following keywords: Cleft conditions (cleft lip, cleft palate), Secondary care services (secondary care, speech therapy, speech-language pathology), Audiology (hearing loss, ENT, otolaryngology), Secondary surgery, Revision surgery, Access and disparity-related terms (health services accessibility, barriers, disparities, inequality, access, availability), Health services needs and demand, Geographical/LMIC indicators (developing countries, low- and middle-income countries, LMIC, Africa, Asia, Latin America, Sub-Saharan Africa, South Asia, Southeast Asia).
Inclusion criteria were as follows: Original article/Opinion/Editorial/Review on Cleft Lip, Cleft Palate, secondary surgery, revision surgery, secondary care, speech therapy, speech-language pathology, audiology, hearing loss,Health Services Accessibility, barriers/disparities/inequality/access/availability/health services needs and demand; in Developing Countries/low- and middle-income countries/LMIC/Africa/Asia/Latin America/Sub-Saharan Africa/South Asia/Southeast Asia/Latin America.
Exclusion criteria were papers from High Income Countries, primary surgical treatment of cleft lip and palate, case reports.
Results
We systematically searched PubMed and Embase electronic databases from 1991 to April 2025, and also searched the reference lists of included studies.
A total of 104 articles were retrieved but finally, only 17 studies were included in the qualitative analysis.
Out of these 17, published between 2004 and 2025, 3 were from Uganda and international cohort, 2 from India, Nepal, Nigeria, Laos, and 1 each from Bangladesh, Thailand and the near East. 16 articles were observational studies while one was an interventional study.4–20 Data extracted included the following: Author (Year), Country/ Region, Study Type, Post-Surgical Barrier(s) and Key Findings (Table 1). Table 1 also highlights that post-cleft surgical care in LMICs is impeded by a recurring constellation of barriers.
Barriers to post-cleft surgery services in LMICs.
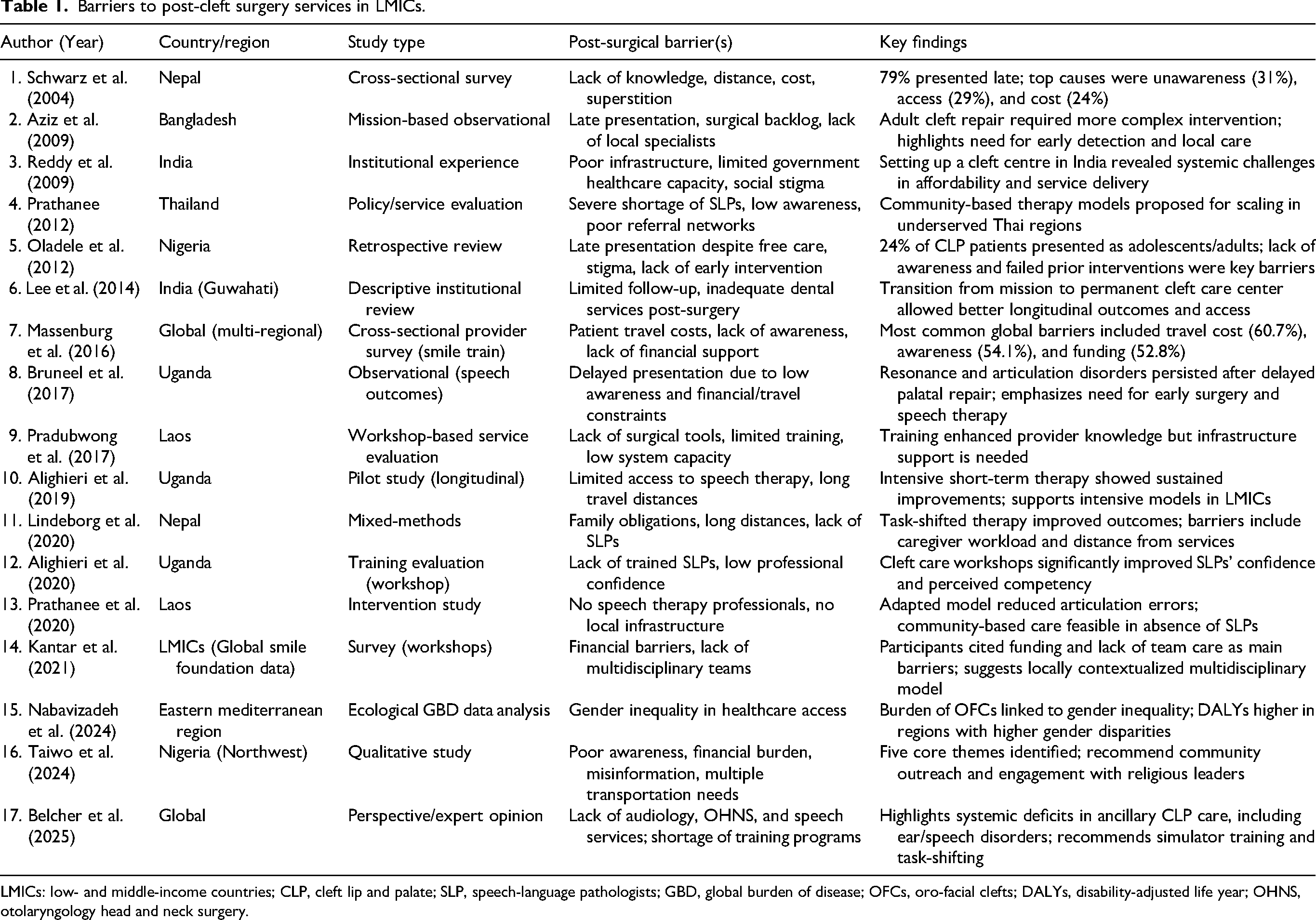
LMICs: low- and middle-income countries; CLP, cleft lip and palate; SLP, speech-language pathologists; GBD, global burden of disease; OFCs, oro-facial clefts; DALYs, disability-adjusted life year; OHNS, otolaryngology head and neck surgery.
