
Abstract
We report two such cases. Case 1: A 30-year-old male presented with right forearm swelling and pain; examination revealed a non-mobile, fluctuant intramuscular swelling. Case 2: A 30-year-old female had a 3-month history of midline chest pain with a mobile, fluctuant swelling over the xiphisternum. In both cases, aspirated pus showed numerous pus cells with few Gram-negative bacilli. Culture revealed non-lactose fermenting, smooth convex colonies identified as Salmonella Typhi by biochemical tests, Vitek 2 (bioMérieux), and serology. The isolates were susceptible to ceftriaxone, ciprofloxacin, azithromycin, cotrimoxazole, and ampicillin, but resistant to chloramphenicol. Both patients were immunocompetent, with no history of trauma, diabetes, or haemoglobinopathy, and responded well to antibiotic therapy. These cases highlight the need for clinical awareness of atypical presentations of S. Typhi osteomyelitis and the importance of timely diagnosis in endemic regions.
Introduction
Enteric fever, caused by typhoidal Salmonellae (serotype Typhi and Paratyphi), is a significant global health concern, causing 11–20 million infections annually and resulting in 128,000–161,000 deaths, particularly impacting low-income countries. 1 The extra-intestinal complications of Salmonella Typhi infection can affect various systems including the central nervous (3–5%), cardiovascular (1–5%), pulmonary (1–6%), bone, joints, and musculoskeletal (<1%), hepatobiliary (1–26%), genitourinary (<1%), amongst others. 2 These presentations are particularly seen in individuals with specific risk factors such as haemoglobinopathies, joint trauma, surgery, connective tissue disorders, lymphoma, diabetes, alcoholism, immunosuppression, or advanced age. 3
Though uncommon, extra-intestinal S. Typhi infections may be noted in immuno-competent individuals without identifiable risk factors. 4 In a systematic review, 2 47.76% cases of Salmonella osteomyelitis occurred in such without common risk factors. The commonly involved sites were the vertebrae, femur, and tibia.
Case series
Case 1
A 30-year old male student, previously healthy, presented at an out-patient clinic of the orthopaedics department with constant pain and swelling of the right forearm persisting for the past 30 days. The swelling was not progressive in size. Additionally, he reported experiencing loss of appetite and weight loss over the previous two weeks. He denied any history of trauma or recent episode of gastroenteritis or bloodstream infection. He was non-diabetic and had no history of alcohol misuse.
On examination, a 6 × 6 cm2 non-mobile intramuscular swelling and a 3 × 3 cm2 bony hard swelling were found over the ulnar aspect of the right proximal forearm. Mobility of the swelling was restricted in both planes, although the range of elbow movement was full and free. The skin appeared intact, with mild erythema and tenderness.
Laboratory investigations revealed a normal full blood count and his erythrocyte sedimentation rate and C-reactive protein levels elevated at 65 mm/h and 12 mg/L, respectively. He had A+ve, Rh−ve blood group, without any irregular antibodies detected.
On radiography, a periosteal reaction was present near the right ulnar shaft. Ultrasound scan revealed a small fluid collection of 1.2 × 3.5 cm2 in size in the intra-muscular plane overlying the shaft of right ulna with intact bony cortex. A contrast-enhanced magnetic resonance imaging scan showed a lytic lesion with oedema as shown in (Fig. 1).

Contrast-enhanced magnetic resonance imaging image showing a lytic lesion in medial aspect of ulna with periosteal reaction and medullary marrow STIR (Short Tau Inversion Recovery) hyperintensity.
Pus was aspirated under aseptic precautions and inoculated on 5% sheep blood and MacConkey agar as well as in brain–heart infusion broth for enrichment and incubated at 37 °C. A Gram-stained smear showed 15–20 pus cells and 1–3 red blood cells per oil immersion field with no organism seen. After 48 h of incubation, however, typical colonies of Salmonella spp. were observed on the plated media (Fig. 2).