A narrative synthesis was undertaken and the thematic synthesis of these 17 studies showed multiple, interlinked barriers that impede access to comprehensive secondary cleft care across LMICs.The following themes consistently emerged:
High out-of-pocket costs, lack of financial support, and income loss due to travel deter timely access to care. Long distances, poor infrastructure, and caregiver constraints limit access to surgical and rehabilitative services. A critical lack of speech-language therapists and audiologists hampers post-surgical rehabilitation. Low health literacy, misinformation, stigma, and late presentation due to socio-cultural beliefs remain widespread. Weak referral systems, lack of institutional support, inadequate equipment, and logistical hurdles obstruct continuity of care. Gender-based disparities affect access and outcomes, particularly for female patients in certain regions. Reports of successful task-shifting, community-based training, permanent care centers, and media-led awareness strategies.
Risk of bias in included studies.
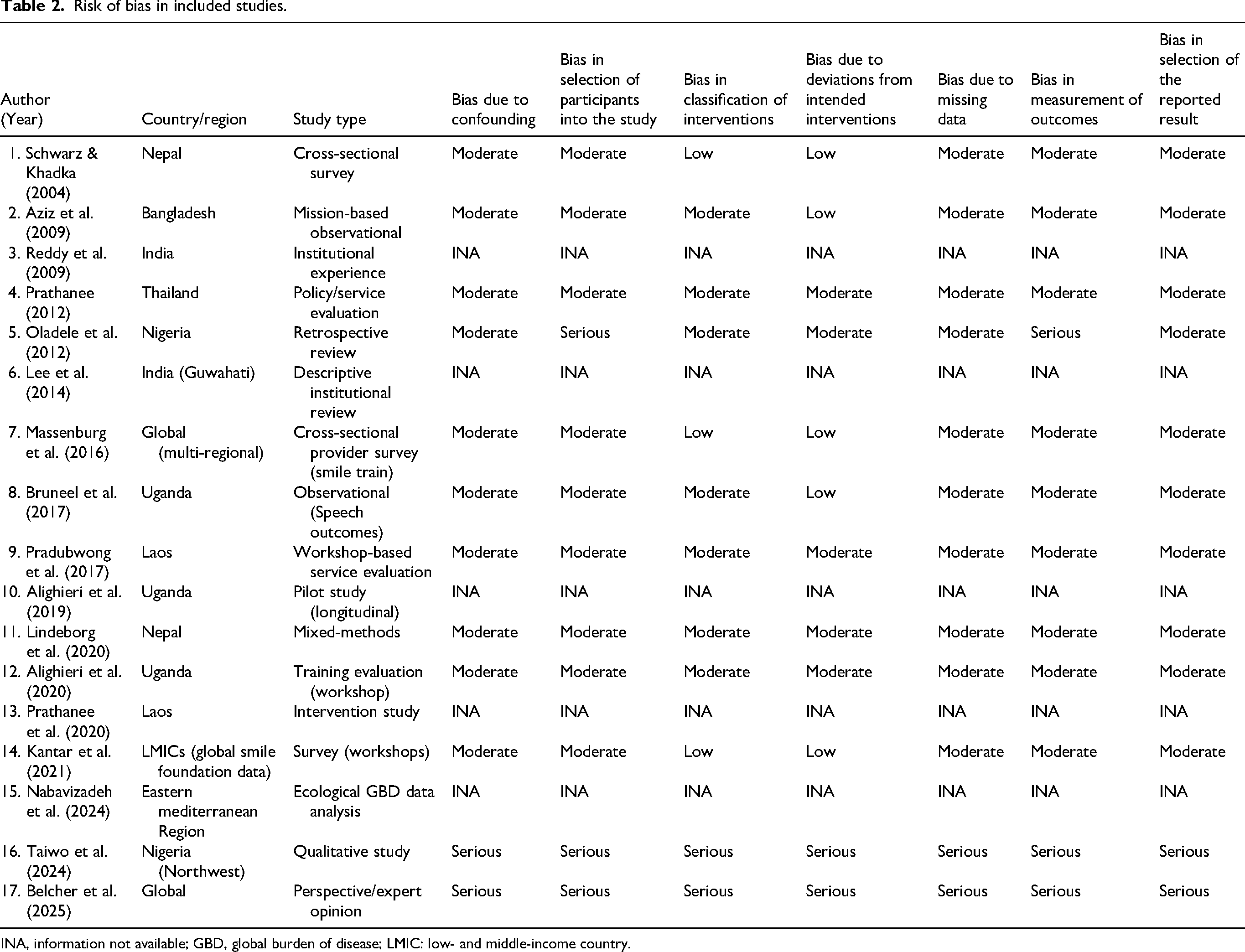
INA, information not available; GBD, global burden of disease; LMIC: low- and middle-income country.