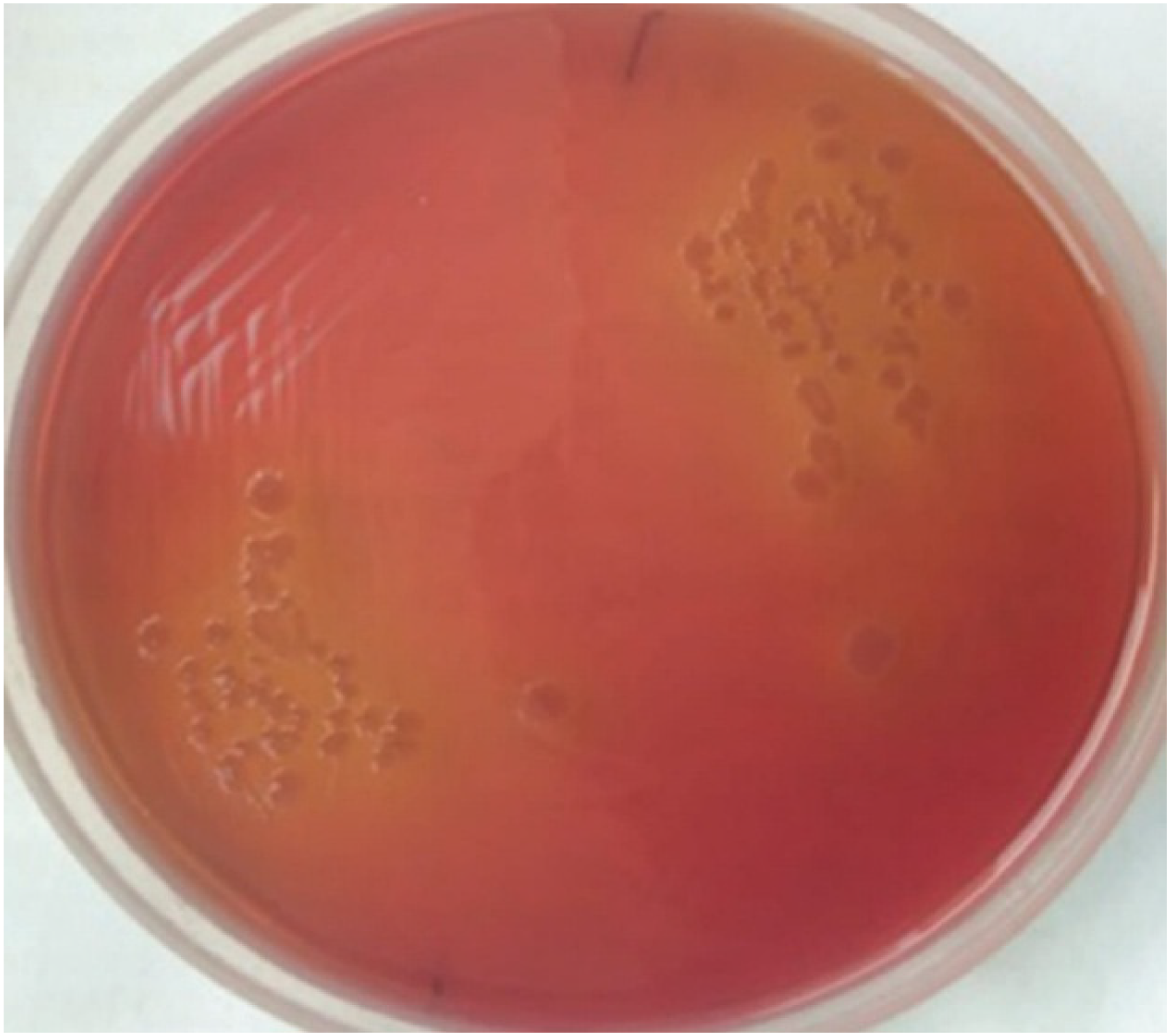
Non-lactose fermenting colony grown on MacConkey.
The isolate was identified by conventional biochemical tests and automated Vitek 2 compact (bioMérieux, Marcy-l'Étoile, France) as S. Typhi and confirmed by serotyping. Antimicrobial susceptibility testing by disc diffusion test and minimum inhibitory concentrations were determined by Vitek 2 compact. 5 The isolate was susceptible to ceftriaxone, ciprofloxacin, azithromycin, cotrimoxazole, and ampicillin, but resistant to chloramphenicol. We used cefixime 400 mg and ciprofloxacin 500 mg bd for 14 days.