Publication bias was not assessed because of the substantial clinical and methodological heterogeneity of selected studies.
Assessment of reliability, validity, and level of evidence was not undertaken as this review was designed to map the existing literature descriptively rather than critically appraise the methodological quality of the included studies.
Statistical analysis was not performed as the qualitative data best answered the research question.
Discussion
Our narrative review underlines that equitable secondary CLP care in LMICs remains largely neglected. Despite progress in primary repair, access to essential secondary interventionsspeech therapy, audiology, and revision surgery, remains severely constrained by the factors previously mentioned, which frequently reinforce one another, leaving many children with preventable speech disorders, hearing loss, malnutrition, and psychosocial difficulties even after successful primary repair.
A key contribution of this review is its focus on the “forgotten part” of cleft care. Cleft management does not end in the operating room; untreated Eustachian tube dysfunction, recurrent otitis media, conductive and sensorineural hearing loss, hypernasality (up to 30%), and severe articulation disorders (up to 94%) all may nullify the benefits of excellent surgery.22–24
Yet LMICs face stark personnel gaps; there is <1 ENT surgeon per 100,000 people, and in many African countries <1 SLP per 4 million.25–27 While 65%–70% of children in high-resource settings receive early speech therapy, such services are rare or absent across most LMICs.These challenges are even more pronounced in languages that use click consonants, making timely and sustained speech therapy especially essential. With nearly 250,000 new CLP cases annually, the cumulative burden is profound.28,29
Although past studies have noted individual barriers (Table 1), none have synthesized the full scope of systemic obstacles to secondary care across LMICs. Our review integrates evidence from Africa, Asia, and Latin America to show that these challenges are not isolated but structurally patterned, and rooted in broader socioeconomic inequities. We deliberately emphasized secondary care, chronically overlooked in policy and literature, despite its central importance for intelligible speech and functional hearing.
Our review also highlights innovative, context-adapted strategies such as task-shifted speech therapy delivered by trained local caregivers, 14 community-based and simulator-based training for ENT and speech care,16,20 and transitioning from mission-based models to permanent care centers, which tangibly strengthens long-term outcomes. 9 Locally driven awareness programs, such as partnerships with religious leaders and radio campaigns, also demonstrate promise in prompting timely care-seeking. 20
Our review has several limitations. Heterogeneity in study design, geography, and methodology limits quantitative synthesis. The predominance of English-language publications may have introduced language bias, and most studies prioritized provider perspectives rather than patient or caregiver experiences. Many also showed moderate to serious risk of bias (Table 2), and few longitudinal studies assessed long-term outcomes of proposed interventions or reforms.
Even with these limitations, the striking consistency of findings across diverse contexts points to common systemic failures in secondary cleft care. The emergence of low-cost, scalable solutions, such as local caregiver-led speech therapy, community-based outreach, simplified orthodontic devices, and locally produced hearing aids, across multiple countries is encouraging. This is where LMIC health systems may intervene most effectively.
Future research should focus on patient-reported experiences, especially among rural and marginalized families, and evaluate the scalability and cost-effectiveness of care models such as task-shifting, teletherapy, and mobile outreach. Region-specific registries and outcome-tracking mechanisms are needed, alongside workforce mapping for SLPs and ENT specialists to inform strategic investment. Finally, implementation research is essential to transition from fragmented, mission-based programs to sustainable, locally integrated care models.
Conclusion
Secondary cleft care in LMICs requires sustained, system-level reform rather than episodic “breeze-in, breeze-out” surgical missions. Our review shows that persistent gaps in speech therapy, audiology, and follow-up care continue to undermine functional outcomes for thousands of children. Comprehensive cleft care must include speech therapy, audiological support, and revision surgery, and these must be embedded within Cleft Lip and Palate care frameworks in LMICs to ensure meaningful, lifelong impact. Without this commitment, LMIC cleft care will continue to celebrate only surgical beginnings while neglecting the forgotten second half of the smile.
Footnotes
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.