Stool and urine specimens were cultured to assess carrier state, which was subsequently excluded. No pre-disposing risk factors were revealed. The family history was unremarkable; no haemoglobinopathy was detected on electrophoresis.
Chronic osteomyelitis of the right ulna was diagnosed; decompression and saucerisation of the ulna, followed by bony reconstruction, were performed under axillary block. On the third day, he could be discharged, and on follow-up after a week showed an improved range of motion and was pain free.
Case 2
A 30-year old female presented with a swelling over the xiphisternum measuring 3 × 3 cm2 in size and mild midline chest pain persisting for 3 months. She denied any history of trauma nor of recent gastro-enteritis. On examination, a mobile fluctuant intramuscular swelling, 3 × 3 cm2 in size was observed over the xiphisternum. The skin appeared intact, with mild erythema, tenderness, and constant tenderness without any exacerbating factors.
A non-contrast computed tomography scan of the chest showed a soft tissue density mass in the midline anterior to the xiphisternum. This displayed an ill-defined irregular margin, surrounding fat stranding, and a tiny focus of calcification, with no obvious hypodense area of necrosis. Additionally, erosion of the underlying xiphisternum, bone, and the costosternal junction of the left sixth rib, along with mild thickening of the adjacent pleuro-pericardium, was seen.
Incision and drainage was performed under anaesthesia, and pus was sent for culture and susceptibility testing, being inoculated as described earlier. The Gram-stained smear showed a field full of pus cells with few Gram-negative bacilli. Characteristic colonies were observed and identified as S. Typhi, as in the first case. Identification was confirmed by serotyping. The isolate was susceptible to ceftriaxone, ciprofloxacin, azithromycin, cotrimoxazole, and ampicillin, and resistant to chloramphenicol.
Carrier state and haemoglobinopathies were ruled out. Antimicrobial therapy was initiated with cefixime 400 mg bd and azithromycin 500 mg od for 14 days, after which the wound had completely healed with complete resolution of symptoms.
Discussion
S. Typhi and Salmonella Paratyphi A and B are facultative intra-cellular organisms causing enteric fever, not uncommon in low-income countries. 6 Salmonella osteomyelitis was first reported in 1876, 6 and is the causative organism in 0.5–2% cases of osteomyelitis, 7 accounting for as few as 0.8% of all Salmonella infections, 8 with the four most common serotypes being S. Typhimurium, S. Enteritidis, S. Enterica subsp. arizonae and S. Typhi. 9
The organism exploits the reticuloendothelial system (RES) for longer-term persistence and systemic dissemination. 10 Within the RES, Salmonellae survive and replicate in macrophage phagosomes, 11 using various virulence factors to manipulate host cell pathways, suppress oxidative killing, and inhibit lysosome fusion. 12 This results in persistence of infection, the organism remaining latent, evading host immunity, and later being able to re-activate. The bone marrow serves both as a portal and reservoir for infection. Complement system and impaired opsonisation have also been suggested to play a role.13,14
Both our patients were young and apparently healthy before their illness. They had no associated co-morbidity, nor any immuno-suppressive condition. There are no specific clinical or characteristic radiological features of Salmonella osteomyelitis. The proximal humerus and distal femur are the most commonly involved sites. Sluggish blood flow to the metaphysis of bones pre-dispose as fertile grounds for Salmonella osteomyelitis. 15
Conclusion
In endemic regions, S. Typhi should be ruled out as a cause of non-healing musculoskeletal infection in low-income countries irrespective of the patient's immune status, pre-disposing risk factors or any reported recent episode of gastroenteritis in the patient.
Footnotes
Consent to participate
The authors confirm that they have secured all necessary patient consent forms. In these forms, the patient(s) have provided consent for their images and other clinical information to be published in the journal. The patients are aware that their names and initials will not be disclosed, and all reasonable measures will be taken to protect their identity, though complete anonymity cannot be ensured.
Author contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.